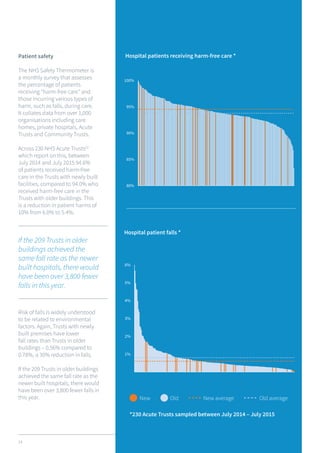
This document discusses how investment in healthcare real estate can contribute to improved patient care and staff wellbeing. It finds that services provided from new healthcare premises are three to four times more likely to receive an "Outstanding" rating from regulators. Modern facilities are also safer for patients, with 30% lower fall rates and 10% lower overall patient harm in new hospitals and care homes. Continuous investment in flexible, future-proof buildings is critical to ensure these benefits are realized across the entire national healthcare portfolio. Doing so would benefit both patients and healthcare professionals.