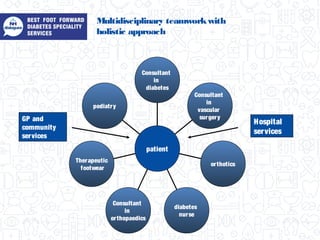
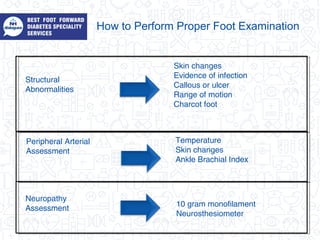
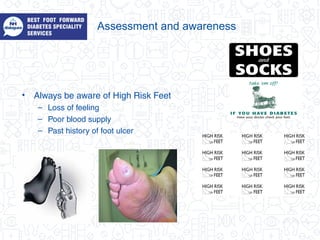
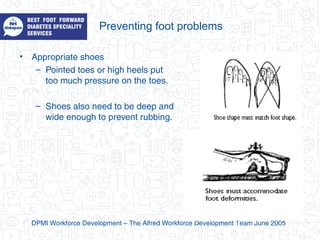
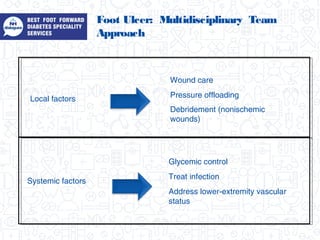
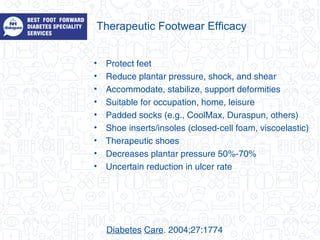
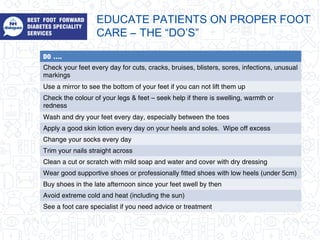
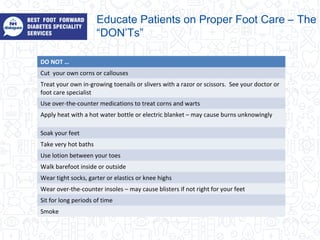
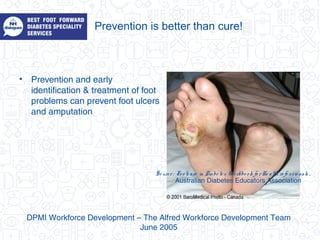
The document discusses the complications of diabetes, particularly emphasizing the risks of foot problems due to factors like decreased blood supply, nerve damage, and high blood sugar levels. It outlines the importance of a multidisciplinary team approach, proper foot examination, and appropriate footwear to prevent and manage diabetic foot issues. Key prevention strategies include daily foot checks, proper hygiene, and patient education on foot care do's and don'ts.


























































![Incare Shoe Training[1] Copy](https://cdn.slidesharecdn.com/ss_thumbnails/incareshoetraining1copy-100109030138-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)





























![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)











