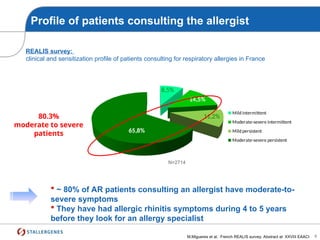
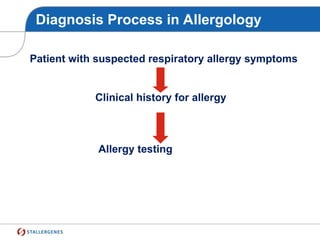
The document outlines a training course agenda focused on the management of allergic patients, highlighting issues in diagnosis and treatment, including the underdiagnosis and undertreatment of allergic rhinitis and asthma. Key discussions include the epidemiology of allergic diseases, challenges in allergen avoidance, pharmacotherapy, and the importance of allergen immunotherapy. Emphasis is placed on patient education, follow-up, and the need for effective communication between doctors and patients to address unmet therapeutic needs.