
More Related Content
Similar to Antibiotics notes.docx
Similar to Antibiotics notes.docx (20)
More from JifamyFundalFaeldin
Recently uploaded
Recently uploaded (20)
Antibiotics notes.docx
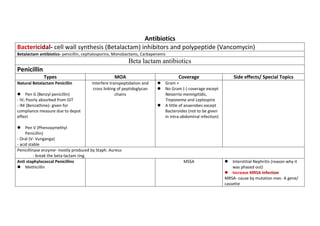
- 1. Antibiotics - cell wall synthesis (Betalactam) inhibitors and polypeptide (Vancomycin) Betalactam antibiotics- penicillin, cephalosporins, Monobactams, Carbapenems Beta lactam antibiotics Penicillin Types MOA Coverage Side effects/ Special Topics Natural Betalactam Penicillin Pen G (Benzyl penicillin) - IV; Poorly absorbed from GIT - IM (Benzathine)- given for compliance measure due to depot effect Pen V (Phenoxymethyl Penicillin) - Oral (V- Vunganga) - acid stable Interfere transpeptidation and cross linking of peptidoglycan chains Gram + No Gram (-) coverage except Neiserria meningitidis, Treponema and Leptospira A little of anaerobes except Bacteroides (not to be given in intra-abdominal infection) Penicillinase enzyme- mostly produced by Staph. Aureus - break the beta-lactam ring Anti staphylococcal Penicillins Methicillin MSSA Interstitial Nephritis (reason why it was phased out) MRSA- cause by mutation mec- A gene/ cassette
- 2. - Change the PBP to PBP 2A causing the B-Lactam loss its affinity. - DOC: Community-acquired (Clindamycin) Hospital-aquired (Vancomycin Nafcillin MSSA Reversible aggranulocytosis Hepatoxicity Isoxazoyl Penicillin - Oxacillin, Cloxacillin, Dicloxacillin Best treatment for staphylococcal infection Like IMPETIGO Aminopenicillin Ampicillin- parenterally; poor GI absorption; Frequently combined with aminoglycoside (Amikacin or gentamicin) because of synergism Amoxicillin- better GI absorption Gram + Gram - Little of anaerobes except Bacteroides fragilis Antipseudomonal Penicillins Carboxypenicillins - Carbenicillin, Ticarcillin Ureidopenicillin - Piperacillin (Most potent) - Azlocillin -Mezlocillin Pseudomonas Aeroginosa Beta-lactamase Inhibitors - Clavulanic acid co-administered with beta-lactam antimicrobials to prevent Gram + Gram -
- 3. - sulbactam - tazobactam antimicrobial resistance by inhibiting serine beta-lactamases, which are enzymes that inactivate the beta-lactam ring, which is a common chemical structure to all beta-lactam antimicrobials Anaerobes including Bacteroides fragilis Cephalosporins Generation Drugs Coverage First Generation -CEPH including Cefalexin (formerly cephalexin) Cefazoline Cefadoxil Gram + plus PEK P- Proteus E- E.coli K- Klebsiella Second generation -CEF followed by a VOWEL Including, META PRO *CefPROzil *CefMETAzol And LORAcarbef Gram + HEN- Haemophilus influenzae, Enterobacter, Neiserria PEK Anaerobes Third Generation -CEF Plus Consonant including PERA, TAXes and FIXers *CefoPERAzone *CefoTAXime *CeFIXime And Moxalactam Gram - HEN PEK Plus SSS- Serratia, Salmonella, Shiegella Pseudomonas- Ceftazidime, Cefoperazone only Fourth Generation Cefipime Cefpirone 3rd Gen coverage + Pseudomonas Fifth Generation The Bothers ROLI and TOBI 4th Generation Plus MRSA
- 4. CeftaROLIne CefTOBIprol Monobactams Astreonam- only IV Same coverage with Ceftazidime (3rd gen coverage + pseudomonas) S/e: No- cross sensitivity ADR: Transaminitis-> Drug induced hepatitis (Increase AST, ALT) Carbapenems- sulfur atom in the Thiazolidine ring was replaced by CARBON atom COVERAGE - Gram +, gram -, Anaerobes, Pseudomonas aeroginosa (except ERTAPENEM) -ALL are epileptogenic but IMEPENEM is more pronounced. - Imepenem is degraded by dehydropeptidase enzyme at renal tubule thus added with CILASTIN (prolongs Imepenem effects) -tx for ESBL infection - Doripenem- best coverage for pseudomonas Polypeptide antibiotics Vancomycin Others: Televancin, teicoplanin MOA: inhibits cell wall synthesis by binding to D-ala-ala- terminus thereby inhibiting transglycosylation furthering subsequent transpeptidydation 0r cross-linking * Vancomycin DOC for hospital-acquired MRSA and PSEUDOMEMBRANOUS Colitis (ORAL) In PH we used METRONIDAZOLE for Pseudomembranous colitis ADR: * REDMAN or RED neck syndrome- erythematous rash; This is INFUSION RElated - SLOW the infusion - Hydrate the patient - give Antihistamines- Cetirizine->Diphenhydramine->Steroids *Nephrotoxic - Vancomycin trough level must be requested, the lowest possible dose to have its effects.
- 5. POLYMIXINS - cell membrane inhibitors -cationic detergents -never a drug of choice -last line - not as a monotherapy (combined with betalactam and aminoglycoside Polymixin B Topical B- Bilat JOKE!!!! BALAT Polymixin E Colistin Parenteral PROTEIN SYNTHESIS INHIBITORS - targets translation; ALL Protein SYNTHESIS Inhibitors are Bacteriostatics except AMINOGLYCOSIDES REMEMBER: Buy AT 30 SELL CC at 50 30 S- Aminoglycosides, Tetracyclins BLOCKS 30S->blocks formation of initiation complex-> blocks translation-> mRNA misreading Aminoglycosides - MYCIN- from Streptomyces *Neomycin *Tobramycin *Streptomycin - MICIN- from Microminispora *Gentamicin *AMikacin - BACTERICIDAL - Polar- No oral absorption - ALL must be given PARENTERALLY to achieve adequate serum levels except NEOMYCIN (topical or oral) - synergistic with BETA-LACTAM, do not combine in 1 contaniner (Beta lactam first then aminoglycoside) -ADR: NEPHROTOXICITY, VESTIBULOTOXICITY, OTOTOXICITY (only in high frequency sounds) OTOTOXIC- Neomycin> Amikacin> Kanamycin (sino ang inuoto? aNAK) VESTIBULOTOXIC- Streptomycin, Gentamicin NEPHROTOXIC- Neomycin, Tpbramycin, Gentamicin - Tobramycin- most toxic -COVERAGE: * Gram + except strep pneumoniae
- 6. * Gram - * Pseudomonas * No coverage for atypical and anaerobes Tetracyclines- bacteriostatic Short acting * Tetracycline * Chlortetracyclines * Oxytetracycline Intermediate * Demeclocycline *Methacycline Long-acting- DoMino *Doxicycline *Minocycline Pharmacokinetics Absorption impaired by food (except doxycycline, minocycline), antacids, dairy products, and divalent cations (Ca2+, Mg2+, Fe2+), or Al3+ due to COMPLEX FORMATION/ CHEILATION *Separate atleast 2 hours for gastric emptying · High protein-binding · Widely distributed to tissues except CSF · Excellent intracellular penetration · Excreted in bile and urine except Doxycycline (bile only not renally excreted) · Can pass the placenta, excreted in milk Coverage: Gram + Gram - Atypical organism (leigionella, chlamydia, leptospira, vibrio, borelia- DOC Anaerobes (-) coverage for Pseudomonas aeroginosa BROADEST spectrum TIGECYCLINE- COVERS everything except 3PM 3P- Pseudomonas, proteus, providencia L- Morganella ADR: Straining TET (Teeth) Enamel hypoplasia Bone deformity/ growth retardation Avoid in children <8 years old 50 S SUBunits- SELL CC at 50 Streptogramins Erythromycin and other macrolides
- 7. Lincosamides Linzezolides- Chloramphenicol, Clindamycin Macrolides -thromycin RACE Roxitromycin Azithromycin- only macrolide using concentration dependent reaction Clarithromycin Erythromycin Coverage: Gram + Gram - Atypical NO COVERAGE for Pseudomonas and Anaerobes SUBSTITUTE for PENICILLIN allergies ADR: Erythromycin- GI disturbances, motilin release Lincosamide * Lincomycin - sulfur containing antibiotics - notorious in causing Steven Johnson Syndrome *Clindamycin Coverage - Gram positive - Community acquired MRSA - Anaerobes * above respiratory diaphragm except brain: CLINDAMYCIN * below the respiratory diaphragm including the brain: METRONIDAZOLE ADR: most commonly cause Pseudomembranous colitis ( due to prolong and/0r multiple antibiotics) Tx: Oral Vancomycin, or metronidazole
- 8. Chloramphenicol - second line drugs due to BONE MARROW SUPPRESSION/ myelosuppresion-> Aplastic ANEMIA - ADR: GRAY BABY SYNDROME- baby appears cyanotic (dose= <50mg/kg/day) Due to impaired glucorinidation reaction due to lack of UDP- glucoronosyl transferase in infant. -in INFANT drug metabolism is only via SULFATION NUCLEIC ACID SYNTHESIS Inhibitors - TMP- Sulfamethoxazole or Co- Trimoxazole Co-timoxazole Mechanism of action Dihydropteroate synthase Dihydrofolate reductase (Sulfonamide acts here) (TMP acts here) PABA--------------------------> Dihydrpfolic acid----------------------------> Tetrahydrofolic acid--------> Purine----> DNA DRUG of CHOICE for: Stenotrophomonas maltophilia Burkholderia cepacian Pneumocystis jeroveci pneumonia Toxoplasma gondii OTHER diseases: ONLY as SECOND LINE ADR: *Bleeding and KIDNEY OBSTRUCTION (Crystalluria) * CRYSTALLURIA: Acidic Urine, High Urinary Concentration, Low Solubility * Agranulocytosis *hemolytic anemia: C/I in G6PD deficiency *Kernecterus *STEVEN JOHNSON SYNDROME
- 9. - Interfere in TOPOISOMERASE II and IV----> increase supercoiling-----> bacterial DNA will be fragile-----> DNA Damage - TOPOISOMERASE- relieve Supercoiling - BACTERICIDAL -Coverage: Gram positive, gram negative, ATYPICAL, anaerobe (only in MOXIfloxacin), Pseudomonas aeroginosa (ONLY CIPROFLOXACIN and LEVOFLOXACIN) - Respiratory fluoroquinolones: MOXIfloxacin, LEVOfloxacin, GATIfloxacin - ADR: HYPERGLYCEMIA (except GATIFLOXACIN but causes HYPOglycemia), Arthropathy, QT-prolongation