AY Isah -ANC
Scenario
Mrs. RA was a 14 year - old primigravida who came for Antenatal
booking at a GA 32 weeks with swollen lower legs. She had had a
genital mutilation when she was 10- year old. She wasn.t sure of her
fetal status but she admitted to be having low grade fever x 4/7 prior.
Exercise
a). List 5 identifiable risks in her
b). What relevant history are you likely to elicit from her?
c). List 8 possible remarkable examination findings that are likely to be
apparent
d). What additional investigations may be relevant in this case?
3.
AY Isah -ANC
Outline
• Introduction
• Objectives
• The Process / Procedure
• Demonstration
• Conclusion
4.
AY Isah -ANC
Outcome
• Components of ANC
• Different format
• Risk scoring
• Conduct the ANC
5.
AY Isah -ANC
Introduction
• Maternity care had existed for several decades - Intra-partum care
• Antenatal care - Last century
• Much later, reproductive health care providers - Postnatal period
(6weeks post-partum)
• Pre-conceptional care – About 50 years age!
• Maternity Care = Pre- conception + Antenatal + Intrapartum +
Postpartum
6.
AY Isah -ANC
Definition
• Specialized care for pregnant women which ensures that they attain
and maintain good health all through pregnancy, as well as improving
their chances of a safe delivery of a healthy infant
• It is a form of preventive medicine that involves a thorough initial
assessment to determine the level of risk to the mother and fetus and
a systematic program of follow up assessments all through pregnancy
• = Reduction of Maternal & Peri- Natal mortality/morbidity
7.
AY Isah -ANC
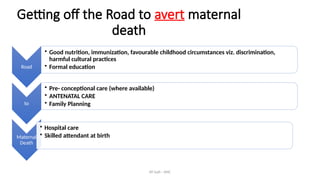
Getting off the Road to avert maternal
death
Road
• Good nutrition, immunization, favourable childhood circumstances viz. discrimination,
harmful cultural practices
• Formal education
to
• Pre- conceptional care (where available)
• ANTENATAL CARE
• Family Planning
Maternal
Death
• Hospital care
• Skilled attendant at birth
8.
AY Isah -ANC
Objectives of the Antenatal care
• Health promotion through a program of education, advice and support for the
woman and her family, including preparation for the process of child delivery
and child rearing
• Early detection and management of complications that may arise during the
course of pregnancy
• Prevention of factors that could compromise the health of the mother and the
baby
• Provides an opportunity for general health screening
9.
AY Isah -ANC
Models of ANC
Traditional:
• Every 4weeks until 28weeks gestation,
• Every 2 weeks until 36weeks gestation,
• Every week until delivery
• This model is excellent - early detection of complications which usually become
more likely as pregnancy advances towards term.
• However, may be quite tasking where there are inadequate numbers of health
care providers. The quality of care may often be compromised, as emphasis is
often on quantity(no. of visits) rather than quality of care received.
10.
AY Isah -ANC
Models- 2
Focused:
• With this model (championed by WHO) the pregnant woman is expected to
participate more actively in the care of herself and the fetus
• Emphasis should no longer be on the number of antenatal visits but rather
on the content and quality of care received at each visit
• Minimum of 4 antenatal visits recommended with this model and is aimed
at ensuring basic essential standards for women in developing countries
where trained personnel are in limited numbers
11.
AY Isah -ANC
Various levels of ANC
• Community based care (community Midwife/GP - led)
(Primary Health Care in Nigerian setting- Midwives/CHEWS)
• Hospital based (Consultant clinics)
• (Secondary/ Tertiary health care in Nigeria)
• ‘Shared’ Care through well established referral systems
• (Referral system exist but poorly developed)
12.
AY Isah -ANC
The conduct of ANC- Demonstration
• Booking Visit and,
• Follow – up visits
• History
• Examination
• Specific Investigations and,
• Health promotion
13.
AY Isah -ANC
Booking Visit
• This is the first antenatal visit.
• Purpose is to identify factors that could adversely affect pregnancy outcome
(Obstetric risk assessment) and address them
• Advocated < 14 weeks – Early
• Preconception clinic
Health education including contraceptive advice
Advise on nutrition and lifestyle issues (smoking, alcohol, hard drugs)
Risk assessment (e.g previous birth defect, previous obstetric complications)
Control of medical disorders e.g D.M before pregnan
14.
AY Isah -ANC
Advantages of Early Antenatal booking:
• Accurate determination of gestational age
• Documentation of important baseline information eg BP, BMI, Urinalysis etc
• Early detection and treatment of medical conditions
AY Isah -ANC
Risk Assessment of patients
• Patient is either,
• High risk or Low risk at the conclusion of booking procedure and care
given as appropriate
• Risk classification = Not static
• Events during pregnancy or delivery will necessitate a reclassification.
• Risk scoring for the above reason is indeed being downplay by some authorities
• Our stand?
17.
AY Isah -ANC
What constitutes high RISK pregnancy
Patients with any of these requires referral to higher medical center
• Bad obstetric history
• Nulliparity
• Grandmultiparity
• Teenage pregnancy
<16yrs
• Abnormal
lie/presentation
• Multiple pregnancy
• Previous preterm birth
• Short statue <1.5m
• Extreme social
deprivation
• SFH-date disparity
• Previous uterine scar
• Chronic medical disease
• Rh negative mother
• Previous APH/ PPH
• Previous gynaecological
operation
• Previous fetal
abnormality
• Previous
perinatal/neonatal birth
• History of infertility
18.
AY Isah -ANC
During follow up (Continuation of Visits)
• Chemoprophylaxis
• Tetanus prophylaxis
• Further visits
• Birth preparedness
• Health promotion
19.
AY Isah -ANC
Chemoprophylaxis in pregnancy
Malaria:
• In malaria endemic regions - Sulphadoxine-pyrimethamine administered
• At least 3 doses are given not less than 4 weeks apart, as directly observed therapy (DOT)
• Start at 1st
contact = > 14 weeks
• Until delivery
Anaemia:
• Anaemia in pregnancy - most often nutritional.
• Prophylaxis in the form of Iron and folic acid administered all through
pregnancy and for 2 months after
• Daily requirement = 60mg of elemental iron and, 0.4mg of folic acid required
daily
20.
AY Isah -ANC
Tetanus prophylaxis in pregnancy
• This is administered in a dose of 0.5mls IM as follows:
• First dose at first contact: -confers no protection
• Second dose after 4-6 weeks:- confers protection for 3 years
• Third dose 6 months later:- confers protection for 5 years
• Fourth dose 1 year after:- confers protection for 10years
• Fifth dose after another I year;- confers protection for life
• NEW APPROACH EXIST! = For those that want to risk Residency in OBGYN!!
21.
AY Isah -ANC
Further visits
Assess current state of her health (Ask, explain with empathy and, investigate)
• Check the following parameters:
i. Weight gain
ii. Blood pressure
iii. Urinalysis- protein, glucose, acetone
iv. Reconfirm GA on every visit (to be very sure)
v. Rate of fetal growth (Symphysio-fundal height assessment)
vi. Fetal lie, presentation, positioning, descent of presenting part, and fetal heart tones
• Required interventional measures for every abnormality detected
• Reassessment of the risk status at every visit
• Opportunity for Health education
• Formulation of the birth plan
22.
AY Isah -ANC
Health promotion / Counselling
Focuses on:
• Entire Antenatal visits and what the patient should expect
• Advise on importance of prophylaxis for malaria, anaemia tetanus
and PMTCT of HIV messages
• Nutrition and hygiene
• Need for the rest, exercise, sexual intercourse etc
• Discourage harmful traditional practices
• Newborn Care
23.
AY Isah -ANC
• Family planning messages
• Emphasis on safety during pregnancy viz. recognition of
complications and prompt presentation to hospital
• Birth preparedness and complication readiness*
24.
AY Isah -ANC
Birth preparedness & Complication readiness
• All pregnant women to have a written plan for birth and for dealing with
unexpected adverse events such as;
• Complications or emergencies, that may occur during pregnancy, childbirth or
immediate postnatal period
• Plan should be discussed and reviewed with a skilled birth attendant at least
one month to the expected delivery date
• WHO recommendation aimed to assist women, their partners and their
families to be adequately prepared for childbirth by making plans on how to
respond if complications or unexpected adverse event occurs
25.
AY Isah -ANC
“Booked patients” by WHO standard
Attendance of at least FOUR antenatal visits
Received Tetanus toxoid immunization
Received Intermittent prophylactic therapy for malaria
OR,
Minimum of two antenatal visits, if the last visit not more than two
weeks from the time of delivery
26.
AY Isah -ANC
Conclusion
• If they bother to attend, be professional and show them empathy
• At all visit, reconfirm the GA
• Search to identify any challenge and respond adequately or, Consult!
• Pregnancy is not a disease / curse – make it joyful