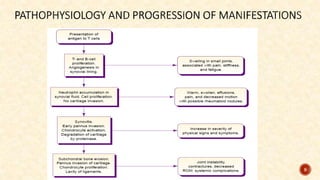
Mrs. Sunita presents with worsening joint pain and stiffness primarily in her hands, leading to difficulty in daily activities. The physician orders tests to investigate potential causes and prescribes anti-inflammatory medication alongside exercises. The document elaborates on rheumatoid arthritis, its causes, symptoms, stages, and management strategies, alongside comparisons to osteoarthritis and gout.




























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






