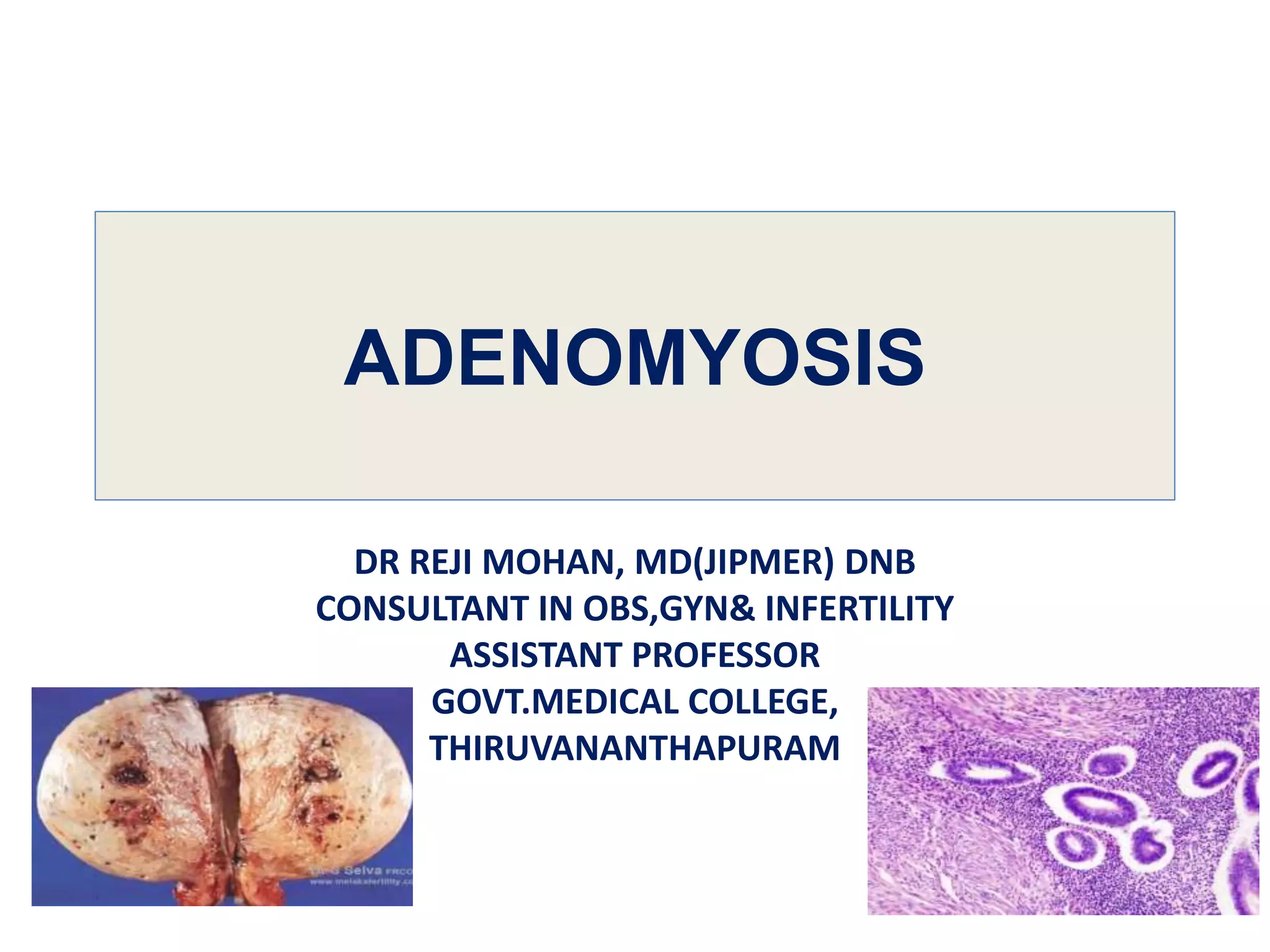
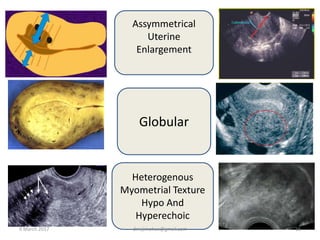
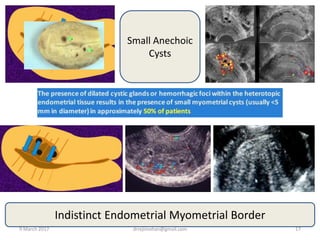
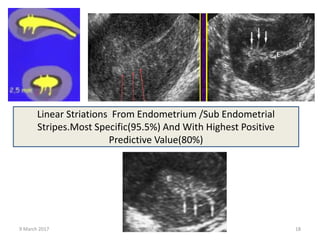
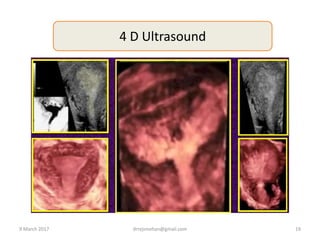
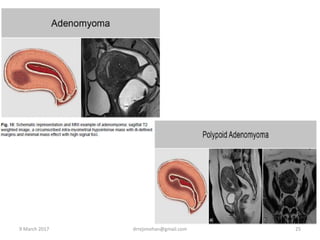
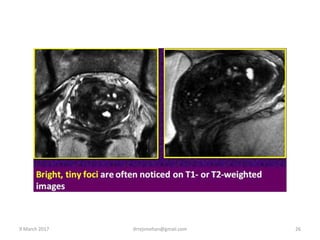
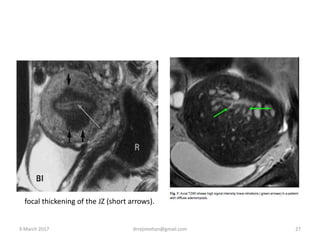
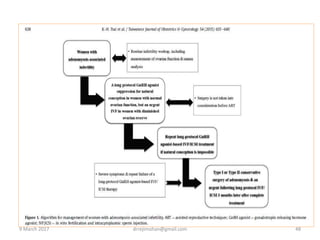
Dr. Reji Mohan provides an overview of adenomyosis. He discusses that adenomyosis is characterized by the presence of ectopic endometrial glands and stroma within the myometrium. Symptoms can include dysmenorrhea, menorrhagia, chronic pelvic pain, and subfertility. Diagnosis involves transvaginal ultrasound or MRI to detect thickening of the junctional zone or intramyometrial cysts and striations. Treatment options include medical management with hormonal therapies or surgical interventions like hysterectomy or conservative surgeries. Adenomyosis can impact fertility by altering uterine function and receptivity.