Download as PDF, PPTX



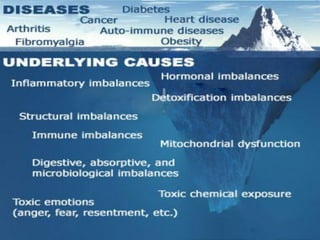

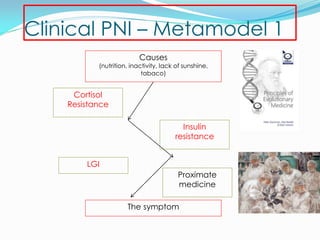
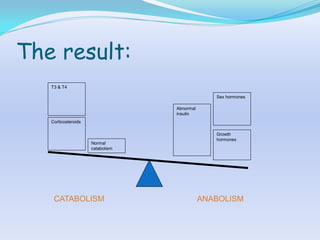





This document provides an overview of obesity, energy balance, inflammation, and other factors related to metabolic health. It discusses how factors like stress, poor diet, lack of activity, and environmental toxins can disrupt metabolic processes and gene expression, leading to issues like insulin resistance, obesity, and disease. The document recommends addressing the root causes of metabolic imbalance through a Mediterranean-style diet high in nutrients and low in inflammation-promoting foods. Regular physical activity and lifestyle factors are also important to maintain metabolic health and gene expression. The goal is to take an integrative, upstream approach to metabolic disorders through nutrition and lifestyle interventions before relying on downstream medical treatments.


































































































