Water content varieswith age & tissue type
Fat has the lowest water content (~20%).
Bone is close behind (~22 – 25%).
Skeletal muscle is highest at ~65%.
5.
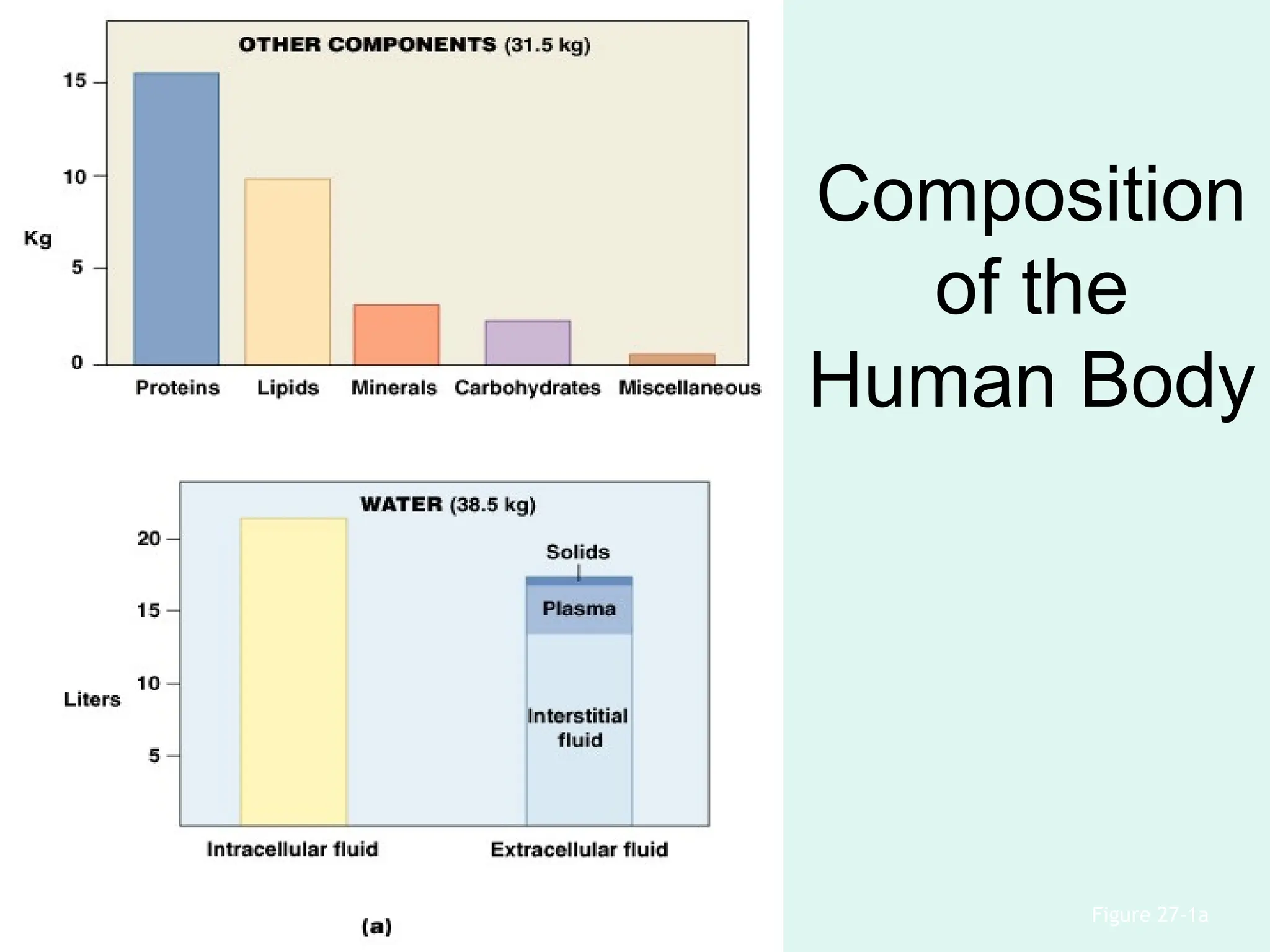
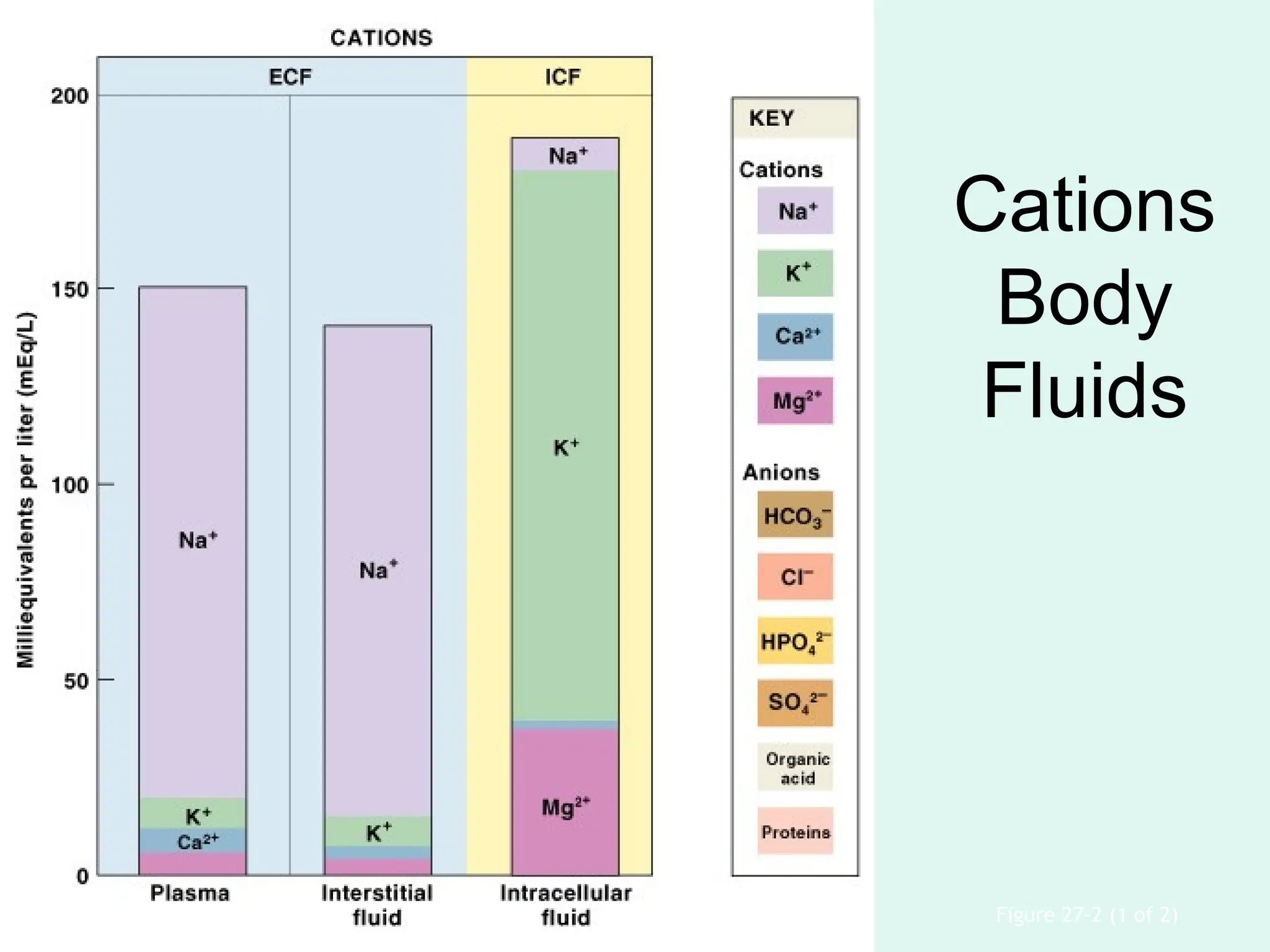
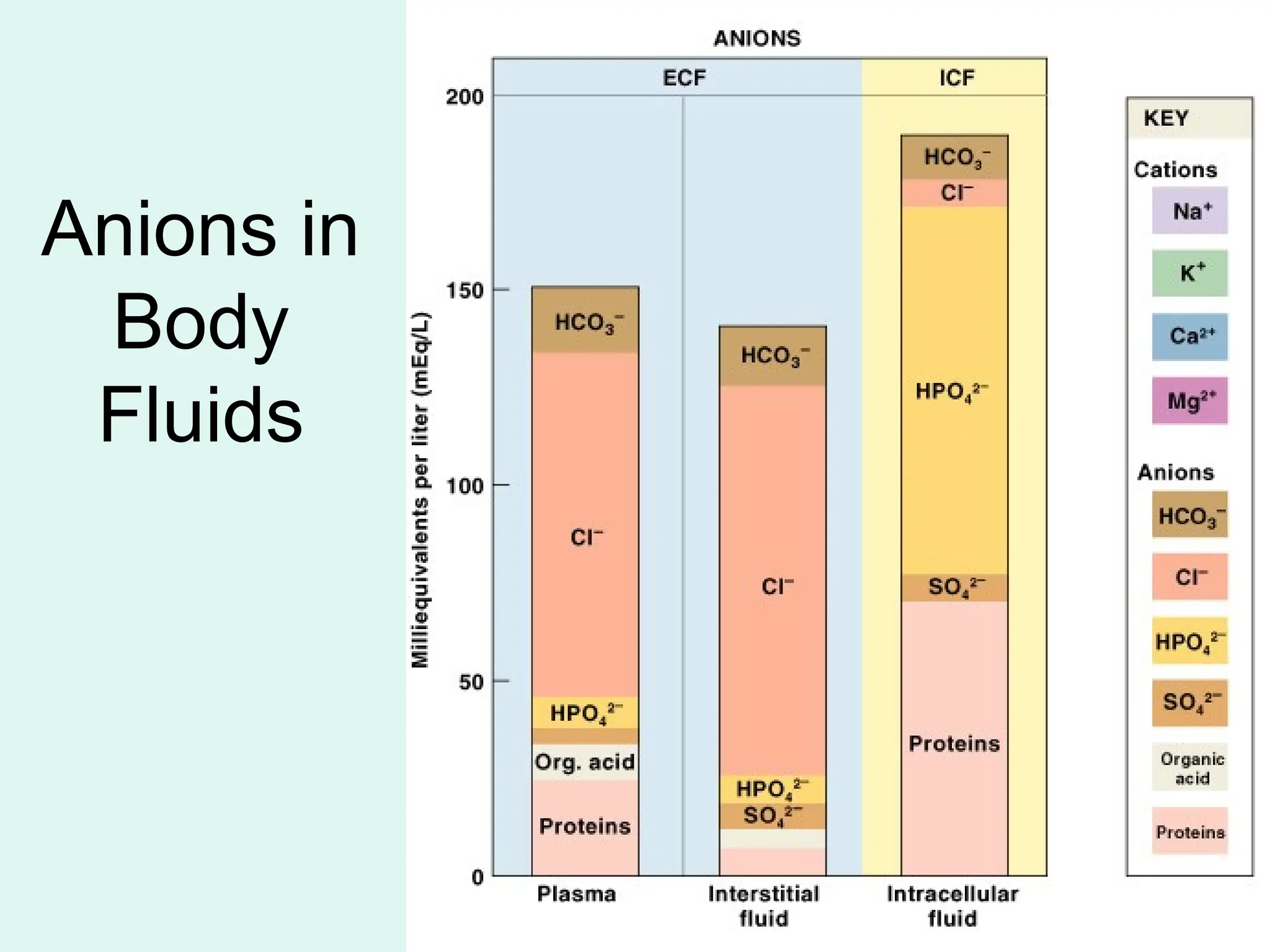
Fluid Compartments
• ECF(extra cellular fluid) and ICF
(intracellular fluid) are called fluid
compartments:
– because they behave as distinct entities
– are separated by cell membranes and active
transport
6.
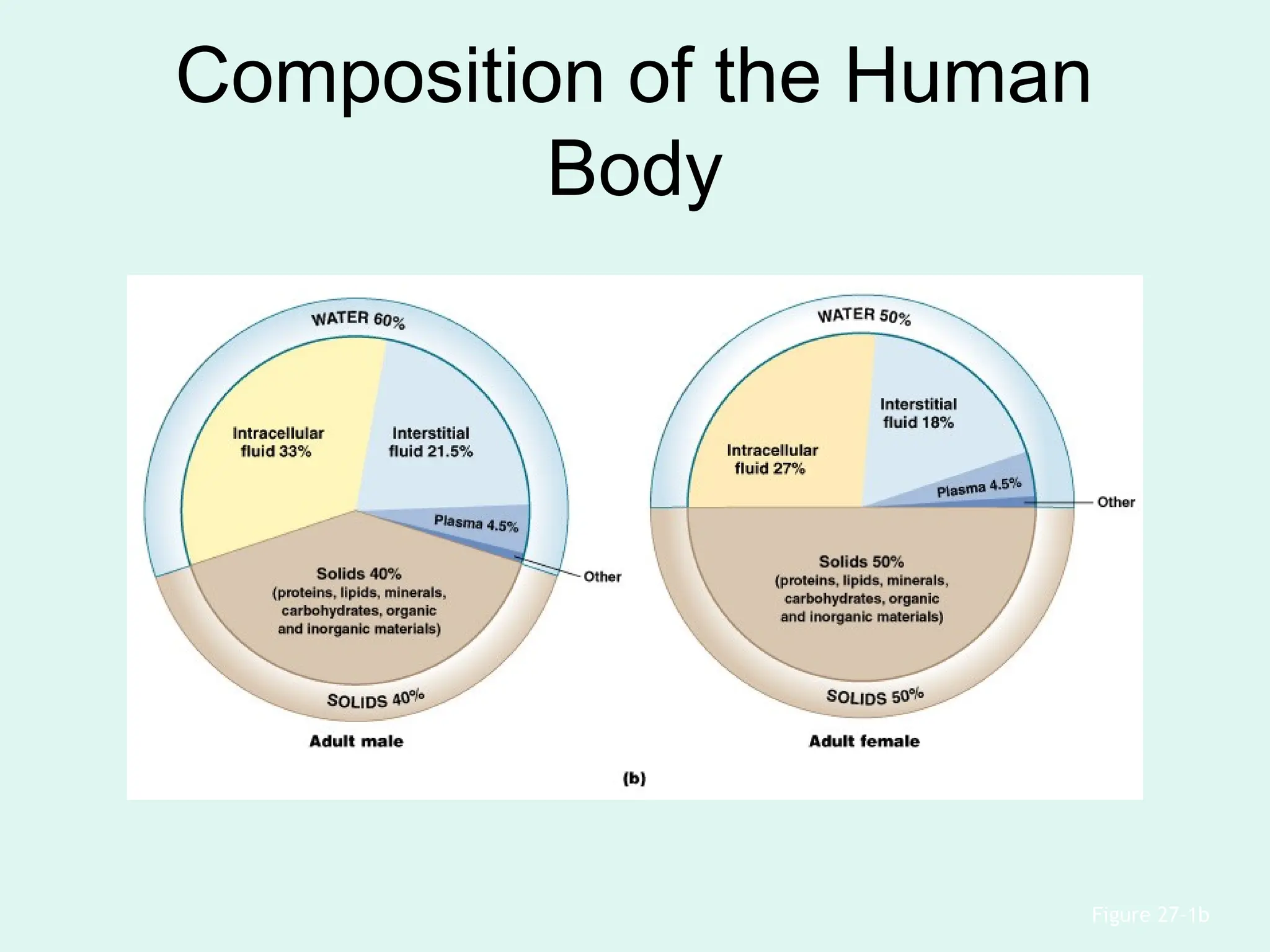
Water Composition
• Is60% percent of male body weight
• Is 50% percent of female body weight
• Mostly in intracellular fluid
7.
Water Exchange
• Waterexchange between ICF(2/3) and
ECF(1/3) occurs across cell membranes
by:
– osmosis
– diffusion
– carrier-mediated transport
8.
Major Subdivisions ofECF
• Interstitial fluid of peripheral tissues(2/3)
• Plasma of circulating blood(1/3)
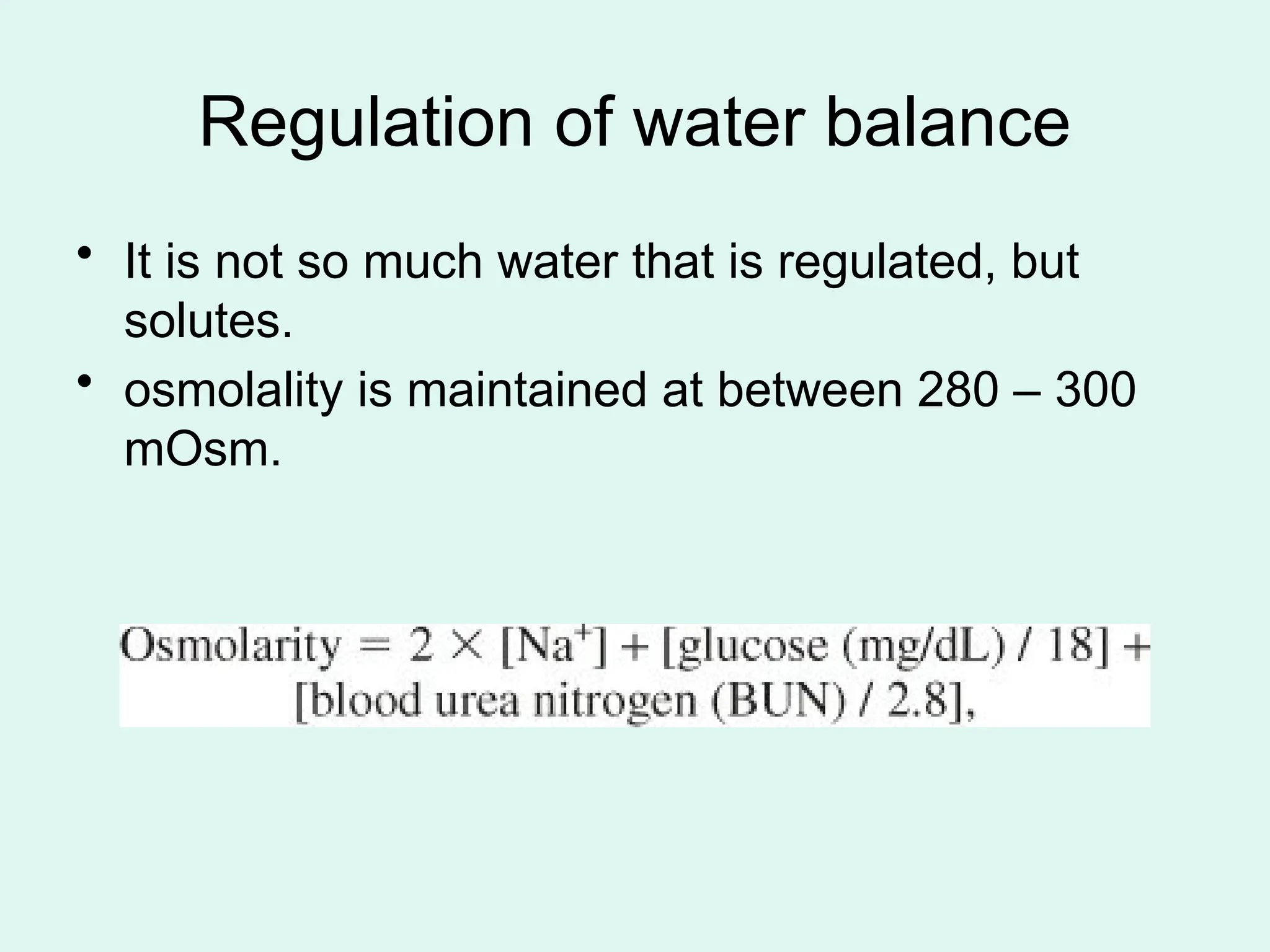
Regulation of waterbalance
• It is not so much water that is regulated, but
solutes.
• osmolality is maintained at between 280 – 300
mOsm.
12.
Sodium
• Is thedominant cation in ECF
• Sodium salts provide 90% of ECF osmotic
concentration (97% with other related
anions)
• Need: 1-3meq/kg/day
13.
renin–angiotensin system
• 1-Decreasein intravascular volume
• 2-Decrease in renal arterial flow
• 3-renin secretion (juxtaglomerular)
• 4-angiotensin to angiotensin I
• 5-angiotensin I to II (in lungs by ACE)
• 6-aldosterone secretion (adrenal cortex)
• 7-↑reabsorption of Na and water, ↓K and H
• 8-↑ECF
14.
Antidiuretic Hormone (ADH)or
vasopressin
• Stimulates water conservation at kidneys:
– reducing urinary water loss
– concentrating urine
• Stimulates thirst center:
– promoting fluid intake
15.
Potassium
• Is thedominant cation in ICF
• Need: 0.5-1meq/kg/day
• 95% excreted in urine and 5% in feces
FLUIDS AND ELECTROLYTES
INTHE PERIOPERATIVE
PERIOD
• Maintenance (D.W5% 1/2N.S +20meq
KCl) (4:2:1 rule)
• Replacement of ongoing loss (same fluid)
18.
• Fluid, electrolyte,and acid–base imbalances
must be identified and treated promptly in
acutely ill patients
• Third spacing
• Loss: ↓hemodynamic - ↓out(0.5cc/kg/h) –
lab(↑ hct- bun/cr20- feNa20)
• Isotonic crystalloides
• Monitor by hemodynamics, output and IVC
sono
Volume excess
• fluidor sodium restriction
• diuresis along with a replacement of
potassium losses
• In vascular volume deficit careful
replacement with crystalloid or blood
products may be needed
26.
Hyponatremia
• Low, highor normal ECF
• Dilutional
• Artificial (high TG or Glucose)
• Necrotizing soft tissue infections
Treatment
• Water restriction
•Stop thiazide
• In chronic max:12 meq/l/d (central
pontine myelinolysis)
• Water and Na restriction in high ECF
• Isotonic in low ECF
• Hypertonic in severe symptoms
Hypernatremia
• loss ofwater alone (hypothalamic abnormalities,
nonreplaced insensible losses)
• loss of water and salt together (gastrointestinal losses,
osmotic diuresis, excessive diuretic use, central or
nephrogenic diabetes insipidus, burns, excessive
sweating)
• increased total body sodium without any water loss
(Cushing’s syndrome, hyperaldosteronism,
ectopic production of ACTH, iatrogenic sodium
administration, ingestion of seawater)
31.
Hypernatremia
• symptoms ofdehydration
• neuromuscular and neurologic disorders
(twitching, restlessness, weakness,
delirium, coma, seizures, and death)
• Intracranial hemorrhage is a common
postmortem finding in patients who die of
hypernatremia.
32.
Treatment
• Water (poor D.W5%)
• Half replacement in 12-24h with
monitoring
• Fast replacement results in brain
edema
33.
Potassium
• 98% ofpotassium in the human body is in
ICF
• Cells expend energy to recover potassium
ions diffused from cytoplasm into ECF
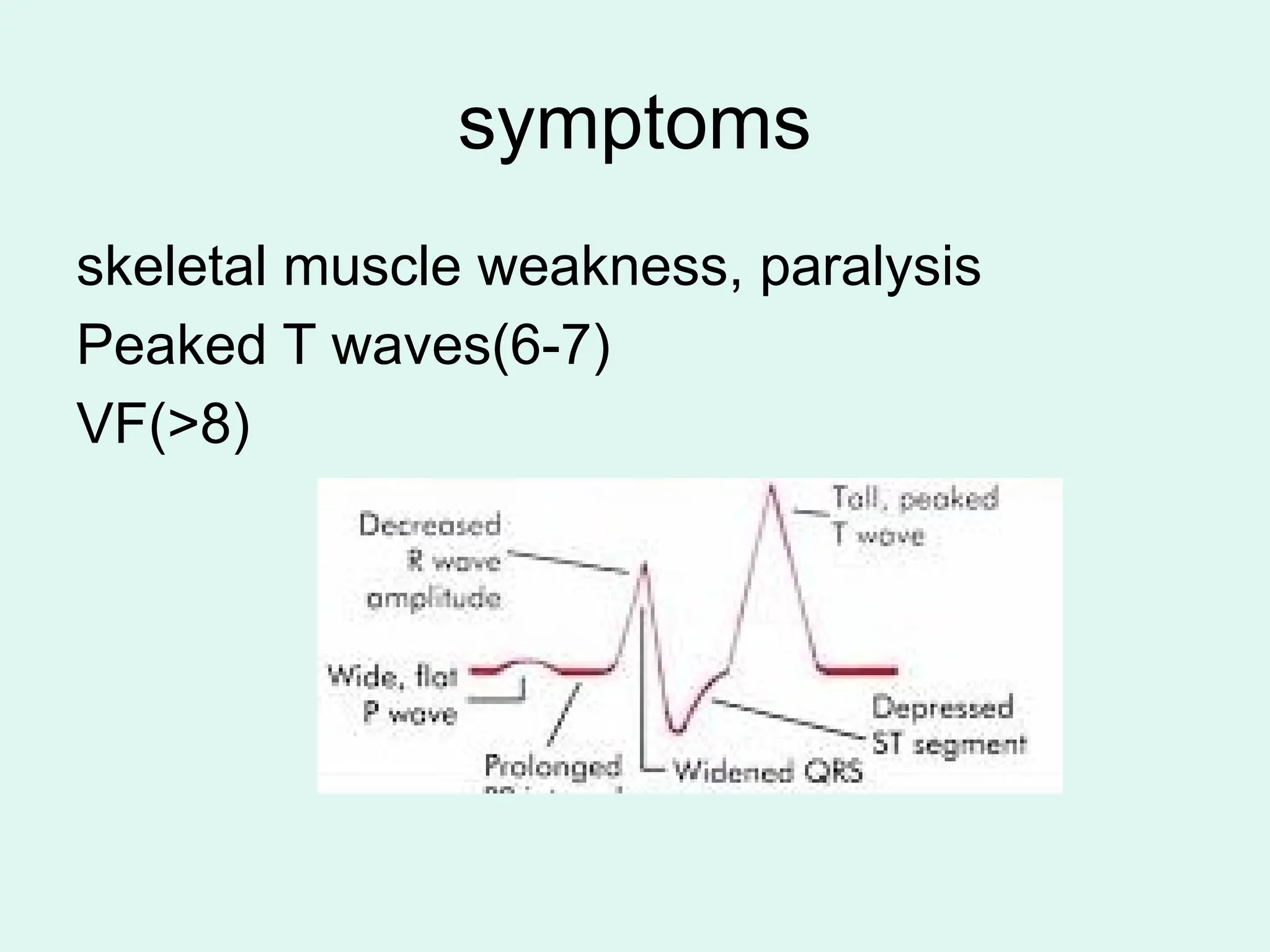
symptoms
<3 meq/L
skeletal muscleweakness, fatigue,
paresthesias, paralysis, rhabdomyolysis.
Deep-tendon reflexes may be diminished or
absent.
anorexia, polyuria, and nausea and vomiting
associated with paralytic ileus
36.
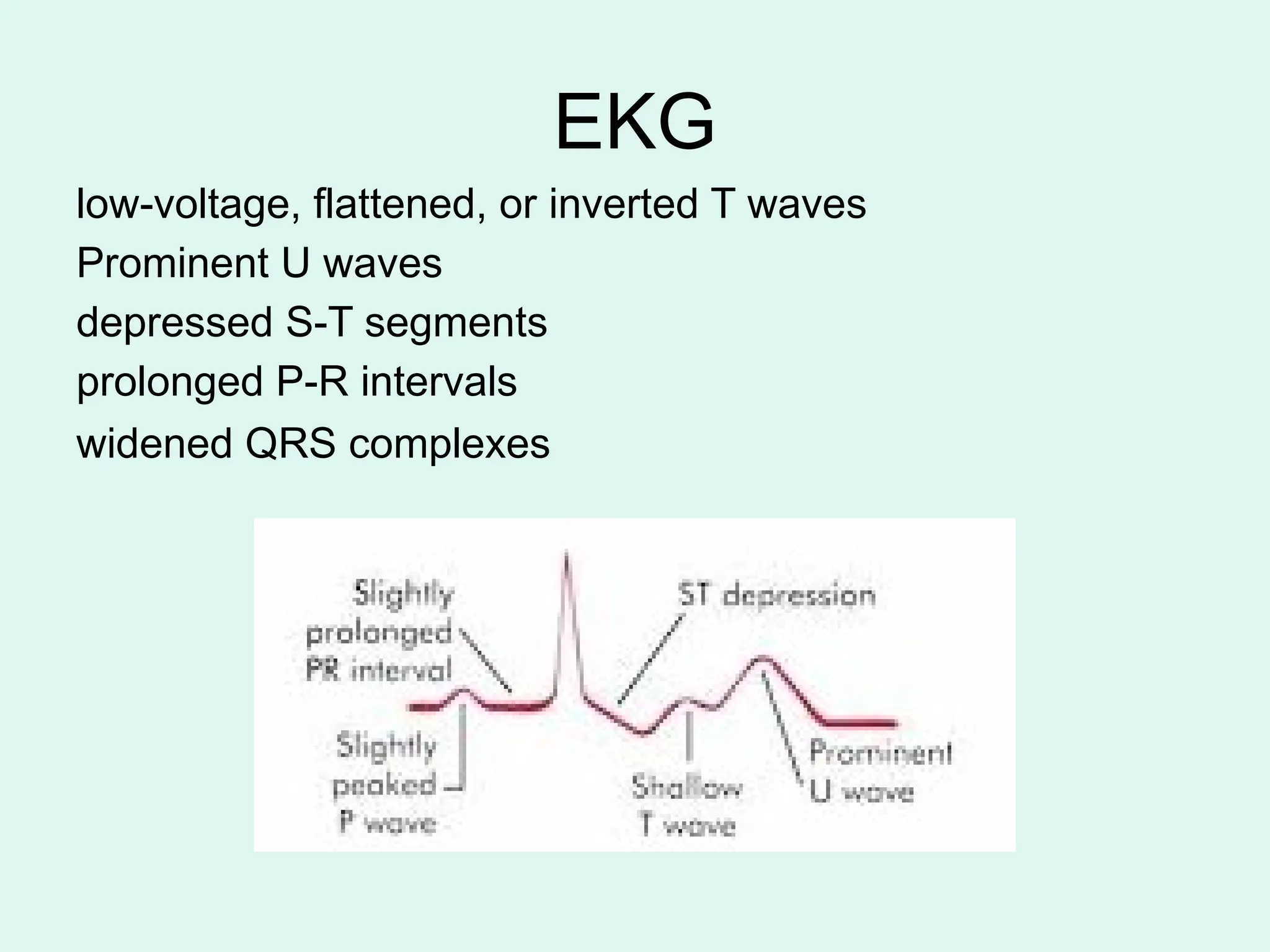
EKG
low-voltage, flattened, orinverted T waves
Prominent U waves
depressed S-T segments
prolonged P-R intervals
widened QRS complexes
37.
Treatment
• Check Digoxinlevel in mild
• Ca and Mg in severe or resistant
• Oral or IV(less than 10meq/h)
• Till above 3.5
38.
Hyperkalemioa
>5 meq/L
high intake(foodor blood) or
shift(crush,hemolysis,hematoma,catabolism,
acidosis) or renal disease
K sparing diuretics, NSAIDs, B blockers,
ACEi
Treatment
• Recheck
• Inmild(<6) restrict potassium intake,
eliminate causes (potassium-sparing
diuretics) and treat fluid volume or acid–
base disorders.
Potassium-wasting diuretics may be
administered, and hormone deficiencies
may be replaced
41.
Treatment
• >6
• 10units of insulin with 25 g of glucose
intravenously over 5 minutes
• Bicarbonate
• Kayexalate
• Ca-gluconate(only in ecg changes)
• hemodialysis
42.
Calcium
• Total 8.5-10.5
•Ionized 4.75-5.3 (physiologic effect)
• PTH : intestinal absorption, renal
excretion, and calcium exchange between
bone and the ECF.
43.
Hypocalcemia
• < 8mEq/L
• acute pancreatitis , necrotizing fasciitis
• Inadequate intestinal absorption(IBD)
• chronic diarrhea or pancreatic or intestinal
fistulas
• Artifactual hypocalcemia
• phenytoin and phenobarbital
• Vit D deficiency
• Massive transfusion
• Hypopara and hypomagnesemia(low PTH)
symptoms
weakness, fatigue, anorexia,nausea, vomiting
severe headaches, diffuse musculoskeletal pain,
polyuria, polydipsia
hypovolemia and dehydration
shortened Q-T intervals and widened T waves
calcification may develop in the kidneys as well as
in unusual locations (heart, skin)
Pancreatitis and renal failure
>15 mg/dL cause confusion and depression and
death
Treatment
• Oral inmild
• IV magnesium solphate in moderate
and malabsorption
53.
Hypermagnesemia
• Rare
• renalfailure, dehydration, severe metabolic
acidosis, adrenal insufficiency, familial benign
• hypocalciuric hypercalcemia, or overdosage with
magnesium salts in cathartics
• treatment of eclampsia
• renal failure who use magnesium-containing
antacids
Hypophosphatemia
• Along withhypokalemia and hypomagnesemia
• Decrease in intake or increase in excretion or
shift
• Alcohol whitdrawal
• Vit D deficiency
• Malignancies
• Hypermetabolic state
• Hungry bone syndrome
58.
symptoms
anorexia, dizziness, osteomalacia,severe
congestive cardiomyopathy, proximal muscle
weakness, visual defects, ascending paralysis,
hemolytic anemia, respiratory failure
Inability to wean from the ventilator
rhabdomyolysis, hypercalciuria
severe hypocalcemia are also seen
seizures, coma, and death
Hyperphosphatemia
• increase inintake or decrese in excretion or shift
• Renal failure
• Hypopara
• Vit D toxicity
• sarcoidosis or TB
• Tumor lysis syndrome








































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)





