Download as PDF, PPTX

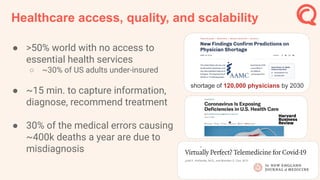

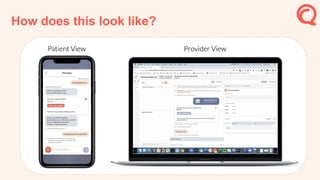


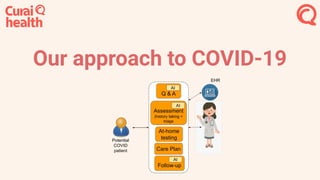
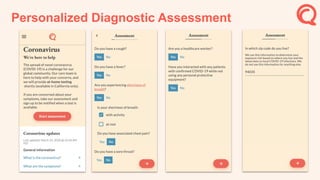
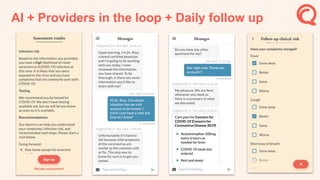

The document discusses the integration of AI technology in healthcare to enhance accessibility, quality, and efficiency, particularly in light of the COVID-19 pandemic. It emphasizes a collaborative approach where AI aids human providers, utilizing data feedback loops for continuous learning and improvement in medical diagnostics. The content also outlines AI-driven innovations in medical conversations, diagnosis through expert systems, and addressing healthcare challenges through tailored AI applications.






















































































