Introduction
•Abdominal radiography isone of the most important first-line imaging
methods in patients presenting with acute abdominal symptoms.
•When intestinal obstruction is suspected, basic abdominal projections
such as supine, erect, and decubitus views play a crucial role in the
initial evaluation.
•Intestinal obstruction is the blockage that keeps the food or liquid from
passing through the small and large intestine.
•Causes of intestinal obstruction may include adhesions, hernias, colon
cancer, certain medications
Brief Overview of Intestinal
Obstruction
• Confirmation ofObstruction: Imaging can confirm the presence
of a blockage and determine if it's a true mechanical obstruction or
another issue, like constipation or functional ileus.
• Localization: Imaging precisely pinpoints where the obstruction is
located within the digestive tract.
• Cause Identification: It helps determine the underlying cause of
the obstruction, such as post surgical adhesions, hernias, tumors,
or strictures from inflammatory conditions like Crohn’s disease.
• Perforation: Identifying if the bowel has perforated, a life-
threatening complication.
Key Reasons For Imaging
6.
Radiographic
Projections
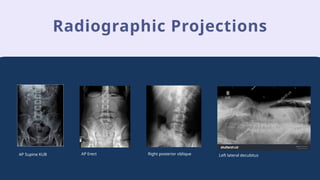
•A radiographic projectionof the abdomen may involve different
projections or a singular one, depending on the physician’s and
the patient’s needs.
•The most common or frequently used projection to examine the
abdomen is the AP Supine projection, also known as the KUB
(Kidney, Ureters & Bladder) projection because it includes these
three important anatomies. Along with these we have other
supplementary views such as AP Erect, Left Lateral Decubitus,
Right & Left Posterior Obliques, Lateral Abdomen and many
more.
7.
Radiographic Projections
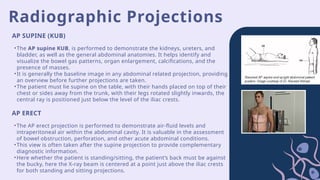
•The APsupine KUB, is performed to demonstrate the kidneys, ureters, and
bladder, as well as the general abdominal anatomies. It helps identify and
visualize the bowel gas patterns, organ enlargement, calcifications, and the
presence of masses.
•It is generally the baseline image in any abdominal related projection, providing
an overview before further projections are taken.
•The patient must lie supine on the table, with their hands placed on top of their
chest or sides away from the trunk, with their legs rotated slightly inwards, the
central ray is positioned just below the level of the iliac crests.
AP SUPINE (KUB)
AP ERECT
•The AP erect projection is performed to demonstrate air-fluid levels and
intraperitoneal air within the abdominal cavity. It is valuable in the assessment
of bowel obstruction, perforation, and other acute abdominal conditions.
•This view is often taken after the supine projection to provide complementary
diagnostic information.
•Here whether the patient is standing/sitting, the patient’s back must be against
the bucky, here the X-ray beam is centered at a point just above the iliac crests
for both standing and sitting projections.
8.
Radiographic Projections
RIGHT &LEFT POSTERIOR OBLIQUE LEFT LATERAL DECUBITUS
•This view is performed when the patient
cannot stand for an erect projection. It is used
to detect intraperitoneal air and air-fluid levels.
•The left side is preferred so that when the free
air rises along the right lateral abdominal wall
and the lateral margin of the liver it can be
easily distinguished from the gastric bubble.
•The x-ray beam is horizontally centered at a
point just above the iliac crest (about 1cm), the
exposure is also taken on arrested expiration.
•The oblique projections (RPO and LPO) are
used to visualize the structures of the
abdomen such as the kidneys (right and left)
in a different plane, helping to detect
localized lesions, calcifications, abnormal
opacities at the renal tract.
•They are particularly useful for
differentiating overlapping structures and
assessing the position of organs.
•For the examination targeted towards the
lower abdomen region the patient is asked
to raise the right or left side of their body
depending on the examination to about 30-
45 and the beam centered between the
symphysis pubis and superior iliac crest.
9.
LATERAL ABDOMEN
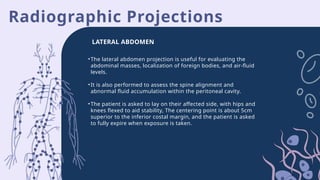
•The lateralabdomen projection is useful for evaluating the
abdominal masses, localization of foreign bodies, and air-fluid
levels.
•It is also performed to assess the spine alignment and
abnormal fluid accumulation within the peritoneal cavity.
•The patient is asked to lay on their affected side, with hips and
knees flexed to aid stability, The centering point is about 5cm
superior to the inferior costal margin, and the patient is asked
to fully expire when exposure is taken.
Radiographic Projections
Radiographic Findings
“Radiographic findingsare the visible results or evidence that is seen on an
X-ray image ”
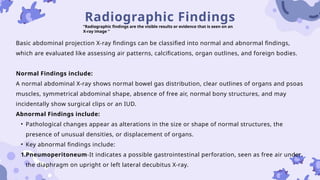
Basic abdominal projection X-ray findings can be classified into normal and abnormal findings,
which are evaluated like assessing air patterns, calcifications, organ outlines, and foreign bodies.
Normal Findings include:
A normal abdominal X-ray shows normal bowel gas distribution, clear outlines of organs and psoas
muscles, symmetrical abdominal shape, absence of free air, normal bony structures, and may
incidentally show surgical clips or an IUD.
Abnormal Findings include:
• Pathological changes appear as alterations in the size or shape of normal structures, the
presence of unusual densities, or displacement of organs.
• Key abnormal findings include:
1.Pneumoperitoneum-It indicates a possible gastrointestinal perforation, seen as free air under
the diaphragm on upright or left lateral decubitus X-ray.
12.
Radiographic Findings
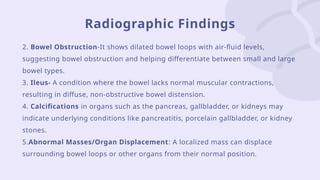
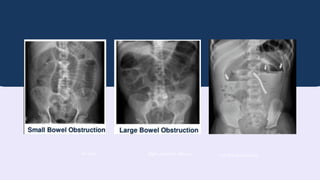
2. BowelObstruction-It shows dilated bowel loops with air-fluid levels,
suggesting bowel obstruction and helping differentiate between small and large
bowel types.
3. Ileus- A condition where the bowel lacks normal muscular contractions,
resulting in diffuse, non-obstructive bowel distension.
4. Calcifications in organs such as the pancreas, gallbladder, or kidneys may
indicate underlying conditions like pancreatitis, porcelain gallbladder, or kidney
stones.
5.Abnormal Masses/Organ Displacement: A localized mass can displace
surrounding bowel loops or other organs from their normal position.
13.
Radiographic Findings
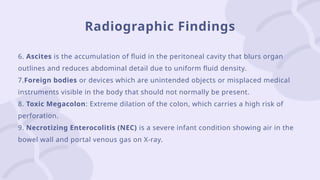
6. Ascitesis the accumulation of fluid in the peritoneal cavity that blurs organ
outlines and reduces abdominal detail due to uniform fluid density.
7.Foreign bodies or devices which are unintended objects or misplaced medical
instruments visible in the body that should not normally be present.
8. Toxic Megacolon: Extreme dilation of the colon, which carries a high risk of
perforation.
9. Necrotizing Enterocolitis (NEC) is a severe infant condition showing air in the
bowel wall and portal venous gas on X-ray.
Imaging plays avery important role in the diagnosis and evaluation of intestinal obstruction.
•Among various modalities available, the plain abdominal radiograph (X-ray) is typically, the first thing
to do due to its wide availability, rapid acquisition, and cost-effectiveness.
•A well-performed abdomen X-ray assists in identifying characteristic features such as dilated bowel
loops, air-fluid levels, and absence of gas in distal bowel, all of which are key indicators of intestinal
obstruction.
•Although plain radiography may not provide an accurate result for every case, it serves as an essential
initial screening tool, guiding clinicians toward appropriate further imaging or intervention.
•Despite the value and cost effectiveness, plain abdomen radiographs have limitations. They often lack
specificity for certain use cases, particularly in cases of partial or early obstruction.
•Overall, imaging plays a very important role not only in identifying the obstruction but also in
monitoring disease progression and guiding treatment, ensuring optimal recovery and patient safety.
Conclusion
16.
Bibliography
1
Long, B. W.., Smith, B. J. ., & Merrill, Vinita. (2016). Merrill’s atlas of radiographic
positioning & procedures.
Morgan, M., Murphy, A., & Er, A. (2015). Abdomen (AP supine view). Radiopaedia.Org.
https://doi.org/10.53347/RID-38090
Morgan, M., Murphy, A., & Jones, J. (2015). Abdomen (PA erect view).
Radiopaedia.Org. https://doi.org/10.53347/RID-38091
2
3
4
vdoc.pub_clarks-positioning-in-radiography-13e.pdf - Google Drive. (n.d.).
Retrieved October 5, 2025, from
https://drive.google.com/file/d/19KBIByK9sA3SOzUClROWyBbeZ3OiAKIb/vew
#4 For AP Erect.
Some considerations such as fluid levels on an erect image does not always indicate obstruction, as conditions such as severe gastroenteritis or jejunal diverticulosis may produce fluid levels as well.
The image acquired must include both the domes of the diaphragm to visualize any peritoneal gas (Free air).
6
#5 Mention common causes and symptoms here
Causes
• Small bowel obstruction (SBO):
o Adhesions (post-surgical) – most common
o Hernias
o Tumors
o Crohn’s disease strictures
o Intussusception
• Large bowel obstruction (LBO):
o Colorectal carcinoma – most common
o Volvulus (sigmoid or cecal)
o Diverticulitis with stricture
o Fecal impaction
Symptoms
• Abdominal pain
• Abdominal distension
• Vomiting
• Constipation
4
#6 We have not mentioned PA prone abdomen as it is a variation of the kub and is used when the patient is unable to stay supine or stand.
5
#7 For AP Erect.
Some considerations such as fluid levels on an erect image does not always indicate obstruction, as conditions such as severe gastroenteritis or jejunal diverticulosis may produce fluid levels as well.
The image acquired must include both the domes of the diaphragm to visualize any peritoneal gas (Free air).
6
#8 For Right and Left Posterior Obliques
After mentioning the abdomen region positioning mention this aswell
There is also another examination which is the examination performed at the lower costal margin, the patient is asked to raise the left side of the trunk of the body to about 20 and the Centering ray is placed at the lower costal margin slightly to the left side of the body which results in the vertebrae region.
7







![RADIOGRAPHIC_IMAGING_OF_THE_ABDOMEN[1].docx](https://cdn.slidesharecdn.com/ss_thumbnails/radiographicimagingoftheabdomen1-250705135117-4a4a689a-thumbnail.jpg?width=640&height=640&fit=bounds)












































