
More Related Content
What's hot
Similar to BalancedScoreCard
Similar to BalancedScoreCard (20)
BalancedScoreCard
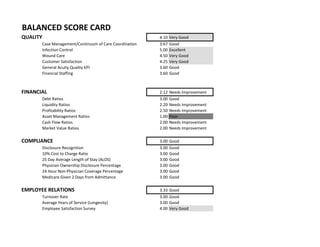
- 1. 4.10 Very Good 3.67 Good 5.00 Excellent 4.50 Very Good 4.25 Very Good 3.60 Good 3.60 Good 2.12 Needs Improvement 3.00 Good 2.20 Needs Improvement 2.50 Needs Improvement 1.00 Poor 2.00 Needs Improvement 2.00 Needs Improvement 3.00 Good 3.00 Good 3.00 Good 3.00 Good 3.00 Good 3.00 Good 3.00 Good 3.33 Good 3.00 Good 3.00 Good 4.00 Very Good BALANCED SCORE CARD Physician Ownership Disclosure Percentage Asset Management Ratios Cash Flow Ratios Market Value Ratios COMPLIANCE Disclosure Recognition 10% Cost to Charge Ratio 25 Day Average Length of Stay (ALOS) 24 Hour Non-Physician Coverage Percentage EMPLOYEE RELATIONS Turnover Rate Average Years of Service (Longevity) Employee Satisfaction Survey Medicare Given 2 Days from Admittance QUALITY Financial Staffing Debt Ratios Profitability Ratios Case Management/Continuum of Care Coordination Infection Control Wound Care Customer Satisfaction General Acuity Quality KPI Liquidity Ratios FINANCIAL
- 2. Score Weight Weighted Score Quality 4.10 0.25 1.03 Financial 2.12 0.5 1.06 Compliance 3.00 0.15 0.45 Employee Relations 3.33 0.1 0.33 2.87 Needs Improvement OVERALL PERFORMANCE:
- 3. BENCHMARK 2015 YTD SCORE DESCRIPTOR Case Management/Continnum of Care Coordination 3.67 Good 6.0% 1.9% 5 Excellent 10.0% 0.0% 5 Excellent 25.0% 13.5% 3 Good 18.0% 17.3% 3 Good 20.0% 20.0% 3 Good 65.0% 63.0% 3 Good 7.0% 5.0% 4 Very Good 8.0% 13.0% 2 Needs Improvement 12.0% 8.0% 5 Excellent 5.0 Excellent 4.5 0 5.0 Excellent 2.8 0 5.0 Excellent 0.95 0 5.0 Excellent 0 5.0 Excellent 0 5.0 Excellent 0.7 5.0 Excellent 90.0% 96.9% 5.0 Excellent 0.59 0 5.0 Excellent 4.5 Very Good 0.8 0 5.0 Excellent 90.0% 92.5% 4.0 Very Good 31 4.25 Very Good 50.0% 75.0% 5.0 Excellent 97.4% 95.0% 4.0 Very Good 97.4% 90.0% 4.0 Very Good QUALITY KPI 1. Returns to the STACH 2. Readmit to STACH in 30 Days 3. Home Discharge Rate 4. Mortality Rate 5. Short Stay Outliers 8. Ventilator Associated Pneumonia (VAP) 1. Hospital Acquired Pressure Ulcers (HAPU) 2. Wound Improvement Infection Control Measures 6. Window Management Wound Care/HBO Core Measures 7. Full Stay Discharges 8. High Cost Outliers 9. Zero Paid Days 1. Hospital Acquired Infections (HAI) 2. Catheter Associated Urinary Tract Infections (CAUTI) 3. Central Line Acquired Blood Stream Infection (CLABSI) 4. MRSA 5. VRE 6. C-Difficile Rate 7. Hand Hygiene Rate 3. Volume of HBO Treatments Customer Satisfaction 1. Patient Satisfaction Survey Response Rate 2. Positive Recommendation 3. Positive Perception
- 4. 93.9% 90.0% 4.0 Very Good 3.6 Good 1.58 1.34 2.0 Needs Improvement 2.64 2.3 3.0 Good 0.49 0 5.0 Excellent 0.1 0.1 3.0 Good 1.67 0.7 5.0 Excellent 69.0% 66.7% 3.6 Good 8.7 8.4 2.0 Needs Improvement 300.00$ $309.00 3.0 Good 3.0% 3.5% 5.0 Excellent 0 0.005 3.0 Good 2 1.8 5.0 Excellent 8. Speech Therapy Cost Per Treatment 7. Patient Safety Survey Results General Acuity Related Quality Indicators Financial Staffing Key Indicators 5. Medication Error Rate 6. Vent Wean Rate 1. Nursing Hours Per Patient Day (NHPPD) 2. Nursing Dollars Per Patient Day (N$PPD) 3. Overtime Hours as % of Total Productive Hours 4. Contract Labor Hours as % of Total Productive Hours 5. Respiratory Hours Per Patient Day (RTHPPD) 6. Physical Therapy Cost Per Treatment 7. Occupational Therapy Cost Per Treatment 1. Case Mix Index (CMI) 2. Patient Fall Rate 3. Patient Falls with Injury 4. Restraints Days Rate 6. Physician Satisfaction Survey Results 4. Call Light Response Rate 5. Employee Satisfaction Survey Results
- 5. PYYTD 2015 YTD SCORE DESCRIPTOR 3.00 Good 0.67 0.77 3.0 Good 0.78 0.84 3.0 Good 0.07 0.09 3.0 Good 3.59 5.39 3.0 Good 0.45 0.52 3.0 Good 2.20 Needs Improvement 0.89 0.89 3.0 Good 0.15 0.07 1.0 Unsatisfactory 0.93 0.93 3.0 Good -295.00 -253.00 1.0 Unsatisfactory 0.89 0.89 3.0 Good 2.50 Needs Improvement 1. Cash Return on Capital Invested 2. DuPont Formula 172 221 3.0 Good 4. Effective Rate of Return 0.03 0.14 4.0 Very Good 6. Operating Expense Ratio 0.03 0.14 4.0 Very Good 8. Profitability Index FINANCIAL KPI Debt Ratios 1. Asset Coverage Ratio 2. Capitalization Ratio 3. Debt Ratio 5. Quick Ratio 4. Debt Service Coverage Ratio 5. Debt-to-Equity Ratio 10. Long Term Debt to Total Asset Ratio 11. Total Expense Ratio Liquidity Ratios 1. Acid-Test Ratio 2. Cash Ratio 3. Current Ratio 4. Net Working Capital 7. Operating Margin Profitability Ratios 3. EBITDA 5. Gross Profit Margin 6. Debt-to-Income Ratio 7. Equity Multiplier 8. Long Term Debt to Capitalization Ratio 9. Long Term Debt to Total Asset Ratio
- 6. -0.02 0.01 2.0 Poor -0.04 0.02 1.0 Unsatisfactory 11. Return on Net Assets -0.05 0.04 2.0 Poor -0.03 0.09 3.0 Good 55.12 13.57 1.0 Unsatisfactory 1.0 Unsatisfactory 4. Days Inventory Outstanding 5. Days Payable Outstanding 1.50 0.38 1.0 Unsatisfactory 2.00 Needs Improvement 2.00 Needs Improvement *$$$ in Thousands 9. Return on Assets 10. Return on Debt 7. Inventory Turnover 8. Receivable Turnover Ratio Cash Flow Indicator Ratios 1. Cash Flow Coverage Ratio 12. Retun on Net Assets 13. Return on Revenue 14. Revenue per Employee Asset Management Ratios 1. Account Payable Turnover Ratio 2. Asset Turnover 3. Enterprise Value Muliple 4. Net Asset Value per Share 5. Price to Earnings Ratio 6. Stock Price 2. Cash Flow Return on Investment 3. Free Cash Flows 4. Price/Cash Flow Ratio Market Value Ratios 1. Dividend Payout Ratio 2. Dividend Yield 3. Capacity Utilization Rate 6. Fixed Asset Turnover
- 7. BENCHMARK 2015 YTD SCORE DESCRIPTOR *No existing information. For illustrative purposes. Turnover Rate Average Years of Service (Longevity) Employee Satisfaction Survey EMPLOYEE RELATIONS
- 8. BENCHMARK 2015 YTD SCORE DESCRIPTOR 24 Hour Non-Physician Coverage Percentage Disclosure Recognition 10% Cost to Charge Ratio 25 Day Average Length of Stay (ALOS) Physician Ownership Disclosure Percentage COMPLIANCE KPI
- 9. Medicare Given 2 Days from Admittance *No existing information. For illustrative purposes.
- 10. DESCRIPTION NUMERIC SCORE Excellent (<10%ile) 5 Very Good (10-25%ile) 4 Good (25-50%ile) 3 Need Improvement (50-75%ile) 2 Poor (75-90%ile) 1 Unsatisfactory (90+%ile) 0 BALANCED SCORECARD SCORING E.g.