Chief Complaints
A 48year old male was brought to the ER with
complaints of:
• Fever since 5days
• Absence of urine output for 1 day
• Shortness of breath since 1day
• Palpitations since 2hrs
3.
Presentation to hospital
Patientwas apparently normal 3 days back when patient
developed
• Fever since 5days,last episode 1day ago,high grade ,
intermittent associated with chills,myalgia and
athralgia,and fatigue since 5days,relieved with
medication.
• Complete absence of urine output for 1day
• Shortness of breath grade-4 since 1day which is sudden
in onset progressive associated with orthopnea , no pnd,
• Palpitations since 2 hrs sudden in onset ,aggrevated on
work, not progressive , not associated with chestpain or
sweating
4.
• No historyof headache, neck pain, burning
micturition, vomiting,loose stools, chest pain, cough
• No burning and tingling sensations of arms and legs
5.
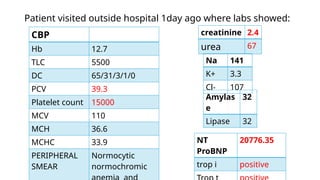
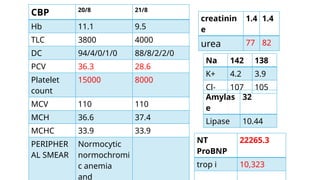
CBP
Hb 12.7
TLC 5500
DC65/31/3/1/0
PCV 39.3
Platelet count 15000
MCV 110
MCH 36.6
MCHC 33.9
PERIPHERAL
SMEAR
Normocytic
normochromic
creatinine 2.4
urea 67
Na 141
K+ 3.3
Cl- 107
Amylas
e
32
Lipase 32
NT
ProBNP
20776.35
trop i positive
Patient visited outside hospital 1day ago where labs showed:
• USG showedhepatomegaly with altered increased
echotexture –Alcohol liver disease ,cholelithiasis with sludge
in gb lumen.
• Foleys catheterisation done and got treated with ionotropes,
antibiotics and other supportive medication for 1 day ,one
sdp transfusion was also done. Patient was referred to
PSIMS & RF for further evaluation and management.
• Patient diagnosed as viral fever with thrombocytopenia
with heart failure ?cause
8.
PAST HISTORY
• Nota k/c/o DM,HTN , CKD ,CAD, CLD, epilepsy,
thyroid disorders, BA, COPD
PERSONAL HISTORY
• known smoker since 5 years -10 cigerettes per day-
2.5pack years
Occasional alcoholic since 25 yrs drinks 180ml/day .
• No history of drug/ food allergies
FAMILY HISTORY- nil
9.
Initial Evaluation
• Patientwas conscious and oriented to time, place and
person at the time of presentation.
• Moderately built, moderately nourished
• No pallor, icterus,cyanosis, clubbing, lymphadenopathy,
edema
• Petechia present on soft palate
• Gum bleed present
10.
• Vitals atpresentation:
BP: 100/60mmhg on 12.5mic/hr nor adrenaline, 3.8meq/hr
dobutamine
PR: 100/min
RR: 34/min
Temp: 98.7F
spO2: 89% on 10l O2
GRBS: 84 mg/ dL
Hess test-positive
11.
Systemic Examination
RS:
• Tracheain midline
• No scars sinuses engorged veins
• Bilateral symmetrical chest movement
• No bony tenderness present
• Bilateral air entry +
• Bilateral coarse crepts with wheeze present in isa ssa iaa
12.
GIT:
• Abdomen isdistended
• Umbilicus in midline and inverted
• All quadrants move equally with respiration
• On palpation
no organomegaly
soft tender in all quadrants
• On auscultation bowel sound heard
13.
CVS:
• No visibleprecordial bulge present
• Apex beat felt in 5 th ICS ½ inch medial to midclavicular line
• On auscultation : S1 S2 heard
• S3 present
• No murmurs
CNS:
• GCS = E4V5M6
• PUPILS – BL NSRL
• No signs of meningeal irritation
• B/l plantars - flexor
14.
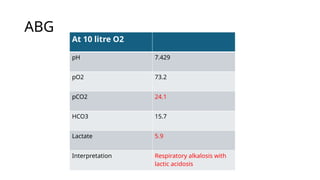
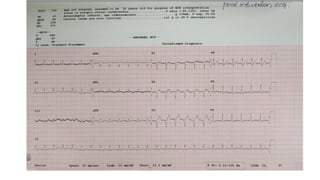
ABG
At 10 litreO2
pH 7.429
pO2 73.2
pCO2 24.1
HCO3 15.7
Lactate 5.9
Interpretation Respiratory alkalosis with
lactic acidosis
Treatment History
In ER
•Case was shifted to MICU and pt was kept on BIPaP i/v/o tachypnoea
In ICU:
• i/v fluids 1NS ,1RL @75 ml/hr
• Inj. noradrenaline infusion at 12.5mic/hr
• Inj. dobutamine infusion at 3.6meq/ hr
• inj meropenem 1gm iv 12th hrly
• Inj. Pantop 40 mg IV 24th
hrly
• inj . Thiamine 500mg stat in 100 ml NS followed by 100 mg in 100ml NS 8th
hrly
• inj zofer 4 mg iv 12th
hrly
• tab atorvas 20 mg po 24th
hrly
• TAB Chlordiazepoxide 25 mg po 8th
hrly
• Input/ output charting
• Vitals monitoring
24.
Course in thehospital
• Patient was shifted to ICU and was put on BiPap initially
due to tachypnoea , as there is persistent increase in work
of breathing patient and pt became drowsy was sedated
and intubated on 21th
August 2025 at 5:00AM.
• mode -vc
• tv-420 ml
• fio2-80 %
• rr-14/ min
• i:e -1:2
• peep- 5 cm h20
25.
• Vitals:
Pre-intubation
BP: 100/60mmhgon 12.5mic/hr
nor adrenaline,3.6meq/hr dobutamine
PR: 130/min
RR: 50/min
spO2: 95% on niv 75%
Post intubation
BP: 120/60mmhg on 12.5mic/hr
nor adrenaline, 3.6meq/hr dobutamine
PR: 130/min
RR: 20/min
spO2: 98% on 80% fio2
27.
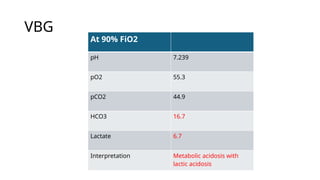
VBG
At 90% FiO2
pH7.239
pO2 55.3
pCO2 44.9
HCO3 16.7
Lactate 6.7
Interpretation Metabolic acidosis with
lactic acidosis
28.
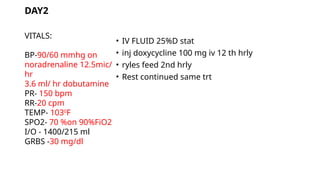
• IV FLUID25%D stat
• inj doxycycline 100 mg iv 12 th hrly
• ryles feed 2nd hrly
• Rest continued same trt
VITALS:
BP-90/60 mmhg on
noradrenaline 12.5mic/
hr
3.6 ml/ hr dobutamine
PR- 150 bpm
RR-20 cpm
TEMP- 1030
F
SPO2- 70 %on 90%FiO2
I/O - 1400/215 ml
GRBS -30 mg/dl
DAY2
29.
• While onmechanical ventilation patient suddenly got desaturated
with non palpable carotids at 10.04am on 21th
August, 2025. High
quality CPR was initiated according to ACLS guidelines.
• Despite adequate resuscitative efforts patient could not be revived
and ECG showed flatline at 10.39am on 21th
august 2025.

























![SOUVIK BERA BWU-BPA-20-014[2].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/souvikberabwu-bpa-20-0142-240128070156-9bf3a914-thumbnail.jpg?width=640&height=640&fit=bounds)















![DKA_,HHS[1].pptxbzhsjdkdkdbjddoeohjsisksjsj](https://cdn.slidesharecdn.com/ss_thumbnails/dkahhs1-240727120718-47e868a7-thumbnail.jpg?width=640&height=640&fit=bounds)





















