First Line ofDefense
• Nonspecific
• Distinguishes self from non-self, but
does NOT distinguish between
pathogens.
• Includes (Barriers)
•Skin & mucous membranes???
•Chemicals
5
6.
Second Line ofDefense
• Responds to antigens that penetrate the
first line.
• Includes
1. Inflammatory response
2. Pyrogens
3. Interferons
4. Complement proteins
6
7.
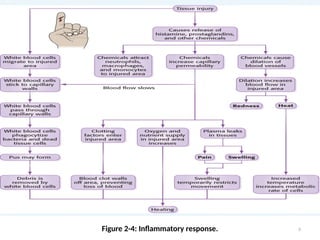
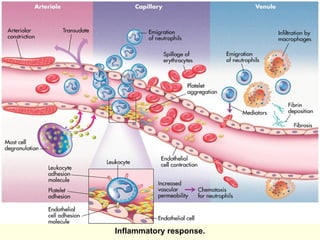
1. Inflammatory Response
•Vascular reaction due to any damage or
trauma.
• Triggered by mast cells that produce
histamine & prostaglandin.
• Manifestations: erythema, edema, pain &
warmth.
• Migration of cells (neutrophils, phagocytes).
• Fibrin formation.
7
2. Pyrogens
• Fever-producingmolecules
• Produced by macrophages, and go to
hypothalamus
• Create an unpleasant environment for
bacterial growth
• Fever increases metabolism
• After 105F (40.6 C), becomes life
threatening.
10
11.
3. Interferons
• Proteinsreleased from virus-infected
cells.
• Bind to nearby uninfected cells.
• The uninfected cells release an enzyme
that prevents viral replication.
• When the virus infects the cells, the are
unable to replicate.
11
4. Complement Proteins
•Blood Plasma Proteins to enhance antibodies.
• Activated by antigens.
• Play a role in the immune & inflammatory
response through (examples only):
1. stimulating vasodilation,
2. increasing permeability,
3. chemical attraction,
4. promote phagocytosis.
13
14.
Third Line ofDefense
• The body’s own immune system.
• Specific, develops over time.
• Uses memory system to distinguish self from
non-self, AND between pathogens.
• Includes (Figure 2-6):
– T cells: cell-mediated immunity
• Regulator (Helper & suppressor), & Effector (killer)
• Role in viral infection, CA prevention, & hypersensitivity
– B cells: humoral immunity
• memory cells vs immunoglobulin-secreting (Antibody) cells
14
15.
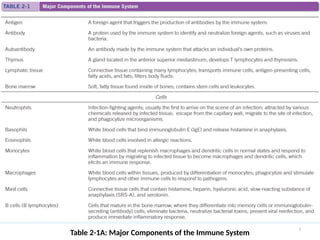
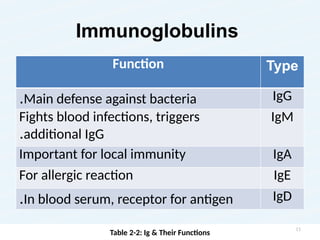
Immunoglobulins
Function Type
Main defenseagainst bacteria
. IgG
Fights blood infections, triggers
additional IgG
.
IgM
Important for local immunity IgA
For allergic reaction IgE
In blood serum, receptor for antigen
. IgD
Table 2-2: Ig & Their Functions
15
16.
Acquired Immunity (Table2-3)
• Active Immunity
–Sources include having the disease
(natural) & vaccinations (artificial)
–Long lasting, but takes a few days to
become effective...Why???
• Passive Immunity
–Sources include maternal-fetal transfer of
immunoglobulins and breastfeeding
–Short lasting
16
Altered Immune Response
A.Hypersensitivity (exaggeration):
–inflated immune response to a foreign
substance… has 4 types.
B. Autoimmune (misdirection):
–mistakes self as non-self
C. Immunodeficiency (diminution)
–inadequate immune reaction
18
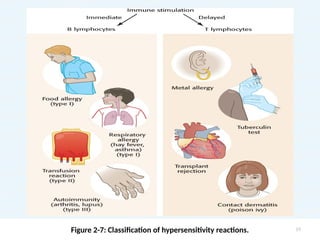
Types of Hypersensitivity
Type1- IgE mediated
– Produces an immediate response
– Local or systemic
– Allergens activate T cells which bind to mast cells.
– At next exposure, the antigen binds with the
surface IgE, releasing mediators & triggering the
complement system.
– Examples: hay fever, food allergies, &
anaphylaxis---- immediate inflammation & pruritus.
– Treatment: epinephrine, antihistamines,
corticosteroids, & desensitizing injections.
20
21.
Types of Hypersensitivity
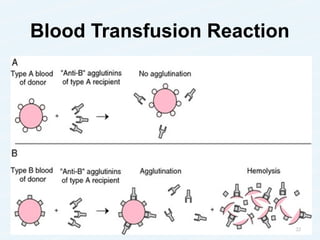
TypeII- cytotoxic hypersensitivity reaction
– IgG or IgM antibodies react to antigen on cells,
which activates the complement.
– Result: Lysis of cells & phagocytosis
– Usually immediate responses
– Examples: Blood transfusion reaction &
erythroblastosis fetalis
– Treatment: ensuring blood compatibility &
administering medication to prevent maternal
antibody development
21
Types of Hypersensitivity
TypeIII- immune complex-mediated
hypersensitivity reaction
– Circulating antigen-antibody complexes
accumulate & are deposited in the tissue
– Triggers the complement system & inflammation
– Example: Autoimmune conditions (e.g. systemic lupus
erythematosus [SLE])
– Treatment: disease specific
23
24.
Types of Hypersensitivity
TypeIV, delayed hypersensitivity reaction
Involves delayed processing of the antigen
by macrophages.
Cell-mediated rather than antibody-
mediated involving T cells (release cytokines)
Examples: tuberculin skin testing, transplant
reactions, contact dermatitis
Treatment: disease specific
24
25.
Transplants
• Making thebest match of tissue antigens is
the core for success (Tissue Compatibility)
• Donor sources may be living or a cadaver
• Four Categories:
1. Allogenic: donor & recipient are related or
unrelated, but share similar tissue types (common)
2. Syngenic: donor & recipient are identical twins
3. Autologous: donor & recipient are the same
person; most successful
4. Xenogenic: donor is from another species
25
26.
Patterns of TransplantReactions
• Hyperacute
– immediate or 3 days after transplant
– due to the complement system (presence of antibodies)
– Tissue becomes necrotic
• Acute
– most common, treatable
– Occurs 4 days to 3 months after transplant
– Cell-mediated leads to inflammation
– Manifestations: fever, erythema, edema, site tenderness,
and impaired function of transplanted organ
• Chronic
– occurs 4 months to years after transplant
– likely antibody-mediated response
– Antibodies & complements deposit in vessel walls of
transplanted tissue, resulting in ischemia 26
27.
Transplant Reaction Classifications
•Host vs Graft Rejection
– Host fights the graft
– The recipient’s immune system attempts to
eliminate the donor cells
• Graft vs Host Rejection
– Graft fights the host
– Frequent & potentially fatal complication of BMT
– Occurs when immunocompetent fatal cells
recognize host tissue as foreign & mount a cell-
mediated immune response
– Host usually immunocompromised & unable to
fight graft cells (host’s cells are destroyed)
27
28.
Autoimmune Disorders
• Immunesystem loses the ability to recognize self
• Defenses are directed against host (self-destructive)
• Can affect any tissue, or systemic
• Mechanism that triggers this response is Unclear
• Examples: SLE, RA, GBS
• Known characteristics
– Genetics play a role
– More prevalent in females
– Onset is frequently associated with an abnormal stressor,
either physical or psychological
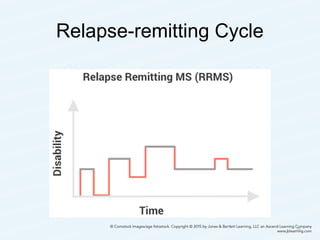
– Are frequently progressive relapsing-remitting disorders
characterized by periods of exacerbation & remission
28
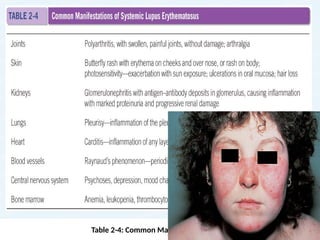
Systemic Lupus Erythematosus
•Chronic inflammatory condition
• Remission & exacerbations (stressors tend to trigger)
• Affects connective tissue of any body organ
• Disease progression varies from mild to severe
• More common in women
• Cause is unclear, but thought that B cells are
activated to produce autoantibodies & autoantigens
that combine to form immune complexes, which
attack the body’s own tissues.
30
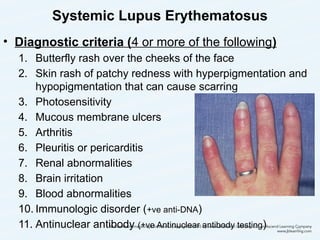
Systemic Lupus Erythematosus
•Diagnostic criteria (4 or more of the following)
1. Butterfly rash over the cheeks of the face
2. Skin rash of patchy redness with hyperpigmentation and
hypopigmentation that can cause scarring
3. Photosensitivity
4. Mucous membrane ulcers
5. Arthritis
6. Pleuritis or pericarditis
7. Renal abnormalities
8. Brain irritation
9. Blood abnormalities
10. Immunologic disorder (+ve anti-DNA)
11. Antinuclear antibody (+ve Antinuclear antibody testing) 32
33.
Systemic Lupus Erythematosus
•Prognosis improves with early diagnosis & treatment
• Diagnosis
– 11 criteria, X-rays, elevated sedimentation rate, c-
reactive protein, and blood testing for complications
• Treatment
– no cure, symptom management
– Stress management & health promotion behaviors
– Pharmacological
• NSAIDs, antimalarials, corticosteroids, &
immunosuppressants
– Plasmapheresis
33
34.
Immunodeficiency
• Diminished orabsent immune response
• Renders the person susceptible to diseases
normally prevented (Opportunistic infections)
• Acute vs chronic
• Causes include viral or Iatrogenic
• Classifications
–Primary (defect in immune system)
–Secondary (a disease suppressing immune system)
• Rx: gammaglobulins, BMT, Isolation,…
34
35.
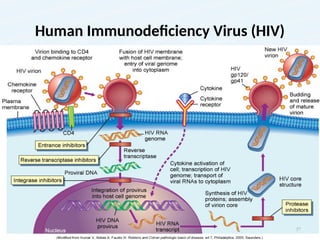
AIDS
• HIV: parasiticretrovirus that infects CD4 &
macrophages upon entry
• Two primary strains
– Type I (most common in USA)
– Type 2 (most common in Africa; progresses to
disease more slowly)
• In USA, rates rising among women & African
Americans
• Transmission: STD, Blood & bodily fluids
35
AIDS Progression
• Asymptomaticphase: Flu-like symptoms
–virus is reproducing (usually for several years)
• Infections begin as the viral number rise
destroying the CD4
• Progression takes three forms
–Immunodeficiency: opportunistic infections
–Autoimmunity: arthritis,…
–Neurological dysfunction: AIDS demenetia
38
39.
AIDS Progression
• Diagnostictest (used for diagnosis &
determine progression)
–HIV antibody
• Rapid test
• Home test
• Polymerase chain reaction
–Measures amount HIV DNA or viral load
–Good for infants and infected mothers
39
40.
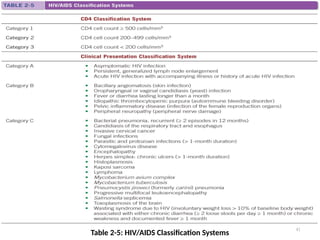
AIDS Classification System
•Two systems, one based on lab findings and
the other based on clinical manifestations
• Laboratory findings (Categories 1,2,3)
• Clinical
– Category A: asymptomatic
– Category B: some less serious manifestations of
immune deficiency
– Category C: AIDS defining illnesses present
40
AIDS Treatment
• Nocure
• Combination therapy works best
–Highly Active Antiretroviral Therapy
• May have to change regimen due to viral
adaptation
• Other meds & vaccines will be used to
prevent opportunistic infections as needed
• Vaccinations
• Transmission prevention
42
43.
The Status ofthe Epidemic in Jordan
• Jordan has a low prevalence HIV epidemic (both among the general population
and among key populations at higher risk of HIV exposure).
• The total number of HIV and AIDS cases registered at MoH/NAP (1986-2013) is
1026 (28% Jordanians and 72% Non Jordanians).
• The total Number of Jordanians and Non Jordanians tested positive for HIV in
2012 and 2013 is 83 and 86, respectively.
• The cumulative number of HIV and AIDS cases registered at MoH/NAP for
Jordanians till end of 2013 is 283 cases (80% males, 20% females).
• The total number of HIV and AIDS cases registered in 2012: 16 (81% males and
19% females)
• The total number of HIV and AIDS cases registered in 2013: 19 (84% males and
16 % females)
• Sexual Contact remains the main mode of HIV transmission, accounting for almost
71% of HIV and AIDS cases registered in both 2012 and 2013.
• The cumulative number of deaths among HIV, and till the end of December, 2013
is 107 (78% males and 22% females)
http://www.unaids.org/en/dataanalysis/knowyourresponse/countryprogressreport
43
44.
At Risk Individualsfor Immune
Dysfunction
• Very young & very old
• Poor nutrition
• Impaired skin integrity
• Circulatory issues
• Alterations in normal flora due to antibiotic therapy
• Chronic diseases especially diabetes mellitus
• Corticosteroid therapy
• Chemotherapy
• Smoking
• Alcohol consumption
• Immunodeficiency states
44
45.
Immune Building Strategies
•Increasing fluid intake
• Eating a well-balanced diet
• Increasing antioxidants & protein intake
• Getting adequate sleep
• Avoiding caffeine & refined sugar
• Spending time outdoors
• Reducing stress
45




![Types of Hypersensitivity
Type III- immune complex-mediated
hypersensitivity reaction
– Circulating antigen-antibody complexes
accumulate & are deposited in the tissue
– Triggers the complement system & inflammation
– Example: Autoimmune conditions (e.g. systemic lupus
erythematosus [SLE])
– Treatment: disease specific
23](https://image.slidesharecdn.com/chapter2bodydefenses-260111071110-7e335690/85/Body_defenses_chapter_Anatomy_Thenursing-23-320.jpg)















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
