

Recommended
More Related Content
What's hot
What's hot (20)
Similar to ataxia
Similar to ataxia (20)
More from Mohamed Rizk Khodair
More from Mohamed Rizk Khodair (16)
Recently uploaded
Recently uploaded (20)
ataxia
- 1. Ataxia Dr mohamed rizk khodair Lecturer of neurology Mohamedrizk.med@o6u.edu.eg
- 2. • Developed from the metencephalon • Located in the posterior cranial fossa
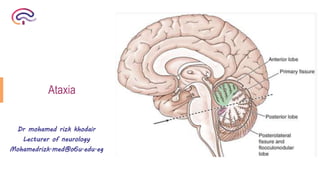
- 3. Lobes of the cerebellum Primary fissure Posterolateral fissure Anterior lobe Posterior lobe Flocculonodular lobe
- 5. The cerebellum consists of three functional subdivisions: 1- Vestibulocerebellum 2- Spinocerebellum 3- Cerebrocerebellum
- 6. Phylogenetically Formed of Primary afferent connections Concerned with Vestibulocerebellum Archicerebellum (the oldest part) Flocculonodular lobe Vestibular nuclei Eye movements, gross balance, equilibrium, orientation of the body in space Spinocerebellum Paleocerebellum Midline vermis and adjacent paravermal cortex Spinocerebellar tracts Posture, muscle tone, axial muscle control Cerebrocerebellum Neocerebellum (the most recent part) The cerebellar hemispheres (the largest part) Pontine nuclei, which receives corticopontine fibers from the cerebral cortex Coordination of movement and providing fine motor control for the precise movements of the extremities
- 7. The cerebellum is connected to the brainstem by 3 cerebellar peduncles: • ICP: connects cerebellum with the medulla • MCP: connects cerebellum with the pons • SCP: connects cerebellum with the midbrain
- 8. SCA (from basilar artery) superior surface AICA (from basilar artery) anterior part of the inferior surface PICA (from 4th part of vertebral artery) posterior part of the inferior surface + lateral part of the medulla
- 9. The cerebellum is made up of a white matter core, covered with a thin layer of grey matter, the cerebellar cortex The cortex is made up of 3 layers: • Outer molecular layer • Purkinje cell layer • Inner granular layer
- 10. Incoordination of voluntary motor activity in absence of motor weakness Cerebellar ataxia Sensory ataxia Vestibular ataxia Mixed HYSTERICAL ATAXIA
- 11. Causes of cerebellar ataxia Hereditary : Friedrich's ataxia , Marie's ataxia Idiopathic : delayed cortical cerebellar degeneration in old age Toxic: alcohol. Drugs: phenytoin; lithium. Vascular: ischemic stroke; hemorrhage. Inflammatory: demyelination (MS, ADEM). Neoplastic: metastases (breast, bronchus); primary brain tumors (in children, pilocytic astrocytoma and medulloblastoma); Paraneoplastic syndrome, associated with small cell lung cancer; ovarian cancer, breast cancer, testicular cancer , Hodgkin’s lymphoma , neuroblastoma , and thymoma. Infectious/post-infectious: viral cerebellitis (measles); SSPE; HIV; Miller Fisher syndrome (ataxia, areflexia, ophthalmoplegia + GQ1b antibody). Structural: Arnold–Chiari malformation; AVM; Degenerative: Friedrich ataxia, adult-onset cerebellar ataxia Nutritional: vitamin E deficiency, thiamine (B1deficiency), e.g., in Wernicke’s encephalopathy; Endocrine: thyroid.
- 12. History/ clinical examination • Type of ataxia (cerebellar, sensory, vestibular) • Affected parts of the body zone of the cerebellum affected • Associated manifestations • Severity of symptoms • Cause of ataxia Investigations
- 13. Personal history • Age at onset, gender • Occupation history, possible toxic exposure to chemicals • Sexual history (HIV, syphilis) • Drug abuse, and excessive alcohol intake Past history • Regular drug use and a possible temporal association with ataxia onset • HTN, DM, other chronic medical illness Family history and pedigree analysis Present history • Mode of onset (acute, subacute, chronic) • Natural history (progressive, regressive, stationary, episodic/intermittent) • Associated symptoms/signs that provide localizing information and determine the underlying etiology • Other systemic features e.g. cardiac, hepatic Functional ataxia should be a diagnosis of exclusion
- 14. Laboratory testing Condition Routine labs (CBC, serum electrolytes) Metabolic abnormalities ESR, ANA, ds-DNA Abs, RF Inflammatory conditions, vasculitis Vitamin B12, B6 levels Nutritional deficiency Vitamin E levels Vitamin E deficiency, AVED TSH Thyroid disease Virology, RPR/FTA Infections e.g. HIV, syphilis Therapeutic drug levels Drug-induced ataxia Urinary heavy metal levels , blood alcohol levels Toxicity Serum/ urine protein electrophoresis Lymphoproliferative disorders Paraneoplastic panel Paraneoplastic Autoantibodies: • anti- GAD65 antibody • anti-GQ1b • antigliadin antibody Glutamic acid decarboxylase (GAD) ataxia Miller Fisher syndrome Gluten ataxia CSF analysis CJD, encephalitis, MS, neoplasm, paraneoplastic, mitochondrial disease, .. Laboratory tests for evaluation of acquired ataxia:
- 15. Testing Condition Copper, ceruloplasmin, 24-hour urinary copper Wilson’s disease Vitamin E levels AVED Serum lipoprotein, acanthocytes in blood film Abetalipoprotinemia Serum cholesterol levels and urinary bile alcohol levels Cerebrotendinous xanthomatosis Serum phytanic acid levels Refsum’s disaese Alpha- fetoprotein and immunoglobulin Ataxia telangiectasia Serum cholesterol and albumin Ataxia with oculomotor apraxia type 1 Alpha-fetoprotein Ataxia with oculomotor apraxia type 2 Erythrocyte glucose uptake assay - CSF glucose level Glucose transporter type 1 deficiency CoQ10 in skeletal muscle by high performance liquid chromatography Ataxia associated with coenzyme Q10 deficiency Lactate, pyruvate Mitochondrial disorder EMG/NC Evaluation for polyneuropathy (axonal vs. demyelinating) Muscle biopsy Mitochondrial disorder Consider genetic testing Certain tests if hereditary ataxia is suspected:
- 16. • Detect the cause • Assess for brainstem and cerebellar atrophy • Some MRI signs are diagnostically useful, as hot cross bun sign (MSA), MCP sign (FXTAS), panda sign (Wilson's disease),.. Neuroimaging:
- 17. Clinical Significance 1-Hypotonia, the muscles lose resistance to palpation due to diminished influence of the cerebellum on gamma motor neurons. 2- The patient walks with a wide or broad-based gait and leans toward the affected side. 3- Disturbances of voluntary movements, called ataxia, involve tremors with fine movements, such as writing or buttoning the clothes. 4- Finger to nose test is performed to examine the coordination of the muscle movements. When a patient is asked to touch the tip of the nose with the index finger, the movements are not properly coordinated, and tremor is observed at the end of the movement, called intention tremor. 5- A similar test can be performed on the lower limbs by asking the patient to place the heel of one foot against the shin of the opposite leg (foot to heel to leg).
- 18. 6- Ataxia of ocular muscles results in nystagmus, a rhythmical oscillation of the eyes. To provoke nystagmus, the patient should rotate eyes horizontally. 7- Similarly, ataxia of the larynx muscles results in dysarthria in form of staccato speech . 8- Dysdiadochokinesia is the lack of ability to perform rapidly alternating movements. One can ask the patient to quickly supinate and pronate both forearms simultaneously. Movements will be slow and incomplete on the side of the cerebellar lesion. 9- Dysmetria—an inability to perform acute finger-to-nose movements accurately with past pointing or a similar inability on heel/shin testing.
- 19. Coordination System examination A. Upper limb (With opened and closed eyes) 1. Finger to nose , 2. Finger to finger test , 3. Finger to nose to doctor’s finger test 4. Dysdiadokokinesia : inability to perform rapid alternating movement (pronation and supination ) 5. Rebound phenomenon : with sudden release of flexed elbow 6. Buttoning or unbuttoning test : earliest sign
- 20. Finger to nose to doctor’s finger test Finger to nose test Finger to finger test Dysdiadokokinesia Rebound phenomenon
- 21. B. Lower limb : (With opened and closed eye ) 1.Heel to knee test. 2. Standing : swaying ----- truncal ataxia 3. Walking along straight line 4. Romberg sign
- 22. Friedreich’s ataxia • It occurs in First decade of life • More common in Female > male • Postive Family history (Autosomal recessive) • Pathologically there is degeneration of Four : 1-cerebellum espcialley archicerebellum and spinocerebellum tracts 2- pyramidal tract 3-posterior column 4- peripheral nerve • Sketeltal deformities pes cavus and kyphioscoliosis • Congential heart disease and ECG changes are common
- 23. Sensory ataxia Clinical features : any marked loss of proprioception will result in sensory ataxia. • Signs of a neuropathy with loss of joint position sense. • Pseudo athetosis of fingers when arms outstretched, and eyes closed. • Upper limb position sense loss is tested by attempting to bring both horizontally outstretched index fingers together in the midline with eyes closed. • Heel/shin testing deteriorates with eye closure. • Positive Romberg’s sign.
- 24. Differential diagnoses of sensory ataxia • CIDP. • Refsum’s disease (due to defect in phytanic acid metabolism. Other features include deafness, retinitis pigmentosa). • Spinal cord disorders (affecting posterior columns): • demyelination (MS). • B12 deficiency.
- 25. Vestibular ataxia • Vestibular ataxia has prominent vertigo (directional spinning sensations) and may cause past pointing of limb movements, but spares speech.