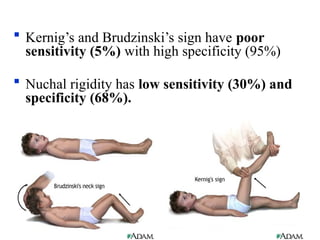
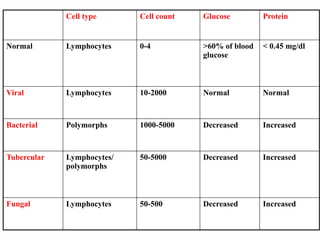
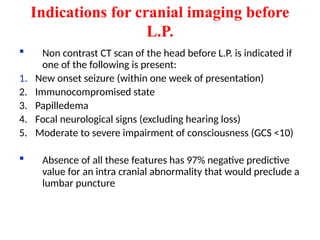
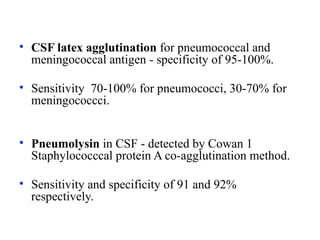
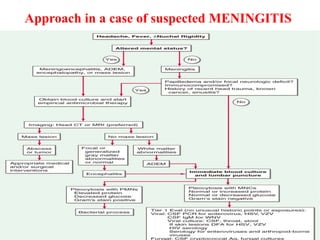
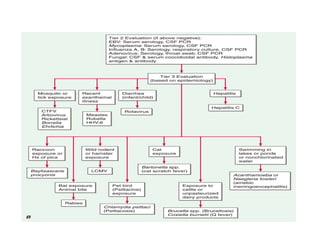
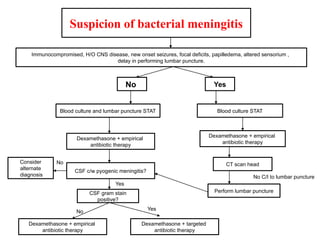
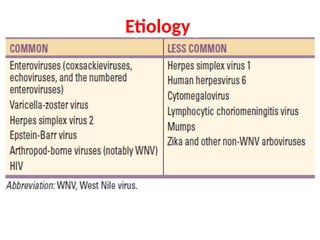
The document provides a comprehensive overview of meningitis, including its types, causes, clinical presentation, investigations, and management strategies. It covers acute, subacute, and chronic forms, detailing the causative organisms and their associated risk factors, as well as diagnostic procedures like lumbar puncture and treatment protocols. Additionally, it emphasizes the importance of early antibiotic therapy and the use of corticosteroids to improve patient outcomes.

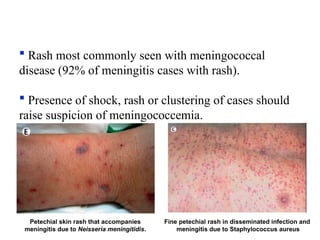









































![DKA_,HHS[1].pptxbzhsjdkdkdbjddoeohjsisksjsj](https://cdn.slidesharecdn.com/ss_thumbnails/dkahhs1-240727120718-47e868a7-thumbnail.jpg?width=640&height=640&fit=bounds)





















