This document provides an overview of anaemia in pregnancy. It begins with definitions of anaemia and classifications of anaemia severity. It then discusses physiological changes in pregnancy that can cause relative anaemia and describes adaptive mechanisms to ensure adequate oxygen delivery to tissues during anaemia. The document outlines considerations for anaesthesia management and choices between regional and general anaesthesia in pregnant patients with anaemia. It emphasizes techniques to minimize factors that decrease oxygen delivery or increase consumption.



![ADAPTIVE MECHANISMS THAT ENSURE OXYGEN
DELIVERY TO TISSUES
Oxygen sensors
• kidneys,aortic and carotid body chemoreceptors and cells [hypoxia-inducible factor (HIF)].
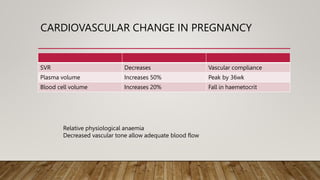
• Adaptive physiological responses occur to compensate for anaemia-induced tissue hypoxia,
which supports cellular survival during anaemia.
The Respiratory adaptations during anaemia
• Increase in minute ventilation due to stimulation of respiration.
NO-mediated mechanisms
• The partial pressure of O2 in arterial blood (PaO2 ) and Hb O2 saturation (SaO2 ) are increased
• Help in ventilation-perfusion matching. This help for maintaining SaO2 in the presence of
reduced Hb](https://image.slidesharecdn.com/laast-231130161547-660e4918/85/anaemia-in-pregnancy-24-320.jpg)