BONE BIOCHEMISTRY &HOMEOSTATIC
REGULATION OF FLUID & ELECTROLYTES
Dr. Window(MBBS-Mw)
2.
Bone biochemistry
• Bonehas an obvious mechanical function as well as serving an equally
important role as a mineral reservoir.
• Bone is in continuous state of flux i.e. its internal and external structures
change from time to time in concert with normal variation in mechanical
function and mineral exchange.
3.
Bone biochemistry ct’d
•The metabolic bone disorders are conditions in which generalized skeletal
abnormalities result from disruption of complex interactive system.
Alteration in mineral ion concentration
↓
Modify hormones and local factors
↓
Controls cellular activity
↓
Modulates bone structure and composition
5.
SOME OF THECHEMICAL COMPONENTS OF A
BONE
• Calcium
• Potassium
• Phosphorus
• Magnesium
6.
1. METABOLISM OFCALCIUM & FUNCTIONS
• Calcium is essential for myocardial contraction.
• Decrease in ionized calcium concentration in blood can cause
neuromuscular irritability, which may become clinically apparent as
irregular muscle spasms, called tetany.
• Parathyroid hormone secretion in the blood is stimulated by a
decrease in ionized calcium and conversely, parathyroid hormone is
stopped by an increase in ionized calcium.
7.
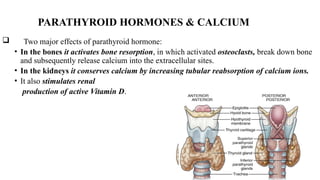
PARATHYROID HORMONES &CALCIUM
Two major effects of parathyroid hormone:
• In the bones it activates bone resorption, in which activated osteoclasts, break down bone
and subsequently release calcium into the extracellular sites.
• In the kidneys it conserves calcium by increasing tubular reabsorption of calcium ions.
• It also stimulates renal
production of active Vitamin D.
8.
NB. Osteoclasts’ mainfunction is critical in the maintenance, repair,
and remodeling of bones of the vertebral skeleton
9.
Calcium and VitaminD
• Vitamin D3, a cholecalciferol, is obtained from diet and is metabolized by the
body with an exposure to sunlight.
• Vitamin D3 is then converted in the liver to 25-hydroxycholecalciferol, which is an
inactive form,
• Later in the kidney it is hydroxylated to form 1,25-dihydroxycholecalciferol (an
active form).
• The active form of Vitamin D will increase calcium absorption in the intestines
and enhances the effects of parathyroid hormone on bone resorption.
10.
Metabolism of Calcium
CalciumReference Ranges
• Calcium Total for adults: 2.15-2.50 mmol/l, for children: 2.15-2.65
mmol/l
• Calcium ionized for adults:1.16-1.32 mol/l, Calcium ionized for
children: 1.20-1.48 mmol/l
11.
HYPERCALCEMIA: (excessof calcium in the plasma), is dangerous
when severe.
• Hypercalcemia crisis has a mortality rate as high as 50% if not treated
properly.
CAUSES: Multiple myeloma, vit D overdose
MANAGEMENT:
• Calcitonin is administered to lower serum calcium levels.
• Bisphosphonates to inhibit osteoclasts, chemotherapy for cancer
12.
METABOLISM OF CALCIUM
HYPOCALCEMIA:
•Clinical features are of neuromuscular excitability;
• ECG-long QT interval
• Cramps/peri-oral numbness
• Seizures
CAUSES: CKD (vit D not hydroxylated), Blood transfusion, hypoparathyroidism
(thyroid surgery), acute pancreatitis, acute rhabdomyolysis
MGT; calcium gluconate 10ml of 10% over 30 mins
13.
2. METABOLISM OFPHOSPHORUS
• Phosphorus is found everywhere in living cells, and it participates in most
important biochemical processes.
• The genetic materials DNA, RNA are complex phosphodiesters.
• Most co-enzymes are esters of phosphoric or pyrophosphoric acid and the most
important reservoirs of biochemical energy e.g ATP (Adenosine
Triphosphate), Creatinine phosphate, phosphoenolpyruvate, etc
• Phosphate is absorbed in the intestines from dietary sources, released from
cells into blood, and loss from the bones.
14.
Relationships between phosphatesand other organs/minerals
.Phosphate and the kidneys;
• When there is higher levels of phosphate there is an increase in excretion, when the
levels are low, the tubular reabsorption is expected to increase.
Phosphorus and vitamin D;
• Vitamin D facilitates both phosphate absorption in the intestines and phosphate
reabsorption in the kidneys.
.
15.
Phosphorus andparathyroid hormone;
• Parathyroid hormone lowers the concentration by increasing renal
excretion of phosphate
16.
Metabolism of phosphorus
Hypophosphatemia;(<0.4mmol/L)
CLINICAL FEATURES: lethargy/weakness, arrythmias.
MGT: oral or iv phosphate replacement.
HYPERPHOSPHATEMIA:
COMMON CAUSE is renal failure
CLINICAL FEATURES: muscle cramps, weak bones
MGT: restrict dietary phosphate intake, dialysis.
17.
3. METABOLISM OFMAGNESIUM.
• Magnesium is the fourth most abundant cation in the body and second
most abundant intracellular ion.
• The average body weight of 70 kg has 1 mole (24 g) of Mg,
• 56 % of the magnesium is found in the bones, 46 % in the muscles
and the remaining is found in other organs e.g. serum and blood cells.
18.
• Magnesium worksas a co-factor;
-of more than 300 enzymes, including those enzymes important in
hydrolysis
-transcellular ion transport
-neuromuscular transmission
-Synthesis of carbohydrates, protein, lipids
-nucleic acids and release of and response to certain hormones.
19.
Metabolism of Magnesium.
•The serum levels of magnesium is 0.63 – 1.0 mmol/l or 1.2-2.1 mEq/l
• Urine levels should range from 3.00 – 5.00 mmol/ 24 hours
20.
Magnesium and kidneyfunctions:
• 25-30% 0f magnesium is reabsorbed by the proximal convoluted
tubule,
• The loop of Henle is the major regulatory site where 50-60% of
filtered magnesium is reabsorbed in the ascending limb.
• Slight excesses of magnesium in serum are rapidly excreted by the
kidneys.
21.
Metabolism of Magnesium.
Magnesiumand Parathyroid hormone;
• Parathyroid hormone increases the renal reabsorption of
magnesium and enhances the absorption of magnesium in the
intestines.
• The effects of parathyroid hormone on kidney is opposed by
the effects of other hormones such as aldosterone and
thyroxine,
• These hormones will reduce the reabsorption of Mg by
kidneys hence they will increase the renal excretion of
Magnesium.
22.
Metabolism of Magnesium.
•Causes of hypomagnesemia
-Reduced intake
-Decreased
absorption
-Increased excretion Renal/Endocrinological
-Increased
excretion –drug induced i.e. diuretic
-Excess lactation and in pregnancy
3. FLUID ANDELECTROLYTES IMBALANCE
• Fluid and electrolyte balance is a dynamic process that is crucial for
life.
• It plays an important role in homeostasis
• Imbalance may result from many factors and it is associated with the
illness
Fluids and ElectrolytesImbalance
• Electrolytes are chemical substances that release cations and anions
when they are dissolved in water.
• Two categories:
• Cations (positively charged); sodium, potassium, magnesium and hydrogen
ions
• Anions (negatively charged): chloride, bicarbonate, phosphates, sulfate
30.
• Osmosis: fluidshifts through the membrane from the region of low
solute concentration until the solution are of equal concentration.
• Diffusion: substance move from an area of higher concentration to an
area of lower concentration.
31.
Fluids and ElectrolytesImbalance
HOW DO WE LOSE/GAIN WATER? Routes of gains and loses
-kidney
-skin
-lungs
-GIT
Fluid volume disturbances
Hypovolemia: fluid volume deficit
Hypervolemia: fluid volume excess
32.
Fluids and ElectrolytesImbalance
SODIUM
• It is the most abundant cation in the extra-cellular fluid,
representing 90% of all extracellular cations and largely determines
the osmolarity of plasma.
• A small amount of sodium can diffuse through the membrane, and the
two sides would eventually reach equilibrium. .
33.
• BUT Activetransport system helps to prevent sodium from reaching
the equilibrium, e.g ATPase ion pump,
• In this system, 3 sodium ions are moved out of the cell in exchange for
2 potassium ions which will be moved into the cell as ATP is changed
to ADP
34.
REGULATION OF SODIUM
•The levels of plasma sodium concentration remains in normal range due to the
following mechanisms:
• NaK-ATPase ion pump, when there is low sodium levels, a lot of sodium ions are
expected to be moved from cells or through intake and excretion of water.
• The excretion of water, largely affected by ADH release in response to changes in
either blood volume or osmolarity.
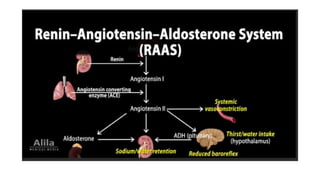
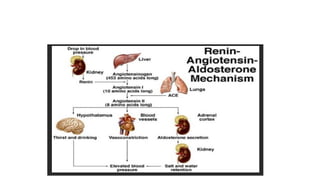
• The blood volume status, which affect sodium through aldosterone, angiotensin
and atrial natriuretic peptides.
37.
Fluids and ElectrolytesImbalance
• Normally, 60-600 of filtered sodium is reabsorbed in the proximal tubule and
electroneutrality is maintained by either chloride reabsorption or hydrogen ion
secretion.
• Some of the sodium is also reabsorbed in the loop and distal tubule and exchanged
for potassium in the connecting segment and cortical collecting tubule.
• Two major metabolic imbalances/disorders of sodium that may occur are:
hyponatremia or hypernatremia
38.
Fluids and ElectrolytesImbalance
Hyponatremia (sodium less than 135mEq/L)
• This metabolic disorder occurs when the levels of sodium are lower than
the normal levels.
• osmolarity hyponatremia is divided into three:
• -hyponatremia with low osmolarity
• -hyponatremia with normal osmolarity
• -hyponatremia with high osmolarity
39.
Fluids and ElectrolytesImbalance
Causes of hyponatremia
• Excessive loss of sodium
-this could be loss from the kidneys, due to diuretic therapy or renal diseases, adrenal insufficiency
-loss from skin through sweating, burns and even widespread dermatitis
-loss from the gut by vomiting, dairrhea, fistula or intestinal obstruction
• Inadequate intake
-sodium depletion will occur whenever intake is inadequate to balance excessive lossess,
inadequate intake alone is rarely a cause depletion.
40.
Fluids and ElectrolytesImbalance
Clinical features
• -weakness, confusion, coma
• -weight loss, hypotension, oliguria
• -decreased intraocular pressure
• -decreased skin turgor
41.
Fluids and ElectrolytesImbalance
Management of hyponatremia
• Sodium replacement
-administration of sodium by mouth
-lactated ringers solution (0.9% sodium chloride).
• Replacement of Serum Sodium must not increase greater than 12meq/l in 24hrs to
avoid neurological damages e.g Central pontine myelinolysis (osmotic demyelination)
• NB; if the patient is not dehydrated, or even volume-overloaded, restrict water to
improve the Na+
42.
Hypernatremia (sodiumlevels more than 145mEq/L)
• Hypernatremia, this condition is frequently found in elderly people, as a
result of inadequate water intake, or could be iatrogenic (in hospital
setting).
Causes of hypernatremia
• -excess water loss; e.g. due to Diabetes mellitus (DKA, HHS), renal
tubular disorder, prolonged diarrhea, profuse sweating, severe burns,
decreased water intake, mental impairment.
43.
Fluids and ElectrolytesImbalance
• Symptoms of hypernatremia
• Due to hyperosmolar state:
-altered mental status, lethargy, irritability, restlessness, seizures, muscle
twitching, hyperreflexia, fever, nausea or vomiting, difficult respiratory and
increased thirst.
• Management/treatment
-give water orally if possible
-or administer 5% dextrose
If shocked use Na+Cl-
44.
Potassium
• Itis a major intracellular cation in the body, the concentration is of
20 times greater inside the cells than outside.
• only 2% of potassium circulates in the plasma
• Functions of Potassium:
• Regulation of neuromuscular excitability; contraction of the heart and
skeletal muscles,
• maintenance of intracellular fluid volume and hydrogen concentration.
45.
Regulation of potassium
•In the kidneys, proximal tubules reabsorb nearly all potassium.
• Under the influence of aldosterone, additional potassium is secreted into
the urine in exchange for sodium in both the distal tubules and the
collecting ducts.
NB Potassium may accumulate to toxic levels due to renal failure
• Potassium does not reach to equilibrium between the intracellular and
extracellular levels which is achieved due to NaK-ATPase ion pump.
46.
Fluids and ElectrolytesImbalance
Factors that influences the NaKATPase pump:
• -in conditions like hypoxia, hypomagnesaemia or digoxin overdose;
there is an inhibition of NaK-ATPase ion pump causing potassium
loss.
• -insulin promotes acute entry of potassium ions into skeletal muscles
and liver by increasing NaK-ATPase activity.
• -catecholamines such as epinephrine (beta stimulator), promote
cellular entry of potassium whereas propranolol (beta blocker)
impairs cellular entry.
47.
Hypokalemia (plasmaconcentration below 3.5mEq/L)
Causes of hypokalemia
-Gastrointestinal loss; vomiting, diarrhea, gastric suction, intestinal tumor,
malabsorption and large doses of laxatives.
-Renal loss,: use of thiazides, nephritis, renal tubular acidosis,
hypomagnesaemia
-Cellular shift due to alkalosis and insulin overdose
-Rarely due to decreased intake.
48.
Fluids and ElectrolytesImbalance
• Clinical manifestation;
-Muscle weakness or paralysis
-Arrhythmia (can be fatal), decreased cardiac contractility, labile arterial blood
pressure due to autonomic dysfunction
-Paralytic ileus (reduced peristaltic movements which mat also lead to
constipation)
• Treatment for hypokalemia:
• Intravenous replacement (should not exceed 8mEq/l in one hour)
49.
Hyperkalemia (plasmapotassium levels exceeds 5.5mEq/L)
Causes of hyperkalemia:
-decreased renal excretion: acute renal failure, hypoaldosteronism,
Addison’s disease and use of diuretics (potassium sparing)
-cellular shift due to acidosis, muscle/cellular injury, chemotherapy
and hemolysis
-increased intake due to oral or intravenous replacement therapy.
50.
Clinical manifestation:
-muscle weakness,tingling, numbness, mental confusion due to
neuromuscular conduction.
-Arrhythmias may be fatal (cardiac arrest)
NB. Confirm that it is true hyperkalemia & Obtain an ECG and
look for changes and manage accordingly
1. Calcium gluconateor calcium chloride to stabilize the cardiac
membrane.
2. Insulin and glucose to shift potassium into cells.
3. Sodium polystyrene sulfonate (Kayexalate) to remove potassium
from the body.
4. Beta-2 agonists such as albuterol, salbutamol to shift potassium into
cells.
5. Dialysis in severe cases.
53.
Fluids and ElectrolytesImbalance
Chloride
• It is a major extracellular anion.
• The normal range is 98-107mmol/l
• It neutralizes the positive charge of sodium in the fluid because of its negative charge.
Function of chloride
-Maintains osmolarity
-Maintains blood pressure
-Maintains electric neutrality of the body; NaCl is reabsorbed in proximal tubules.
-It exchanges with bicarbonate in RBC.
-Important in the formation of gastric HCl where by the chloride ions are secreted
along with protons from parietal cells.
54.
Fluids and ElectrolytesImbalance
Regulation of chloride
• It filtered out by the glomerulus and passively reabsorbed, in conjunction with
sodium, by the proximal tubules however excess chloride is excreted in the urine.
• Skin helps regulate chloride levels through sweating.
Hyperchloremia:
• Occurs in dehydration, Cushing syndrome, renal tubular acidosis, high intake
• Hypochloremia:
• Occurs due to vomiting, excessive sweating, Addison's disease
55.
Fluids and ElectrolytesImbalance
Bicarbonate
• The second most abundant anion in the extracellular fluid.
Function
-blood buffer system preventing the acid base disorder such as the acidosis.
-in collaboration with chloride, it maintain the neutrality charge of the cells.
Regulation
-85% of bicarbonate is reabsorbed by proximal tubules and 15 % is being
reabsorbed by the distal tubules. (it also being reabsord as carbon dioxide)
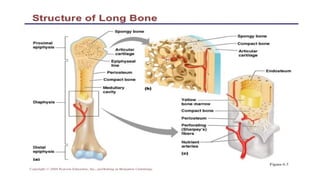
#4 The bone composition: 60% inorganic –calcium hydroxyapatite
40% organic (non mineralized matrix is known as osteoid) –type 1 collagen 9tensile strength), proteoglycans (compressive strength), osteocalcin/osteonectin (bone forming protein), under influence of PTH they participate in bone resorption and Ca transport.
Cells; Osteoblast-concerned with bone formation, they are rich in ALP and responsible for production of type I collagen
Esteocyte; spent osteoblast, communicate with each other with cytoplasmic process.
Esteoclast; principle mediator of bone resorption. By chemotactic they come and attach to specific regions on cell surface –ruffled border and release lysozyme
#6 Calcium is a major component of bone and teeth, about 1% of skeletal calcium is exchanged with blood cacium.
Calcium plays a major role in transmitting nerve impulses and helps to regulate muscle contraction and relaxation, including cardiac muscle.
#7 Any condition that causes a decrease in the production of PTH may result in the development of hypocalcemia
#10 Hypercalcemia stimulates the parafollicular cells to produce calcitonin which lowers the level of calcium (by blocking the breaking down of bone calcium and prevents reabsorption of calcium.
#37 Patients with Na+ below 120mEq/L develops serious manifestation
#39 SIADH (syndrome of inappropriate ADH) secretion: less water excreted by kidneys therefore dilute blood picture with low Na+; patient with hyponatremia, hypo-osmolarity.
#42 Produces a state of hyperosmolality, Imbalance of sodium and water in the body leads to this condition.
Occurs in people who do not drink water due to impaired thirst or mental judgment like people with dementia or an infant who can not access fluids
#48 ECG: T-wave flattening or inversion, prominent U wave, ST depression, prolonged PR interval
#49 ECG: peaked T waves, widening of QRS complex, prolonged P-R interval, loss of P wave, loss of R amplitude, ST segment depression