
Recommended
More Related Content
Similar to antepartumhaemorrhage-i-160714051258.pdf
Similar to antepartumhaemorrhage-i-160714051258.pdf (20)
Recently uploaded
Recently uploaded (20)
antepartumhaemorrhage-i-160714051258.pdf
- 2. DEFINITION • It is defined as bleeding from or into the genital tract after the 28th week of pregnancy but before the birth of the baby. • Incidence -3% amongst hospital deliveries.
- 3. CAUSES
- 4. PLACENTA PREVIA When the placenta is implanted partially or completely over the lower uterine segment (over and adjacent to the internal os) it is called PLACENTA PREVIA. INCIDENCE: -About one-third cases of antepartum hemorrhage. -The incidence of placenta previa ranges from 0.5–1%. -In 80% cases, it is found to multiparous women. -Incidence increases beyond the age of 35, with high birth order pregnancies and in multiple pregnancy.
- 5. ETIOLOGY • Dropping down theory • Persistence of chorionic activity in the decidua capsularis and its development into capsular placenta • Defective decidua • Big surface area of placenta
- 6. Predisposing factors • Multiparity • Increased maternal age(>35yrs) • History of previous cesarean section or any other scar in the uterus (myomectomy or hysterotomy) • Placental size and abnormality (succenturiate lobes) • Smoking • Prior curettage
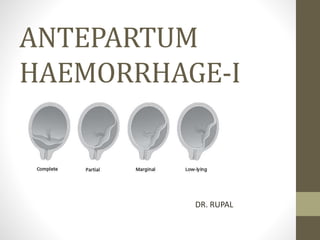
- 7. TYPES/DEGREES OF PLACENTA PREVIA *For clinical purpose, the types are graded into Mild degree (Type-I and II anterior) and Major degree (Type-IIposterior, III and IV).
- 8. CLINICAL FEATURES SYMPTOMS ONLY SYMPTOM- VAGINAL BLEEDING Classical features of bleeeding suddenonset,painless,apparently causeless and recurrent. • 5% cases occurs for the first time during labor, especially in primigravidae. • one-third of cases, there is a history of “warning hemorrhage” usually slight. • bleeding is unrelated to activity and often occurs during sleep and the patient becomes frightened on awakening to find herself in a pool of blood
- 9. • SIGNS General condition and anemia are proportionate to the visible blood loss. ABDOMINAL EXAMINATION The size of the uterus is proportionate to the period of gestation. The uterus feels relaxed, soft and elastic Persistence of malpresentation like breech or transverse or unstable lie is more frequent. The head - floating Fetal heart sound is usually present, unless there is major separation of the placenta with the patient
- 10. • VULVAL INSPECTION -blood is bright red • Vaginal examination must not be done outside the operation theater in the hospital, as it can provoke further separation of placenta with torrential hemorrhage and may be fatal • CONFIRMATION OF DIAGNOSIS- USG
- 12. MANAGEMENT IMMEDIATE (1) Amount of the blood Loss assessed — by noting the general condition, pallor, pulse rate and blood pressure (2) Blood samples are taken for group, cross matching and estimation of hemoglobin (3) A large-bore IV cannula is sited and an infusion of normal saline is started and compatible cross matched blood transfusion should be arranged (4) Gentle abdominal palpation to ascertain any uterine tenderness and auscultation to note the fetal heart rate (5)Inspection of the vulva to note the presence of any active bleeding. (6)Confirmation of diagnosis is made from the history, physical examination and with USG.
- 13. EXPECTANT MANAGEMENT Macafee and Johnson (1945) • The aim is to continue pregnancy for fetal maturity without compromising the maternal health. • Vital prerequisites: (1)Availability of blood for transfusion whenever required (2)Facilities for cesarean section should be available throughout 24 hours. • Selection of cases: (1)Mother is in good health status(hemoglobin > 10 g%; hematocrit > 30%) (2)Duration of pregnancy is less than 37 weeks (3)Active vaginal bleeding is absent (4) Fetal well being is assured (USG).
- 14. (1) Bed rest with bathroom privileges (2) Investigations—like hemoglobin estimation, blood grouping and urine for protein are done (3) Periodic inspection of the vulval pads and fetal surveillance with USG at interval of 2–3 weeks (see p. 244) (4) Supplementary hematinics (5) When the patient is allowed out of the bed (2-3 days after the bleeding stops), a gentle speculum examination is made to exclude local cervical and vaginal lesions for bleeding. (6) Use of tocolysis (magnesium sulfate) can be done if vaginal bleeding is associated with uterine contractions (7) Rh immunoglobin should be given to all Rh negative (unsensitized) women.
- 15. • Expectant management at Hospital or at Home? Hospital setting is ideal. home care may be allowed in some. Selected cases are — (a) patient lives close to hospital (b) 24-hour transportation is available (c) Bed rest assured and (d) patient is well motivated to understand the risks. • Termination of the expectant treatment:37 weeks of pregnancy. • Steroid therapy is indicated when the duration of pregnancy is less than 34 weeks
- 16. ACTIVE MANAGEMENT(DELIVERY) Bleeding occurs at or after 37 weeks of pregnancy Patient is in labor Patient is in exsanguinated state on admission Bleeding is continuing and of moderate degree Baby is dead or known to be congenitally deformed DEFINITIVE MANAGEMENT • Cesarean delivery –placental edge is within 2 cm from the internal os. • Vaginal delivery -placenta edge is clearly 2–3 cm away from the internal cervical os