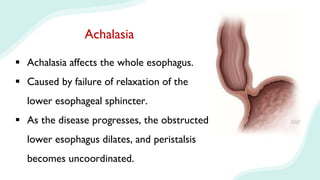
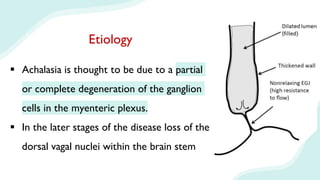
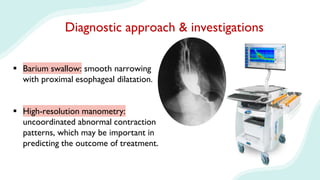
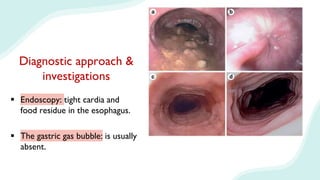
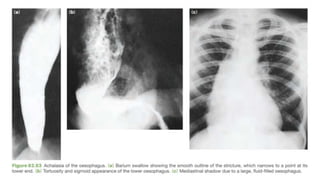
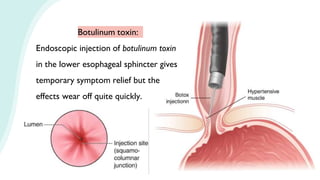
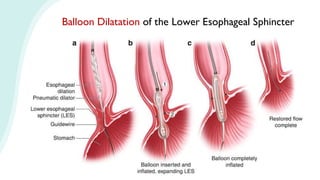
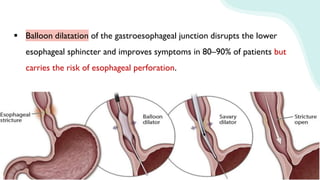
Achalasia is a condition caused by failure of relaxation of the lower esophageal sphincter. It affects the whole esophagus and is caused by degeneration of ganglion cells in the esophageal wall. Clinical manifestations include progressive dysphagia, regurgitation of undigested food, weight loss, and chest pain. Diagnosis involves barium swallow, high-resolution manometry, and endoscopy showing dilated esophagus and food residue. Treatment options include botulinum toxin injection, balloon dilatation, and Heller myotomy to disrupt the lower esophageal sphincter and improve symptoms.









































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


