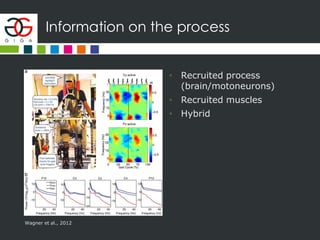
The document discusses the use of brain-computer interfaces (BCIs) to facilitate communication for individuals with disorders of consciousness (DoC). It outlines the identification of populations, biomarkers, modeling techniques, and various applications such as rehabilitation. The document emphasizes the potential of BCIs to enhance quality of life, while also recognizing challenges such as misdiagnosis and the need for proper statistical validation.
























































![ANIMAL_CELL_,_TISSUE_AND_ORGAN_CULTURE[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/animalcelltissueandorganculture1-260204172026-4462b440-thumbnail.jpg?width=640&height=640&fit=bounds)









![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)



