aki_vs_ckd2015.pdf the differences between aki and ckd
1.
AKI VS CKD
FRACPcourse 2015
OVERVIEW
How to tell the difference between acute and chronic
kidney disease for exam purposes
How to work out whether is it glomerular or tubular and
what the cause is
Some background info time permitting
SOME DEFINITIONS
Chronic Kidney Disease ( chronic renal failure)
Loss of renal function over a prolonged time
This means that there is time for impact on growth,
bones ( aka CKD – MBD or renal osteodystrophy) and
anaemia.
So look for words like short, pale, bones as clues
WHAT’S A GFR
2.
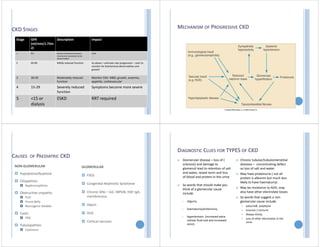
CKD STAGES
Stage GFR
(ml/min/1.73m
2)
DescriptionImpact
1 90+ Normal function but known
structural or persistent urine
abnormalities
Little
2 60‐89 Mildly reduced function As above + estimate rate progression – start to
monitor for biochemical abnormalities and
growth
3 30‐59 Moderately reduced
function
Monitor CKD‐ MBD, growth, anaemia,
appetite, cardiovascular
4 15‐29 Severely reduced
function
Symptoms become more severe
5 <15 or
dialysis
ESKD RRT required
MECHANISM OF PROGRESSIVE CKD
CAUSES OF PAEDIATRIC CKD
NON‐GLOMERULAR
Hypoplasia/dysplasia
Ciliopathies
Nephronopthisis
Obstructive uropathy
PUV
Prune Belly
Neurogenic bladder
Cystic
PKD
Tubulopathies
Cystinosis
GLOMERULAR
FSGS
Congenital Nephrotic Syndrome
Chronic GNs – SLE, MPGN, HSP, IgA,
membranous
Alport
HUS
Cortical necrosis
DIAGNOSTIC CLUES FOR TYPES OF CKD
Glomerular disease – loss of (
sclerosis) and damage to
glomeruli lead to retention of salt
and water, raised renin and loss
of blood and protein in the urine
So words that should make you
think of a glomerular cause
include
oliguria,
haematuria/proteinuria,
hypertension (increased extra
cellular fluid and and increased
renin)
Chronic tubular/tubulointerstitial
diseases – concentrating defect
so loss of salt and water
May have proteinuria ( not all
protein is albumin but much less
likely to have haematuria)
May be resistance to ADH, may
also have other electrolyte losses
So words that suggest a non
glomerular cause include
polyuria& polydipsia
enuresis / nocturia
Always thirsty
Loss of other electrolytes in the
urine
3.
CAUSES OF PAEDIATRICCKD
NON‐GLOMERULAR
Hypoplasia/dysplasia
Ciliopathies
Nephronopthisis
Obstructive uropathy
PUV
Prune Belly
Neurogenic bladder
Cystic
PKD
Tubulopathies
Cystinosis
Clues
CAUSES OF PAEDIATRIC CKD
Clues GLOMERULAR
FSGS
Congenital Nephrotic Syndrome
Chronic GNs – SLE, MPGN, HSP, IgA,
membranous
Alport
HUS
Cortical necrosis
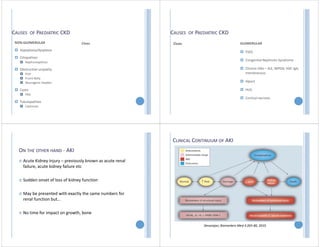
ON THE OTHER HAND ‐ AKI
Acute Kidney Injury – previously known as acute renal
failure, acute kidney failure etc
Sudden onset of loss of kidney function
May be presented with exactly the same numbers for
renal function but…
No time for impact on growth, bone
CLINICAL CONTINUUM OF AKI
Devarajan, Biomarkers Med 4:265‐80, 2010
4.
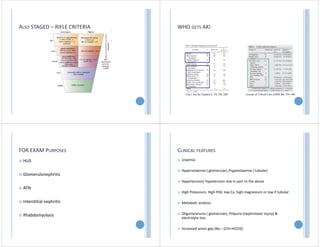
ALSO STAGED –RIFLE CRITERIA WHO GETS AKI
FOR EXAM PURPOSES
HUS
Glomerulonephritis
ATN
Interstitial nephritis
Rhabdomyolysis
CLINICAL FEATURES
Uraemia
Hypervolaemia ( glomerular) /hypovolaemia ( tubular)
Hypertension/ hypotension due in part to the above
High Potassium, High P04, low Ca, high magnesium or low if tubular
Metabolic acidosis
Oliguria/anuria ( glomerular), Polyuria (nephrotoxic injury) &
electrolyte loss
Increased anion gap (Na – (Chl+HCO3))
5.
AKI VS CKD
FRACPcourse 2015
Tonya Kara
PRERENAL AKI
Decreased perfusion to the kidneys, and as a
consequence a reduction in GFR:
True volume depletion :bleeding, intestinal/cutaneous loss
Effective renal hypoperfusion :decreased arterial pressure ‐
heart failure or septic shock or cirrhosis
RENAL
Affects renal parenchyma
Vascular e.g. RVT, TTP, HUS
Glomerular e.g. Post infectious GN, HSP, anti GBM.
Interstitial e.g. pyelonephritis, NSAIDs, diuretics
Tubular e.g. ATN, aminoglycosides. Aciclovir, tumour
lysis
POST RENAL
Affects the drainage of the kidney:
Stones
Bladder outlet obstruction
Trauma/clots
Tumours
Sometimes comes up as a question about post obstructive
polyuria
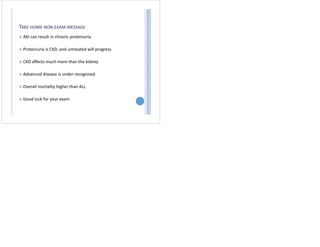
6.
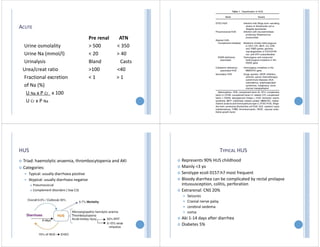
ACUTE
Urine osmolality
Urine Na(mmol/l)
Urinalysis
Urea/creat ratio
Fractional excretion
of Na (%)
U Na x P Cr x 100
U Cr x P Na
Pre renal ATN
> 500 < 350
< 20 > 40
Bland Casts
>100 <40
< 1 > 1
HUS
Triad: haemolytic anaemia, thrombocytopenia and AKI
Categories:
Typical: usually diarrhoea positive
Atypical: usually diarrhoea negative
Pneumococcal
Complement disorders ( low C3)
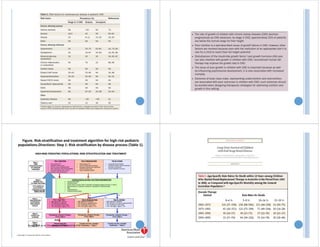
TYPICAL HUS
Represents 90% HUS childhood
Mainly <3 yo
Serotype ecoli 0157:h7 most frequent
Bloody diarrhea can be complicated by rectal prolapse
intussusception, colitis, perforation
Extrarenal: CNS 20%
Seizures
Cranial nerve palsy
cerebral oedema
coma
Aki 1‐14 days after diarrhea
Diabetes 5%
7.
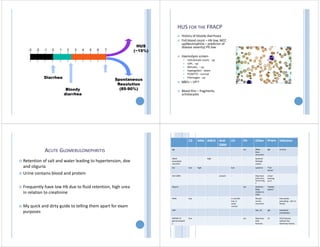
Spontaneous
Resolution
(85-90%)
HUS
(~15%)
-3 -2 -10 1 2 3 4 5 6 7
Diarrhea
Bloody
diarrhea
HUS FOR THE FRACP
History of bloody diarrhoea
Full blood count – Hb low, WCC
up(Neutrophilia – predictor of
disease severity) Plt low
Haemolysis screen‐
reticulocyte count, ‐ up
LDH, ‐ up
Bilirubin, ‐ up
haptoglobin ‐ down
PT/APTT/ ‐ normal
Fibrinogen ‐ up
U&Es – UP!!
Blood film – fragments,
schistocytes
ACUTE GLOMERULONEPHRITIS
Retention of salt and water leading to hypertension, doe
and oliguria
Urine contains blood and protein
Frequently have low Hb due to fluid retention, high urea
in relation to creatinine
My quick and dirty guide to telling them apart for exam
purposes
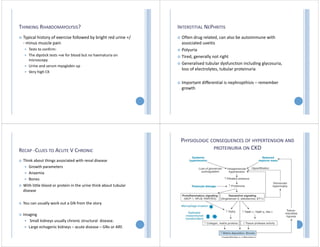
C3 ANA ANCA Anti
GBM
C4 FH Other Biopsy Infection
IgA ‐ ‐ ‐ ‐ ‐ occ Often
boys
recurrent
IgA At time
ANCA
associated
vasculitis
‐ ‐ High ‐ ‐ ‐ Systemic
Multiple
causes
‐
SLE low high low systemic “Full
house”
‐
Anti GBM ‐ ‐ ‐ present ‐ ‐ May have
pulmonary
haenorrhag
e
Linear
staining
on IF
‐
Alports ‐ ‐ ‐ ‐ ‐ yes Deafness
Male
relative in
ESKD
“basket
weave”
‐
PIGN low ‐ ‐ ‐ In real life
low, in
exam
normal
‐ Should
not be
recurrent
Few weeks
preceding – skin or
throat
HSP ‐ ‐ ‐ ‐ ‐ ‐ Skin, GI IgA Sometime
precipitates
MPGN/ C3
glomerulopath
y
low ‐ ‐ ‐ ‐ occ May have
HUS
features
C3 HUS features
without the
diarrhoea history
8.
THINKING RHABDOMAYOLYSIS?
Typicalhistory of exercise followed by bright red urine +/
‐ minus muscle pain
Tests to confirm:
The dipstick tests +ve for blood but no haematuria on
microscopy
Urine and serum myoglobin up
Very high CK
INTERSTITIAL NEPHRITIS
Often drug related, can also be autoimmune with
associated uveitis
Polyuria
Tired, generally not right
Generalised tubular dysfunction including glycosuria,
loss of electrolytes, tubular proteinuria
Important differential is nephropthisis – remember
growth
RECAP ‐CLUES TO ACUTE V CHRONIC
Think about things associated with renal disease
Growth parameters
Anaemia
Bones
With little blood or protein in the urine think about tubular
disease
You can usually work out a GN from the story
Imaging
Small kidneys usually chronic structural disease.
Large echogenic kidneys – acute disease – GNs or ARF.
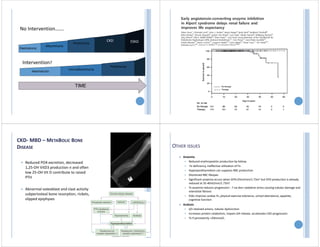
PHYSIOLOGIC CONSEQUENCES OF HYPERTENSION AND
PROTEINURIA ON CKD
9.
TIME
Haematuria
microalbuminuria
Proteinuria
No Intervention…….
Intervention?
Albuminuria
Proteinuria
CKD ESKD
Haematuria
CKD‐MBD – METABOLIC BONE
DISEASE
Reduced PO4 excretion, decreased
1,25‐OH VitD3 production n and often
low 25‐OH Vit D contribute to raised
PTH
Abnormal osteoblast and clast activity
subperiosteal bone resorption, rickets,
slipped epiphyses
OTHER ISSUES
Anaemia
Reduced erythropoietin production by kidney
Fe deficiency, ineffective utilisation of Fe
Hyperparathyroidism can suppress RBC production
Shortened RBC lifespan
Significant anaemia occurs when GFR<25ml/min/1.73m2 but EPO production is already
reduced at 35‐40ml/min/1.73m2
Tx anaemia reduces progression ‐ ? via decr oxidative stress causing tubular damage and
interstitial fibrosis
ESAs improve cardiac fn, physical exercise tolerance, school attendance, appetite,
cognitive function
Acidosis
d/t retained anions, tubular dysfunction
Increases protein catabolism, impairs GH release, accelerates CKD progression
Tx if persistently <20mmol/L
TAKE HOME NONEXAM MESSAGE
AKI can result in chronic proteinuria
Proteinuria is CKD, and untreated will progress
CKD affects much more than the kidney
Advanced disease is under recognised
Overall mortality higher than ALL
Good luck for your exam