This document provides information on bipolar disorder including:
- The prevalence of bipolar disorder is estimated to be around 2% of the population, or about 17,800 people in Calgary.
- Common comorbid disorders include substance abuse issues (61% of people with bipolar disorder), anxiety disorders, narcissistic or borderline personality disorders.
- Adolescents presenting with bipolar disorder are more likely to experience delusions or be misdiagnosed with conduct disorder due to irritability.
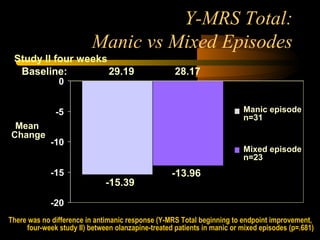
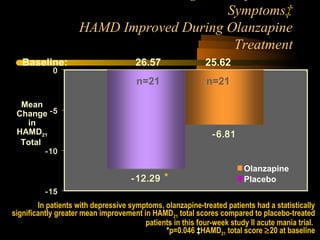
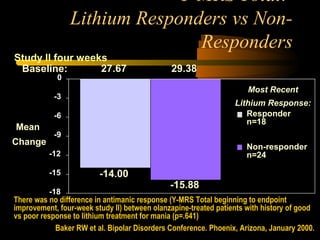
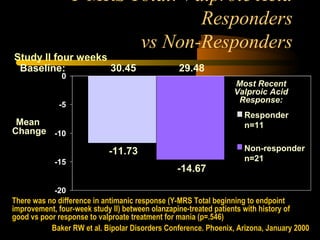
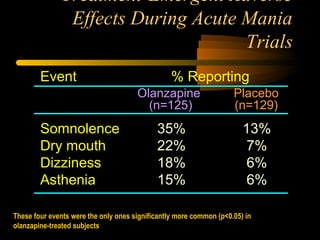
- Treatments discussed include mood stabilizers like lithium, lamotrigine, valproate, atypical antipsychotics like olanzapine, and augmentation with thyroid hormone or anticonv

















































![Bipolar disorders [2002]](https://cdn.slidesharecdn.com/ss_thumbnails/bipolardisorders-170814010745-thumbnail.jpg?width=640&height=640&fit=bounds)





















