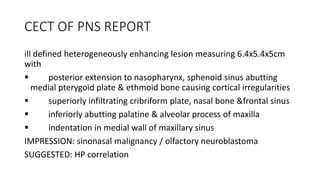
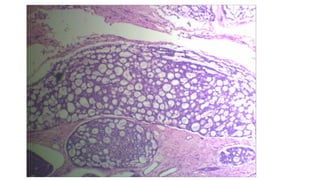
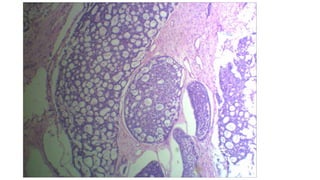
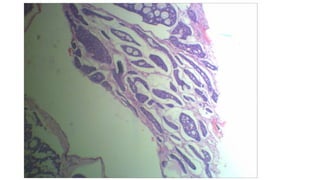
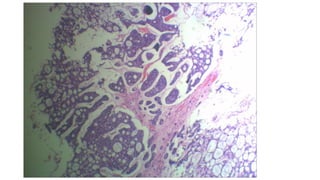
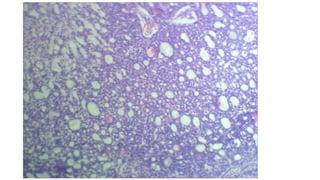
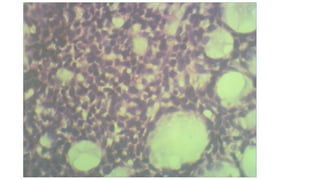
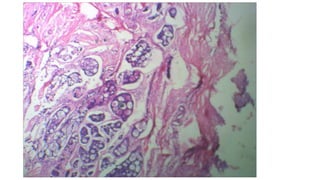
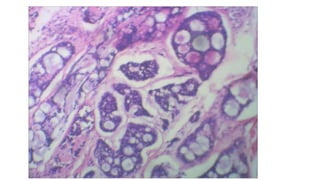
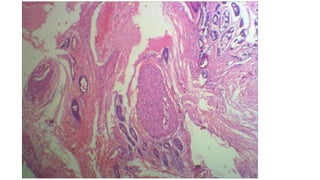
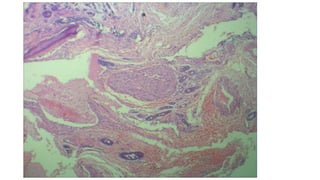
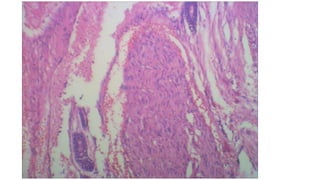
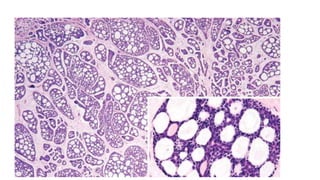
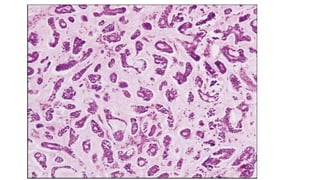
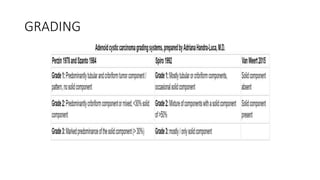
This document describes a case of adenoid cystic carcinoma found in a woman's right nasal cavity. Key details include that the tumor measured 6.4x5.4x5cm and had extended into surrounding areas. Microscopic examination revealed the tumor had cribriform, tubular, and solid growth patterns typical of adenoid cystic carcinoma, with perineural invasion. This rare type of cancer is known to spread along cranial nerves or hematogenously to distant sites like the lungs. Treatment involves wide surgical excision and radiation therapy, with prognosis depending on growth pattern and extent of disease.











































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
