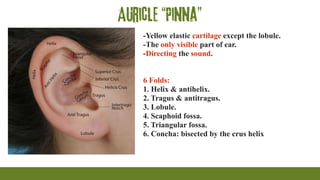
Auricle “Pinna”
-Yellow elasticcartilage except the lobule.
-The only visible part of ear.
-Directing the sound.
6 Folds:
1. Helix & antihelix.
2. Tragus & antitragus.
3. Lobule.
4. Scaphoid fossa.
5. Triangular fossa.
6. Concha: bisected by the crus helix
4.
External auditory canal
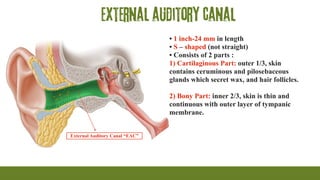
ExternalAuditory Canal “EAC”
• 1 inch-24 mm in length
• S – shaped (not straight)
• Consists of 2 parts :
1) Cartilaginous Part: outer 1/3, skin
contains ceruminous and pilosebaceous
glands which secret wax, and hair follicles.
2) Bony Part: inner 2/3, skin is thin and
continuous with outer layer of tympanic
membrane.
5.
Tympanic membrane
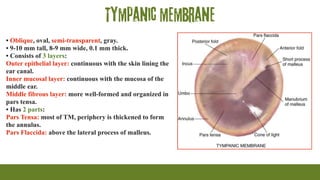
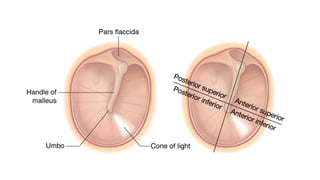
• Oblique,oval, semi-transparent, gray.
• 9-10 mm tall, 8-9 mm wide, 0.1 mm thick.
• Consists of 3 layers:
Outer epithelial layer: continuous with the skin lining the
ear canal.
Inner mucosal layer: continuous with the mucosa of the
middle ear.
Middle fibrous layer: more well-formed and organized in
pars tensa.
• Has 2 parts:
Pars Tensa: most of TM, periphery is thickened to form
the annulus.
Pars Flaccida: above the lateral process of malleus.
7.
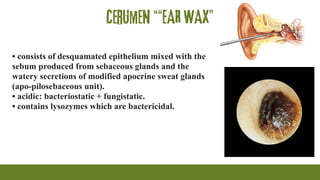
Cerumen ““EAR WAX”
•consists of desquamated epithelium mixed with the
sebum produced from sebaceous glands and the
watery secretions of modified apocrine sweat glands
(apo-pilosebaceous unit).
• acidic: bacteriostatic + fungistatic.
• contains lysozymes which are bactericidal.
8.
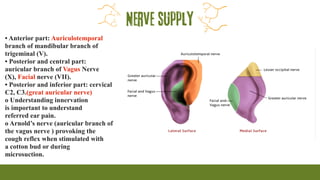
Nerve supply
• Anteriorpart: Auriculotemporal
branch of mandibular branch of
trigeminal (V).
• Posterior and central part:
auricular branch of Vagus Nerve
(X), Facial nerve (VII).
• Posterior and inferior part: cervical
C2, C3.(great auricular nerve)
o Understanding innervation
is important to understand
referred ear pain.
o Arnold’s nerve (auricular branch of
the vagus nerve ) provoking the
cough reflex when stimulated with
a cotton bud or during
microsuction.
9.
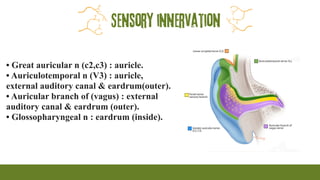
Sensory innervation
• Greatauricular n (c2,c3) : auricle.
• Auriculotemporal n (V3) : auricle,
external auditory canal & eardrum(outer).
• Auricular branch of (vagus) : external
auditory canal & eardrum (outer).
• Glossopharyngeal n : eardrum (inside).
10.
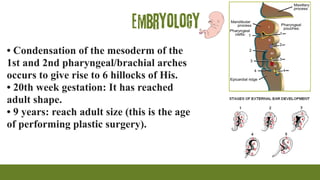
Embryology
• Condensation ofthe mesoderm of the
1st and 2nd pharyngeal/brachial arches
occurs to give rise to 6 hillocks of His.
• 20th week gestation: It has reached
adult shape.
• 9 years: reach adult size (this is the age
of performing plastic surgery).
11.
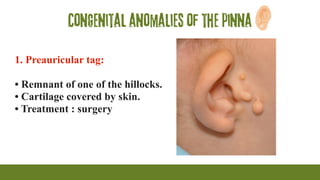
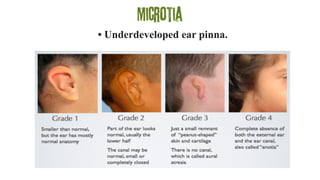
Congenital anomalies ofthe pinna
1. Preauricular tag:
• Remnant of one of the hillocks.
• Cartilage covered by skin.
• Treatment : surgery
12.
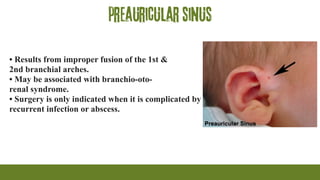
preauricular sinus
• Resultsfrom improper fusion of the 1st &
2nd branchial arches.
• May be associated with branchio-oto-
renal syndrome.
• Surgery is only indicated when it is complicated by
recurrent infection or abscess.
Trauma to theauricle
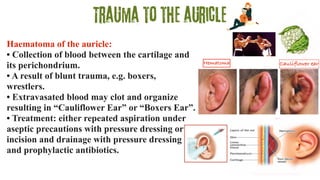
Haematoma of the auricle:
• Collection of blood between the cartilage and
its perichondrium.
• A result of blunt trauma, e.g. boxers,
wrestlers.
• Extravasated blood may clot and organize
resulting in “Cauliflower Ear” or “Boxers Ear”.
• Treatment: either repeated aspiration under
aseptic precautions with pressure dressing or
incision and drainage with pressure dressing
and prophylactic antibiotics.
Hematoma Cauliflower ear
16.
Infections of theauricle
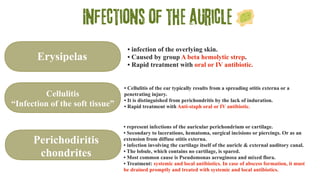
Erysipelas
Cellulitis
“Infection of the soft tissue”
Perichodiritis
chondrites
• infection of the overlying skin.
• Caused by group A beta hemolytic strep.
• Rapid treatment with oral or IV antibiotic.
• Cellulitis of the ear typically results from a spreading otitis externa or a
penetrating injury.
• It is distinguished from perichondritis by the lack of induration.
• Rapid treatment with Anti-staph oral or IV antibiotic.
• represent infections of the auricular perichondrium or cartilage.
• Secondary to lacerations, hematoma, surgical incisions or piercings. Or as an
extension from diffuse otitis externa.
• infection involving the cartilage itself of the auricle & external auditory canal.
• The lobule, which contains no cartilage, is spared.
• Most common cause is Pseudomonas aeruginosa and mixed flora.
• Treatment: systemic and local antibiotics. In case of abscess formation, it must
be drained promptly and treated with systemic and local antibiotics.
17.
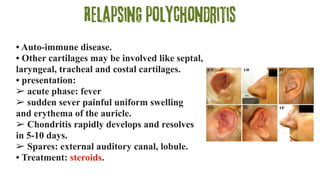
Relapsing polychondritis
• Auto-immunedisease.
• Other cartilages may be involved like septal,
laryngeal, tracheal and costal cartilages.
• presentation:
➢ acute phase: fever
➢ sudden sever painful uniform swelling
and erythema of the auricle.
➢ Chondritis rapidly develops and resolves
in 5-10 days.
➢ Spares: external auditory canal, lobule.
• Treatment: steroids.
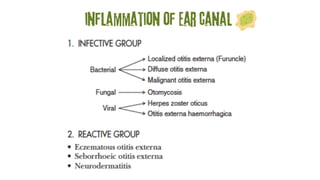
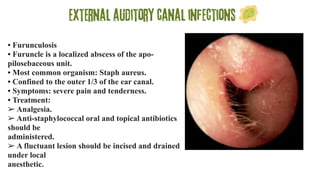
External auditory canalinfections
• Furunculosis
• Furuncle is a localized abscess of the apo-
pilosebaceous unit.
• Most common organism: Staph aureus.
• Confined to the outer 1/3 of the ear canal.
• Symptoms: severe pain and tenderness.
• Treatment:
➢ Analgesia.
➢ Anti-staphylococcal oral and topical antibiotics
should be
administered.
➢ A fluctuant lesion should be incised and drained
under local
anesthetic.
20.
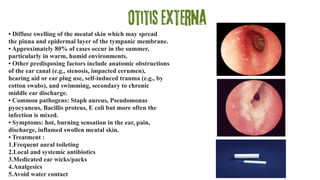
Otitis media
• Diffuseswelling of the meatal skin which may spread to
the pinna and epidermal layer of the tympanic membrane.
• Approximately 80% of cases occur in the summer,
particularly in warm, humid environments.
• Other predisposing factors include anatomic obstructions
of the ear canal (e.g., stenosis, impacted cerumen),
hearing aid or ear plug use, self-induced trauma (e.g., by
cotton swabs), and swimming, secondary to chronic
middle ear discharge.
• Common pathogens: Staph aureus, Pseudomonas
pyocyaneus, Bacillis proteus, E coli but more often the
infection is mixed.
• Symptoms: hot, burning sensation in the ear, pain,
discharge, inflamed swollen meatal skin.
• Treatment :
1.Frequent aural toileting
2.Local and systemic antibiotics
3.Medicated ear wicks/packs
4.Analgesics
5.Avoid water contact
21.
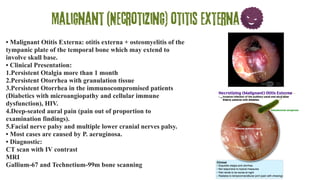
Malignant (Necrotizing) otitisexterna
• Malignant Otitis Externa: otitis externa + osteomyelitis of the
tympanic plate of the temporal bone which may extend to
involve skull base.
• Clinical Presentation:
1.Persistent Otalgia more than 1 month
2.Persistent Otorrhea with granulation tissue
3.Persistent Otorrhea in the immunocompromised patients
(Diabetics with microangiopathy and cellular immune
dysfunction), HIV.
4.Deep-seated aural pain (pain out of proportion to
examination findings).
5.Facial nerve palsy and multiple lower cranial nerves palsy.
• Most cases are caused by P. aeruginosa.
• Diagnostic:
CT scan with IV contrast
MRI
Gallium-67 and Technetium-99m bone scanning
22.
• Treatment:
1. Regularaural toilet.
2. Blood sugar control.
3. Correct immunodeficiency if possible.
4. Pain killer.
5. IV antibiotic for 6-8 weeks, with anti-
pseudomonal coverage (gentamicin +
ticarcillin or ceftazidime + aminoglycoside or
quinolones like ciprofloxacin).
• Prognosis:
Mortality is 5-20%.
23.
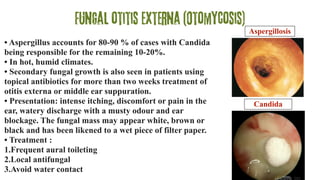
Fungal otitis externa(Otomycosis)
• Aspergillus accounts for 80-90 % of cases with Candida
being responsible for the remaining 10-20%.
• In hot, humid climates.
• Secondary fungal growth is also seen in patients using
topical antibiotics for more than two weeks treatment of
otitis externa or middle ear suppuration.
• Presentation: intense itching, discomfort or pain in the
ear, watery discharge with a musty odour and ear
blockage. The fungal mass may appear white, brown or
black and has been likened to a wet piece of filter paper.
• Treatment :
1.Frequent aural toileting
2.Local antifungal
3.Avoid water contact
Aspergillosis
Candida
24.
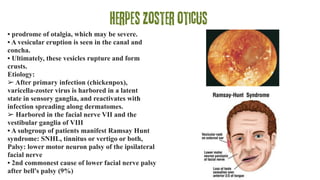
Herpes zoster oticus
•prodrome of otalgia, which may be severe.
• A vesicular eruption is seen in the canal and
concha.
• Ultimately, these vesicles rupture and form
crusts.
Etiology:
➢ After primary infection (chickenpox),
varicella-zoster virus is harbored in a latent
state in sensory ganglia, and reactivates with
infection spreading along dermatomes.
➢ Harbored in the facial nerve VII and the
vestibular ganglia of VIII
• A subgroup of patients manifest Ramsay Hunt
syndrome: SNHL, tinnitus or vertigo or both,
Palsy: lower motor neuron palsy of the ipsilateral
facial nerve
• 2nd commonest cause of lower facial nerve palsy
after bell's palsy (9%)
25.
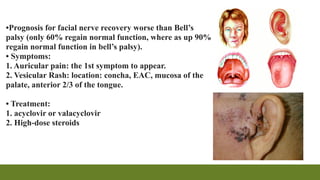
•Prognosis for facialnerve recovery worse than Bell’s
palsy (only 60% regain normal function, where as up 90%
regain normal function in bell’s palsy).
• Symptoms:
1. Auricular pain: the 1st symptom to appear.
2. Vesicular Rash: location: concha, EAC, mucosa of the
palate, anterior 2/3 of the tongue.
• Treatment:
1. acyclovir or valacyclovir
2. High-dose steroids