Download to read offline

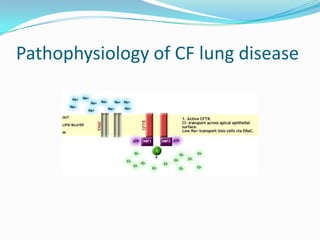

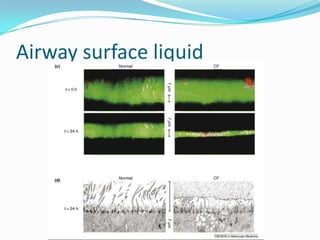








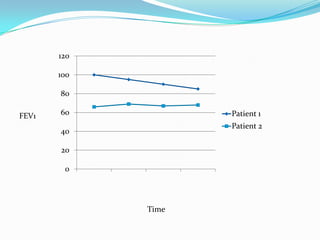







The document reviews cystic fibrosis (CF) lung disease, detailing its pathophysiology, chronic therapies, and the importance of tracking lung function through FEV1 measurements. Key treatments discussed include hypertonic saline, inhaled mannitol, DNase, and antibiotics, alongside airway clearance methods like chest physiotherapy and exercise. Emphasis is placed on regular monitoring and maintaining a healthy weight to manage the progressive nature of CF lung disease.



![Cystic fibrosis[1]](https://cdn.slidesharecdn.com/ss_thumbnails/cysticfibrosis1-130307125149-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)































































