This document discusses abdominal tuberculosis, including its etiology, pathogenesis, clinical presentation, diagnosis and treatment. Some key points include:
- Abdominal tuberculosis can involve the gastrointestinal tract, peritoneum, liver and spleen and is caused by Mycobacterium tuberculosis spreading hematogenously from a primary pulmonary infection.
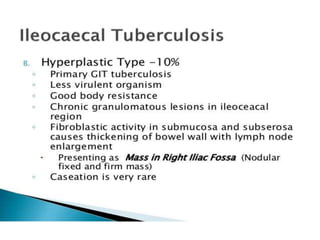
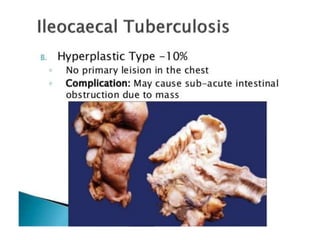
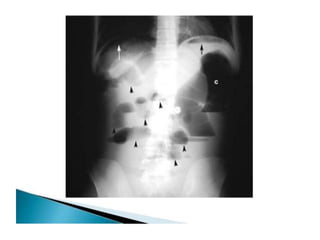
- Clinical manifestations depend on the site of involvement but commonly include abdominal pain, weight loss, fever and intestinal obstruction or perforation from strictures or ulcers. Chest x-rays often do not show evidence of pulmonary lesions.
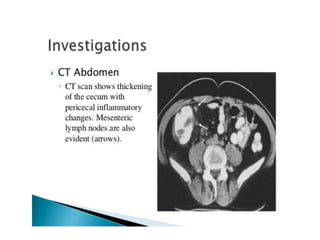
- Diagnosis involves biopsy of affected tissue to identify granulomas and acid-fast bacilli on staining, and culturing bacteria. Abdominal tuberculosis is more common