
Recommended
More Related Content
Similar to 603RADIOLOGIC TECHNOLOGY, JulyAugust 2017, Volume 88, Numb
Similar to 603RADIOLOGIC TECHNOLOGY, JulyAugust 2017, Volume 88, Numb (14)
More from MerrileeDelvalle969
More from MerrileeDelvalle969 (20)
Recently uploaded
Recently uploaded (20)
603RADIOLOGIC TECHNOLOGY, JulyAugust 2017, Volume 88, Numb
- 1. 603RADIOLOGIC TECHNOLOGY, July/August 2017, Volume 88, Number 6 CE Directed Reading This article is a Directed Reading. To earn continuing education credit for this article, see the instructions on Page 618. After completing this article, the reader should be able to: �� Define the concepts of leadership, followership, and servantship. �� Describe the importance of compassion, empathy, and altruism in patient care. �� Explain the ongoing need to evaluate one’s leadership and followership in the workplace. �� Discuss the varying leadership and service roles of the radiologic science professional. �� Explain how health care professionals’ servantship can enhance patient care. Steven M Penny, MA, R.T.(R), RDMS The primary role of all health care workers is that of patient servant. In health care, being a patient servant requires com-
- 2. passion for the patient, and many profes- sionals personally aspire to have empa- thy and altruism in all patient encoun- ters. As followers, health care workers might be free to choose which leader they desire to follow and a level of com- mitment they will provide to the leader and the organization. Lastly, health care workers, including medical imaging technologists, can be in leadership roles within an organization, and workers should study leadership concepts rou- tinely to prepare for these roles. Service and Leadership A given individual’s choice to enter a helping profession is the foundation for patient care. Studies have reported that nurses provided the following reasons for their career choice1: � Caring for people. � Rewarding work. � Possible career advancement. � Family history of working in health care. � Career security. � Socialization. � Job satisfaction. � Interest in the human body and medicine.
- 3. An Australian study of nearly 800 nurses and nursing students identified the top 5 reasons for entering the nurs- ing profession as it being an interesting job, an opportunity for caring for others, working with people, the per- ception that nursing was a calling, and a sense of giving to the community.1 Although health care workers choose to work in a field in which they take care of others for various reasons, providing honest patient care has been long estab- lished as a primary motivation. The health care culture typically stresses that medical professionals place the needs of their patients and soci- ety above all other considerations.2 Servantship, also called servanthood, relates to how health care practitioners serve the needs of patients and the Serving, Following, and Leading in Health Care Radiologic technologists often perform diverse roles throughout the workday, and they should have at least a minimal understanding of the responsibility and effects of these roles on the patient and organization. Although technologists can practice independently or as part of
- 4. a work group, individuals should be prepared to improve patient care and to function as a servant, follower, and leader for the overall success of the organization. This article examines those roles, emphasizing servantship. 604 RADIOLOGIC TECHNOLOGY, July/August 2017, Volume 88, Number 6 CE Directed Reading Serving, Following, and Leading in Health Care satisfaction refers to the pleasure and gratitude an indi- vidual feels when providing the best patient care one can offer.4 As a result, the compassionate caregiver feels a sense of personal benefit when generously contribut- ing to a positive change in patient care or outcomes.5 Compassion satisfaction benefits the patient as well and leads to gaining and sustaining patient trust when health care professionals exhibit excellence, altruism, skillfulness, and accountability.6 An ancient Native American teaching maintains that “each time you heal someone, you give away a piece of yourself until, at some point you will require heal- ing.”7 Working with individuals in pain and distress is a component of most caring professions, but continual exposure to the suffering of others has a cost: compas- sion fatigue. Compassion fatigue, often referred to as
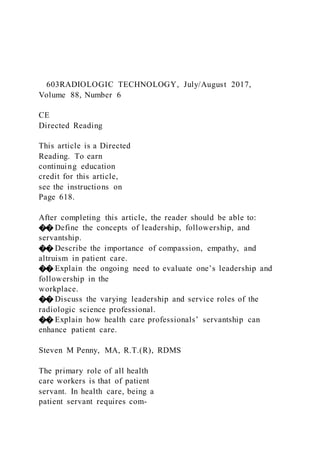
- 5. the cost of caring, is the combination of burnout and secondary traumatic stress.4,7 Burnout is a prolonged response to chronic job-related emotional and interper- sonal stressors characterized by emotional exhaustion, depersonalization, and a feeling of decreased personal accomplishment. Secondary traumatic stress relates to working with people whose illness or pain is uncontrol- lable, thus leading to a sense of powerlessness.4,8 Eventually, compassion fatigue can lead to disillu- sionment, which has been identified as a primary reason why nurses choose to leave health care.9 Unhappiness at work leads to increased turnover, absenteeism, safety risks, and poor judgment, all of which negatively community (see Box 1). Helping professions, such as those in patient care, offer a fitting environment for indi - viduals who are inclined to serve others. For the radiologic technologist, serving the needs of patients should not be viewed simply as a job requirement, but as the norm, and as a genuine opportunity to make a distinctive difference. Imaging technologists play a unique role in patient care. Whereas a nurse might spend an entire shift (often as many as 12 hours in critical care units) with a few patients, an imaging technologist might spend 10 min- utes or less performing a single diagnostic examination. However, limited time should not keep imaging profes- sionals from providing the patient with individualized care, and the time spent serving patients is amply rewarded. Servantship is based on acts of compassion, empathy, and altruism, with altruism being the ultimate goal (see Figure). Compassion, Empathy, and Altruism in Health Care The compassionate nature required of health care
- 6. professionals is associated with benefits and risks. Compassion is described as a virtue that causes an individual to consider seriously another person’s real - ity, inner self, emotions, and external circumstances.3 William J Bennett stated that courage allows a person to stand by others in challenging situations, but com- passion causes a person to stand with others who are in painful situations.3 Freely exhibiting compassion often results in what has been called compassion satisfaction. Compassion Box 1 Essentials of Servantship in Health Care Smile. Ensure patient dignity. Respond to patient needs appropriately. Value the uniqueness of the patient (eg, age, race, gender, emotional state). Advocate patient rights and safety. Never demonstrate disrespect towards the patient. Thank the patient. Serve the patient with compassion. Help others serve the patient. Identify patient mistreatment and demand improvement. Portray professionalism. Altruism (only for others) Empathy (connecting with others)
- 7. Compassion (considering others) Honesty Integrity Trust Increased follower engagement, sharing of knowledge and job performance. Figure. Patient care model where altruistic patient care is the ultimate goal. Image courtesy of the author. 605RADIOLOGIC TECHNOLOGY, July/August 2017, Volume 88, Number 6 CE Directed Reading Penny patients ultimately leads to the personal benefits of com- passion satisfaction, personal growth, self-actualization, and the potential to exhibit empathy.10 Unfortunately, studies have shown that empathy in the United States is on the decline. According to Anderson and Konrath, empathy in college students was 40% lower in 2011 compared with 20 or 30 years prior. This included a 48% drop in empathic concern, which is the tendency to possess concern for others’ emotions.11 The authors stated hypothetical societal
- 8. causes of decreased empathy such as: � An increase in reality television shows, which cen- ter on narcissistic main characters. � The rise of social media. � A focus of primary education on self-esteem vs encouraging the cultivation of empathy. According to the authors, this is why the millenial gen- eration has been referred to as “Generation Me.”11 Empathy is enhanced compassion. It can be defined as an ability to recognize and feel or share the emotions and feelings of others with a minimal distinction placed on the difference between self and others.8 Empathy often is confused with sympathy, which is concern for others.8 Although sympathy demonstrates care for another’s situation, empathy is characterized by sharing the perspective of feelings regarding the circumstances of another. Furthermore, empathy is the capacity to be affected by and share the emotional state of another person, while assessing the reasons behind the other person’s emotional state by identifying and adopting the person’s perspective.12 Most people have the capacity for empathy and the concept can be seen in nature and early in human life. In nature, mobbing demonstrates empathy. Mobbing is an instinctive antipredator behavior that occurs when a creature from an established colony warns the colony or attacks a predator to save others within the group. Infants as young as 12 months have shown the capacity to comfort victims of distress, while by age 18 months, they can display spontaneous helping behaviors.8 In patient care, empathy is a step above compassion
- 9. because empathy demands that caregivers put them- selves in the patient’s situation, and that they recognize that the caregiver could be in a similar state of ill health a patient faces. affect patient care.4 Physical manifestations of com- passion fatigue have been demonstrated and include gastrointestinal issues, headaches, physical exhaustion, insomnia, and substance abuse.7 Burnout has been shown to hinder patient care if the affected professional begins to treat patients in an uncaring manner.8 According to Aycock and Boyle, health care workers who are most at risk for compassion fatigue are those who bring high expectations to a job, are aged 30 years or younger, and are unmarried or lack an intimate part- ner.8 Slocum-Gori et al demonstrated that compassion satisfaction provides an effective counterbalance to the risks of compassion fatigue. A negative correlation has been established between compassion satisfaction and compassion fatigue and burnout.5 An individual can accomplish compassion satisfaction by acknowledg- ing the symptoms of compassion fatigue. Compassion fatigue can be overcome by focusing on others instead of oneself and through activities that help reinvigorate the passion for caring for others that once was felt.4 Stress management and relaxation techniques, exer- cise, rest, a healthy diet, forgiveness, and taking care of oneself all work to increase compassion satisfaction and battle compassion fatigue.7 An individual who regularly can balance the con- cern of self and others often is called a mature carer or mature caregiver.10 These individuals can maintain a healthy emotional balance, showing compassion toward others while maintaining a professional distance. The
- 10. self-awareness and self-confidence of mature caregivers strengthens their ability to care.10 By contrast, caregiv- ers distraught with compassion fatigue appear to create a protective yet invisible emotional barrier between the caregiver and the patient. As the caregiver begins to unintentionally build up a defensive emotional for- tification, compassion begins to erode. Establishing an emotional barrier between caregiver and patients can support self-preserving efforts. The analogy of building a barrier resembling a window vs a wall demonstrates how best to handle emotional barriers. A window provides the opening for compassionate care while simultaneously providing an emotional barrier to maintain a professional distance. The caregiver can continue to see the patient’s pain and point of view through the metaphorical window to provide compassionate care. Honest compassion for 606 RADIOLOGIC TECHNOLOGY, July/August 2017, Volume 88, Number 6 CE Directed Reading Serving, Following, and Leading in Health Care altruism in patient care focuses less on the monetary rewards, professional recognition, or even patient appre- ciation, but is purely for the sake of the other, or patient.10 Servantship Within the Code of Ethics Examples of servantship can be found in the Standards of Ethics established by the American Registry of Radiologic Technologists (ARRT). Within
- 11. the standards is a code of ethics, which the ARRT says can guide radiologic technology professionals in how they “evaluate their professional conduct as it relates to patients, healthcare consumers, employers, colleagues, and other members of the healthcare team.”15 The code of ethics is considered aspirational, or conduct that radiologic professionals should constantly strive to meet.15 Several key points within the code of ethics relate to servantship. The ARRT’s first ethical code states that profession- als should respond to patient needs and offer support for other team members.15 Responding to the needs of the patient requires a considerate approach from the health care professional and continual mindful- ness of the changing health needs of each patient. In this regard, imaging professionals must serve others by being completely available and accountable to patients. Accountability is the willingness to accept responsibil - ity for and the consequences of one’s actions.16 Dealing with the various and changing needs of each patient requires radiologic technologists to appreciate the dynamic environment in which they are engaged. Those interested in enhancing servantship should strive to augment existing knowledge in their fields of expertise beyond the minimal requirements imposed by certifica- tion organizations. Lifelong learning directly benefits the patient and the technologist. The support role of the imaging technologist encourages teamwork and all health professionals should share in the concern for the patient, working together for the patient’s benefit. The ARRT’s second ethical code articulates that the imaging technologist should strive “to provide services to humanity with full respect for the dignity of mankind.”15 Every individual has dignity, which can
- 12. be fragile and easily bruised.17 Wounding a patient’s dignity erodes trust, making serving the patient more difficult.17 As the technologist demonstrates respect At the core of patient care is the ancient maxim of treating others as one would like to be treated—often referred to as “the golden rule.” Yet health care profes- sionals can face decreased empathy, emotional burnout, and reduced altruistic motivation, resulting in less productive and effective patient care.12 Like compas- sion fatigue, a caregiving individual must recognize and address decreased empathy. Empathy is much like a muscle that can atrophy but regrow and regenerate if an individual chooses to focus on others instead of self.11 Focusing more on the needs of others typically results in an increase in personal and professional satisfaction.4 The empathy-altruism hypothesis claims that empathy directed toward improving another person’s welfare evokes altruistic behavior.12 Altruism, rooted in the French word autrui, meaning “other people,” is a human quality synonymous with self lessness, taking others’ perspectives, and showing concern for others for the sake of the other people rather than for oneself.10,13 The opposite of altruism is egoism. Egoism includes social reward-seeking behavior and punishment avoid- ance.12 Narcissism can be considered an extreme form of egoism. Narcissists have high emotional aptitude in that they can identify the emotions of others, but rather than aligning themselves with the other person’s emo- tions and feeling empathetic, narcissists use the other person’s emotions for personal gain or to manipulate.11 These self-serving individuals tend to prey upon the perceived weaknesses of others. According to some authors, an entire generation of
- 13. individuals once served the United States and the world in a manner that might never be matched. For example, in his book The Greatest Generation, Tom Brokaw describes the story of the servant-minded Chuck Van Gorder, MD. Gorder, who was a World War II field surgeon, returned to America after the war to continue offering his medical expertise in a small community. In the early days of his struggling medical practice, Gorder accepted garden vegetables or wild game as payment for the care he provided to the less fortunate patients in his community.7 Gorder stated that in the past, “medicine was more altruistic.”7 An altruistic individual is someone who is a servant intrinsically.14 True altruistic care is ideal in that the act is unconditional, spontaneous, and selfless.10 Possessing 607RADIOLOGIC TECHNOLOGY, July/August 2017, Volume 88, Number 6 CE Directed Reading Penny supports the leader while simultaneously meeting the mission of the organization and the professional direc- tives or standards of ethics placed upon the individual by the profession. The imaging technologist is an example of a frontline follower in health care. Followers perform the fundamental, yet vital, functions that involve commitment to the leadership of the organiza- tion, while simultaneously satisfying customer needs. As a result, everyone in the health care workplace could
- 14. be described as a follower, even the chief executive offi - cer, who typically reports to a board of directors. Some might perceive followers as those individuals within an organization who lack power, authority, or influence, but who are led from 1 task to another by a leader.19 Further, society’s view of leadership means that followership positions might be considered ancillary to accomplishing an organization’s overall mission.20 But a leader with a group of helpful, competent fol- lowers can accomplish a great deal, while a leader with a dysfunctional group of followers will struggle and likely fail. The most valuable followers are said to be skilled, self-directed individuals who invest time and energy in the work group and who use critical thinking effectively.4 The courageous follower model sugges ts that effective followers share and assume responsibility for a common purpose with their leaders, support the leader, constructively challenge the leader, participate in transformational needs required to fulfill the leader’s mission and organization, and take a moral stand when warranted (see Box 2).21 for a patient’s dignity, a reciprocated respect is created between the caregiver and patient, resulting in mutual trust and a commitment to the common aim of appro- priate diagnosis and recovery.10 Patients who have high trust in their caregivers tend to have better quality of care and outcomes.18 This person-oriented approach to professionalism compels a technologist to invest him- self or herself in patient interactions and to commit to doing the best possible job for the person in need.10 In the third and fifth codes, the ARRT states that the technologist should deliver “patient care and service unrestricted by the concerns of personal attributes or
- 15. the nature of the disease or illness, and without dis- crimination on the basis of sex, race, creed, religion, or socio-economic status.”15 Truthful servantship regards all patients as equals, regardless of whether the patient reciprocates the sentiment. Many patients have under- lying emotional needs that are not evident at the time of the first encounter. Although some patients exhibit rudeness or disrespect, technologists should always act “in the best interest of the patient,” particularly when the reasons for the patient’s behavior can be unknown or beyond health care professionals’ understanding.15 In the eighth ethical code, the technologist is encour- aged to practice “ethical conduct appropriate to the profession” and protect “the patient’s right to quality radiologic technology care.”15 The rules of ethics, which are mandatory standards of professional conduct, also are found in the ARRT’s Standards of Ethics. These rules help ensure the competence of the technologist as well as patient protection, safety, and comfort.15 Technologists who aspire to practice honest service follow these rules and ensure that others follow the rules as well. Followership Business literature is replete with research on leadership and models or suggestions for leaders. By comparison, followership research appears to be lack- ing. However, followership is a vital component of overall leadership effectiveness because leaders need followers in order to lead. Although many radiologic technologists serve as leaders at some point in their careers, the overwhelming majority of a radiologic technologist’s time is spent as a follower.4,19 In the clini - cal setting, followership relates to how the follower
- 16. Box 2 Courageous Follower Model21 The follower should have the courage to: � Support the leader and do everything possible to contribute to the leader’s success. � Assume responsibility for the common purpose and act independently. � Challenge constructively the leader or group’s behaviors or policies if these threaten the common purpose. � Participate in any transformation needed to improve the leader-follower relationship and the organization’s performance. � Take a moral stand when warranted to prevent ethical abuses or, at the very least, to refuse to participate in them. 608 RADIOLOGIC TECHNOLOGY, July/August 2017, Volume 88, Number 6 CE Directed Reading Serving, Following, and Leading in Health Care In almost every situation, followers outnumber lead- ers. Consequently, it is clear that a group of inharmonious followers can disrupt the productivity of an organization, ultimately negating the overall effectiveness of the leader
- 17. and the organization. Therefore, although followers do not have to be eternally happy, they need their leaders to provide a clear vision, perhaps with an explanation of collective goals. Failing to provide the connections and direction needed to maintain follower engagement could be the difference between effective and ineffective leader - ship. Thus, for the leader to be effective, the leader and follower must view their shared fundamental mission similarly. In effect, it is easier for a follower to develop a secure pattern of attachment to a leader when the leader and follower share a strong degree of synergy in values, goals, work, and communication styles.23 Followership requires a personal commitment to contribute within a collaborative environment.24 Being a team player with personal accountability is crucial for the follower to excel. Birds demonstrate teamwork in nature when they f ly in the “V” formation. The lead bird works the hardest, helping the entire group benefit from the aerodynamics of the formation. However, birds instinctively appreciate the need to cooperate and share the lead position in a group for the benefi t of all, so they rotate positions throughout their migratory f lights. Like birds, followers should occasionally rise to a casual leadership position when needed for the better - ment of the group. Serving as an efficient follower and a valued employee also is linked (see Box 3). Employers want to hire individuals who consistently28: � Demonstrate honesty and integrity. � Have positive attitudes. � Are reliable, professional, and intrinsically moti - vated. � Convey cheerfulness and friendliness in the work-
- 18. place. Choosing to be an efficient follower can improve leader- ship potential and place the follower in a position that might improve his or her opportunity to advance within the organization. Leadership The word leader originates from the word leden, which means to travel or to show the way.27 The idea of Examples of followership styles and types range from the follower offering the leader diminutive support and challenge just to maintain employment, to high support and challenge in which the follower serves more as a partner with the leader than an employee to accomplish shared goals and uphold the overarching mission of the organization (see Table 1).21 Followership types also relate to the view from the leadership position. According to Thomas, the most effective or valuable followers tend to be those who are talented critical thinkers.22 These individuals do not have to be told what to do and often practice informal leadership.22 Bureaucratic followers, commonly referred to as “brown nosers,” are conformists who follow the rules but lack leadership and critical thinking skills.22 Slackers are followers who do the minimum required or less than the minimum. Criticizers are followers who are disgruntled, pessimistic, and who work to manipulate the work envi- ronment negatively by using petty tactics of disruption. Leaders must thus appreciate the fact that if followership styles and types are perceptible, then followers should not be viewed simply by the leader as perfunctory subordi- nates, but rather as individuals with the freedom to choose which leader they want to help be successful.22 Equally, it
- 19. also is evident that followers can choose which leader to undermine. Both must share in the recognition and reme- diation of work troubles, as the dysfunction of a follower is not always the sole fault of the follower, but it could be a symptom of ineffectual leadership. Table 1 Followership Styles1 Style Explanation Resourceful Will do enough to retain position but no more. Individualistic Will speak up when others are silent, but voice is marginalized because it is too chronically contrarian. Implementer Will do whatever the leader wants them to do regardless of the consequences. They tend to not challenge the leaders authority. Partner Assumes full responsibility for their own actions and leader's behavior and acts accordingly. 609RADIOLOGIC TECHNOLOGY, July/August 2017, Volume 88, Number 6 CE Directed Reading Penny
- 20. leaders’ charge, or followers, in a desired manner to achieve specific goals. That is, leaders know what they need from followers, and effective leaders know how to get the desired results. This fundamental description of leadership acknowledges that leadership exists in all aspects of life—at home, work, and even in associations with strangers. If everyone has some leadership skills required and used in daily practice, then it stands to reason that everyone has some degree of leadership potential. However, on observation, it also is clear that some people are more likely to excel as leaders than are oth- ers.35 One must accept that although leadership can be learned, and that most people have evident or dormant skills that must be honed, leadership manifests more naturally in some individuals.36 Further, although some leadership skills are innate, most appear to be learned over the course of life experiences.18 Great acts of leadership exist throughout history. On April 15, 1912, as the Titanic began to sink and people fought for survival, 8 musicians played a solemn harmony as they stood on the deck of the plummeting leadership dates to Plato’s time (427 to 347 bc).26 Plato recognized 3 leadership concepts or laws in his early work The Republic; these are the rules of reason, desire, and spirit.29 Since Plato, many others have sought to define leadership and to consequently acknowledge the need to study leadership as a component of essential human existence. The term leader was noted as early as the 13th century, but the term leadership was not used until the 17th century.30 The organized study of leadership is essentially a novel endeavor, with the true
- 21. scientific research beginning early in the 20th century.30 Subsequently, much has been written about leader- ship and the construction of numerous definitions and theories, including the study of traits, qualities, and behaviors of effective leaders as they encourage others to participate, grow, and commit to an organization (see Table 2).30 Leadership has been characterized broadly as the ability to influence others to accomplish a specific goal.33 When one seeks to influence the thoughts, behaviors, or development of others, he or she is adopting the role of a leader.33 Leadership is a process that requires a group context and the aim to reach a defined goal.29 According to Fioravante, leadership consists of 2 fundamental functions: offering a clear vision and the ability to incentivize others to follow.34 Consequently, effective leaders influence those who are under the Box 3 Qualities of an Efficient Follower25 � Aligns personal goals with those of the organization and commits to achieving those shared goals. � Recognizes connections between own work and the broader mission of the organization. � Competent at completing a job. � Seeks opportunities to advance skills without being told to do so. � Can self-manage and self-assess. � Uses critical thinking effectively.
- 22. � Appreciates and respects the leader. � Is compliant, but unafraid to offer a different viewpoint from the leader respectfully, along with suggestions. � Interacts constructively with the leader and others in the workplace. � Leads by example. Table 2 Overview of Historical Leadership Theories2,3 Leadership Theory Time of Study Explanation Trait Early 20th century Sought to define effective leaders by analyzing shared personality traits or qualities. Behaviorist Late 1940s Concentrated on leader actions vs personal qualities. Contingency 1960s Refined version of situational leadership emphasizing that situation best predicts appro- priate leadership style.
- 23. Transactional 1980s to present Focuses on the contractual leader-follower relationship and the mutual benefits derived. Transformational 1980s to present Focuses on follower change and personal growth and development. 610 RADIOLOGIC TECHNOLOGY, July/August 2017, Volume 88, Number 6 CE Directed Reading Serving, Following, and Leading in Health Care Truly great leaders develop their skills over a life- time.40 The consequence of a manager taking on a true leadership role represents a focus shift. Whereas the manager’s primary obligation is to produce accept- able end results for overall organizational success, the manager-leader also must concentrate on creating personal connections to engage followers.27 Essentially, management is solely about building business, and lead- ership is about building business and relationships. If a manager desires to be a leader, then the manager should
- 24. strive to include relationship building as part of the management skill set because it is clear that people are the most significant resource in an organization.41 Demonstrating Leadership Through study of leadership skills of renowned individuals, scholars have developed an extensive list of characteristics to describe the qualities of great lead- ers. These qualities also are called leadership traits. In many situations, these traits also are called virtues. Trait theories of leadership arose as a way to identify specific characteristics of a successful leader; although the list is expansive, several are common throughout the litera- ture. These trait theory skills include33: � Technical skills. � Friendliness. � Task motivation. � Social skills. � Emotional control. � General charisma. � Intelligence. Other common leadership skills identified include creativity, diplomacy, verbal f luency, knowledge, orga- nization, persuasiveness, and the ability to understand abstract concepts.31 The virtues of honesty and integrity should be evident in leaders. Honesty is truthfulness, being free of fraud or deception. Thus, honesty is a virtue that can be honed to become an essential part of an individual’s character. The most successful leaders are honest and are accountable for their own actions.42 Honesty is accomplished through a conscious effort to live in truth. Honesty breeds integrity,
- 25. and integrity develops credibility.42 Ultimately, integrity is honesty demonstrated, as integrity is open-mindedness in thought, word, and deed.43 For the leader, honesty and ship. The musicians’ calm offering in a time of human tragedy demonstrated noble leadership. Unfortunately, all 8 musicians died in the frigid waters of the North Atlantic Ocean.37 On September 11, 2001, in the midst of the hijacking of United Airlines Flight 93, passenger Todd Beamer declared “let’s roll!,” which portrayed leadership in the midst of a horrifying situation. That day, the hijacked plane was headed toward any number of susceptible targets in the nation’s capital, but it is believed that Beamer and others onboard overtook the hijackers. Although the plane crashed in a field, the pas- sengers prevented the loss of additional human lives had the original target been hit.38 These historical examples demonstrate extraordi- nary leadership in practice, but routine leadership also is evident in everyday lives. For example, parents influ- ence their children, and therefore are leaders. At work, a health care professional can be a leader among a group of coworkers.39 Still, when asked for an example of a leader within an organization, many people often look to those who have significant power within the chain of command.40 True leadership has nothing to do with one’s occu- pation or level within an organization.40 Anyone can display leadership skills at anytime. Thus, leader- ship can be formal or informal. Formal leadership is exhibited by an individual in an assigned role who has allocated powers within an organization, but informal leadership can be demonstrated by members of a work group, such as a collection of staff technologists, who
- 26. share a leadership role to accomplish routine tasks.4 Often, definitions of management and leadership overlap, yet there is a clear distinction between leader- ship and management. Management has been described as preparing, arranging, staffing, and controlling actions of followers to achieve specific goals.4 Managers often focus on outcomes, make the best possible deci- sions for a group, and concentrate on the bottom line. However, managers are placed at optimal power levels within organizations to exercise leadership simply because managers oversee, and therefore lead subordi - nates in day-to-day organizational tasks and efforts.27 Holding a manager title does not necessarily make someone a leader. However, managers can study and cultivate their individual leadership styles. 611RADIOLOGIC TECHNOLOGY, July/August 2017, Volume 88, Number 6 CE Directed Reading Penny research a revolutionary concept referred to as emotion- al intelligence (EI). Although EI has been defined and then redefined by others, the 5 domains of emotional intelligence are54: � Knowing one’s emotions. � Managing one’s emotions. � Motivating oneself by organizing emotions. � Recognizing the emotions of others.
- 27. � Managing the emotions of others. EI and leadership have been linked throughout the literature, and authors often establish direct relation- ships between leadership effectiveness and EI.50 A statistically significant correlation between EI and the leader’s job performance has been reported.50 Researchers consistently report that the leader who has higher EI often is more effective.53 Batool stated that EI can help reduce stress, develop performance, improve sense of achievement, and enhance the productivity of the employee by meeting organizational goals.54 Some authors claim that EI is a better predictor of a leader’s success than is intellectual quotient (IQ ).55 Four components make up EI: self-awareness, self-management, social awareness, and relationship management (see Table 3).51 A leader who is self-aware can recognize his or her strengths, weaknesses, and feel - ings. Being self-aware requires humility. Management author Jim Collins described leader levels, with level 5 as the highest level of leadership. These high-level leaders combine humility and will.56 Thus, it may be surmised that level 5 leaders possess a higher EI because they have the ability to appreciate the impor- tant contributions of followers and to look in the mirror to apportion responsibility. Being humble enough to manage ego and power is a mark of an emotionally strong leader. Effective leaders are willing to make well- informed decisions to the best of their ability and are bold enough to stand by those decisions. Leaders also should be willing to admit when they make mistakes, a task that requires the courage to reflect upon one’s actions. Emotionally intelligent leaders also can manage
- 28. relationships with followers and self-manage their own emotions to breed an environment of trust.50 Finally, emotionally intelligent leaders have social aware- ness, which demonstrates the capacity to empathize integrity are demonstrated in straightforwardness in all interactions with followers, which in turn yields respect and trust from followers.44 Trust is vital for the leader, and leaders who make personal connections by establishing trust with fol- lowers tend to be more effective.41 If a follower trusts a leader, then trust in the organization also can increase, and trust in an organization has been shown to be positively associated with work engagement, sharing of knowledge, teamwork, and employee performanc e.45 Effective leaders are true to themselves and their follow - ers.46 John Wooden, famed University of California, Los Angeles, basketball coach, claimed that before one can lead others, one must be able to lead oneself.46 Because health care professionals are responsible for the lives of others, honest personal reflection and accountability always should thrive in patient care, even in leadership positions. Blanchard and Miller suggested that the lead- er continuously gain knowledge, reach out to others, open their worlds, and walk toward wisdom (GROW).47 In clinical practice, the application of the as low as reasonably achievable (ALARA) concept, as it relates to diagnostic imaging of any kind, is an example of honesty and integrity a leader can promote consistently. The Image Gently Alliance, which was founded by the American Society of Radiologic Technologists, Society for Pediatric Radiology, American College of Radiology and the American Association of Physicists in Medicine, operates on similar principles. Image
- 29. Gently aims to advocate on behalf of and ensure safe and effective imaging care for children worldwide.48 Parents usually are unaware of the radiation exposure their child receives and the potential for biological effects from diagnostic examinations. Leaders who have the courage to demonstrate honesty and integrity in imaging practice know and enforce ALARA principles and practice standards, are patient advocates, and gain patient trust, ultimately supporting enhanced patient care. The courage to demonstrate honesty and integrity in leadership is not so much fearless as it is a willingness to act out of conviction.49 Emotional Intelligence and Leadership In the mid-1990s, psychologist and writer Daniel Goleman helped bring to the forefront of leadership 612 RADIOLOGIC TECHNOLOGY, July/August 2017, Volume 88, Number 6 CE Directed Reading Serving, Following, and Leading in Health Care the changing definition of EI appears to cause some confusion and difficulty among academic scholars, and others denounce the existence of EI altogether.50 Still, emotions likely play a vital role in leadership success; leaders who are self-aware, manage themselves, and can relate to others appear to create a work environment favorable for success.52,54
- 30. Leadership Models George Washington, Martin Luther King Jr, and Mahatma Gandhi are considered impressive, efficient leaders. Although these individuals did not know each of their followers personally, followers were said to feel a personal connection with the leaders because each demonstrated an evident concern for followers.57-59 Great historic leaders in health care also have made distinctive contributions to evoke change. Examples include Clara Barton, the founder of the American Red Cross; Wilhelm Conrad Roentgen, the engineer and physicist who discovered x-rays; and Alexander Fleming, the Scottish scientist who discovered penicillin.60-62 Leadership in health care is facing some challenges.18 Reasons suggested for these challenges include the lack of a formal leadership model specifically for health care, time constraints on those in leadership positions in the health care setting that are secondary to time needed for clinical responsibilities, and the financial limitations of an ever-evolving health care system.18 As a result, sev- eral leadership styles have been proposed. Transactional leadership, transformational leadership, and servantship are fundamental forms of leadership that are practi- cal for use in a health care organization, although the emphasis on the leader-follower relationship varies markedly among them. Transactional Leadership Transactional refers to accordance or a contract between people, or a group of people, that results in an exchange.42 In business, transactional leadership is an approach in which the leader-follower relationship is
- 31. focused on the mutual benefits when an effort-reward contract is in place.31 For example, if one follower were to outperform another follower on a specific task, the transactional leader would recognize the higher achiev- er through recognition, remuneration, or some other with others. The common characteristic among these concepts appears to be reflection upon self without neglecting others. Leaders with high EI might practice situational leadership, which emphasizes that a leader must adapt his or her style according to the situation of the leader’s team or organization.44 EI has been demonstrated as important for follow - ers as well. A follower’s EI contributes to the leader’s assessment of the follower’s potential and credibility.51 Essentially, an emotionally intelligent follower respects the power of the leader and can delineate his or her unique role within the organization. Complex EI inventories, scales, questionnaires, and online tools have been created to measure EI.50 However, since its introduction, the concept of EI has been criticized. Although the control and malle- ability of emotions clearly is necessary for leadership, a definitive model for measuring EI has not yet been established, resulting in possible ambiguity.50 Some authors also suggest that participants can falsely self- report, leading to skewed data. Finally, critics say that Table 3 Dimensions of Emotional Iintelligence4,5 Dimension Capacity to Explanation
- 32. Self-awareness Appreciate one’s individual emotions, strengths, and weaknesses Sought to define effective leaders by analyzing shared personality traits or qualities. Relationship management Influence, handle disagreement, and inspire change Concentrated on leader actions vs personal qualities. Social awareness Relate to and empathize with others Refined version of situational leader- ship emphasizing that situation best predicts appropriate leadership style. Self- management
- 33. Be truthful and control emotions that can be harmful to relationships Focuses on the contractual leader- follower relationship and the mutual benefits derived. 613RADIOLOGIC TECHNOLOGY, July/August 2017, Volume 88, Number 6 CE Directed Reading Penny Transformational Leadership Whereas the transactional leader motivates via an exchange relationship with the follower, the transfor- mational leader clearly communicates his or her vision and inspires followers by promoting self-respect, pride, and mutual trust.58 For example, in his celebrated “I Have a Dream” speech, Martin Luther King Jr provided an example of transformational leadership through symbolic oratory by identifying and articulating a clear vision, providing a model for change, establishing lofty expectations, and fostering acceptance.58
- 34. Transformational leadership strongly predicts job satisfaction, ratings of effectiveness, high group performance, and increased overall work effort by fol- lowers when compared with transactional leadership.54 Clarence Francis, once the chief executive officer of General Foods, stated that “You can buy a person’s time; you can buy his physical presence at a given place, but you cannot buy enthusiasm. You cannot buy loyalty. You cannot buy the devotion of hearts, minds, and souls. These you must earn.”65 This statement relates to the transformational leader, because follow - ers of transformational leaders often view the leader as a benevolent parent who remains responsive and treats the follower as an equal despite the disparity in knowl - edge and experience.30 Transformational leaders ultimately acquire trust, fondness, admiration, loyalty, and respect from fol- lowers.30 Transformational leadership is thus rooted in emotion and has been linked with the leader’s EI level.51 Transformational leaders with high EI use empathy to connect with followers and work to encourage expres- sion of emotions from individuals or group members.49 Having empathy for followers is thus a precursor for the transformational leadership model because the leader’s ability to express emotions is vital for the success of the group.49 Several benefits to transformational leadership have been reported. Transformational leaders recognize the need for the follower to learn and evolve continually. Govaerts et al studied 972 employees and revealed that empowering employees to do more and learn about their strengths encourages the employees to stay with the organization.66 Authentic leadership is similar to transformational leadership, but at a more personal level
- 35. established incentive. Conversely, a punishment would follow the breaking of an established rule or agreed- upon custom. Although financial or social rewards have been reported to increase feelings of fairness and satis- faction, punishment exerts a negative influence on the follower.61 Transactional leadership has been cited as the most common leadership model used in health care.18 However, studies suggest f laws in transactional leader- ship. One study claimed that out of 845 employees, only 9% agreed their performance was motivated by transaction.30 And although transactional leadership often helps leaders accomplish specific goals, it also can stif le creativity and innovation by discouraging individuality and expecting compliance.44 Disparity between the effort and resulting reward for similar contributions (or punishment for infractions) can create ambiguity among followers. For example, if 1 employee’s frequent tardiness and laziness remains unpunished, but an employee who is continually punctual and hardworking is not recognized, the lat- ter employee could become unhappy and lose respect for the leader. The punctual, hardworking employee might even feel mistreated or taken advantage of for simply doing what is expected. Employees often experience burnout when not recognized and offered rewards or even gratitude.64 Transactional leadership is an impersonal form of leadership because there is no attempt to change or recognize the follower’s attitudes or values, resulting in a follower who experiences a great deal of anxi- ety and uncertainty about his or her employment.32 Transactional leadership is related to directive leader-
- 36. ship, also called autocratic, controlling, or authoritarian leadership.36 An autocratic leader assumes complete sov- ereignty and control of the group. Autocratic leaders do not recognize the benefit of cultivating an intrinsically motivated employee, but rather focus on extrinsically motivating each employee equally to accomplish spe- cific goals for the leader or organization.18 Transactional leaders also fail to build trust between the leader and fol - lower.18 Although a transactional leader might be viewed as successful by his or her superiors, especially for pro- ducing results, followers can feel subjugated and isolated as they submit to the changing needs of the leader. 614 RADIOLOGIC TECHNOLOGY, July/August 2017, Volume 88, Number 6 CE Directed Reading Serving, Following, and Leading in Health Care and professional goals (see Table 4).67 Models of leader - ship in which the leader’s behaviors more significantly and positively influence a follower’s self-identity appear to produce a positive effect on follower behaviors and the overall success of the organization.67,69 Servant lead- ership is a value-laden leadership model that encourages the ethical treatment of followers, thus gaining follower trust and increasing overall effectiveness of the group.67 Transformational leadership contrasts with servant leadership because transformational leaders focus on the well-being of the organization, but servant leaders, though mandated to serve the organization, focus on the best interests of their followers first.69
- 37. The servant leadership model appears to be ideal in the health care setting because health care workers typically emphasize serving patients.18 Thus, those who accept a leadership role in a caregiving setting should be, at their core, naturally predisposed to offering com- passionate guidance.69 Conclusion Patients rightly anticipate and merit the best possible health care. Serving the needs of others with compas- sion is the primary obligation of professionals who work in health care. Some health care professionals might be required to perform the functions of servant, follower, that is based on the concept of being genuine. Authentic leaders inspire others and motivate followers on an intellectual level while simultaneously providing them with individualized attention.45 Servant Leadership Although many leadership theories focus on the top-down approach to leadership, in which the source of power is placed solely on the leader, the servant lead- ership model establishes a bottom-up organizational view in which the followers’ needs are regarded before the leader’s desires.67 Thus, servant leadership focuses on the welfare of the follower rather than the glorifica- tion of the leader. This model establishes a servant-first, leader-second attitude.30 Robert K Greenleaf often is credited with first recognizing and espousing the value of the self less leader (see Box 4).37 However, this form of leadership has been demonstrated throughout his- tory. The Bible says that Jesus espoused the concept of
- 38. servant leadership when he said, “whoever wants to be great among you must be your servant, and whoever wants to be first must be your slave—just as the Son of Man did not come to be served, but to serve.”68 George Washington often closed his letters by signing “your humble obedient Servant.”57 Despite the fact that these historical figures were in a position that offered them great power over their followers, they chose to humble themselves to promote the welfare of others first. With servant leadership, the leader functions as a steward, recognizing followers as individuals who should be nurtured to achieve their highest personal Box 4 Characteristics of Servant Leaders18 � Listening skills � Empathy � Healing focus � Awareness � Persuasive ability � Conceptualization skills � Foresight � Possesses stewardship ethics � Commitment to follower growth � Community-building skills Table 4 Key Ways Leaders Can Serve6 Action Purpose See the future. Servant leaders should provide followers a
- 39. vision for the future. Engage and develop others. Servant leaders put the right people in the right positions and cultivate followers’ potential. Reinvent continually. Servant leaders should never stop learning and always encourage follower education. Value results and relationships. Servant leaders obtain financial strength and profits from enhanced relationships with customers and employees. Embody values. Servant leaders continually build trust between customers and followers while embodying the values of the organization. 615RADIOLOGIC TECHNOLOGY, July/August 2017, Volume 88, Number 6 CE Directed Reading Penny
- 40. 8. Brennan MD, Monson V. Professionalism: good for patients and health care organizations. Mayo Clin Proc. 2014;89(5):644-652. doi:10.1016/j.mayocp.2014.01.011. 9. Bennett WJ. The Book of Virtues. New York City, NY: Simon and Schuster; 1993. 10. Kelly L, Runge J, Spencer C. Predictors of compassion fatigue and compassion satisfaction in acute care nurses. J Nurs Scholarsh. 2015;47(6):522-528. doi:10.1111/jnu.12162. 11. Slocum-Gori S, Hemsworth D, Chan WWY, Carson A, Kazanjian A. Understanding compassion satisfaction, compassion fatigue and burnout: a survey of the hospice palliative care workforce. Palliat Med. 2013;27(2):172-178. doi:10.1177/0269216311431311. 12. Decker JT, Brown JLC, Ong J, Stiney-Ziskind C. Mindful- ness, compassion fatigue, and compassion satisfaction among social work interns. Soc Work Christ. 2015;42(1):28-42. 13. Aycock N, Boyle D. Interventions to manage compas- sion fatigue in oncology nursing. Clin J Oncol Nurs. 2009;13(2):183-191. doi:10.1188/09.CJON.183-191. 14. Hem MH, Halvorsen K, Nortvedt P. Altruism and mature care: some rival moral considerations in care ethics. Nurs Ethics. 2014;21(7):794-802 doi:10.1177/0969733014521094. 15. Anderson P, Konrath S. ‘Why should we care?’—what to do about declining student empathy. Chronicle of Higher Education website. http://www.chronicle.com/article/Why -Should-We-Care-What/128420. Accessed May 3, 2017. 16. Decety J. The neurodevelopment of empathy in humans.
- 41. Dev Neurosci. 2010;32(4):257-267. doi:10.1159/000317771. 17. Burks DJ, Youll LK, Durtschi JP. The empathy-altruism association and its relevance to health care professions. Soc Behav Personal. 2012;40(3):395-400. doi:10.2224/sbp.2012 .40.3.395. 18. Oord TJ, ed. The Altruism Reader: Selections From Writings on Love, Religion, and Science. West Conshohoken, PA: Templeton Foundation Press; 2008. 19. Brokaw T. The Greatest Generation. New York City, NY: Dell Publishing; 1998. 20. Christenson JE. Servanthood in the 21st century. Phi Kappa Phi Forum. 2008;88(2):32-33. 21. American Registry of Radiologic Technologists. ARRT Standard of Ethics. https://www.arrt.org/pdfs/Governing -Documents/Standards-of-Ethics.pdf. Accessed July 7, 2016. 22. Makely S. Professionalism in Health Care: A Primer for Career Success. 4th ed. Upper Saddle River, NJ: Pearson Education; 2013. 23. Elmer D. Cross-Cultural Servanthood: Serving the World in Christlike Humility. Westmont, IL: IVPBooks; 2006. 24. Trastek VF, Hamilton NW, Niles EE. Leadership models in health care - a case for servant leadership. Mayo Clin Proc. 2014;89(3):374-381. doi:10.1016/j.mayocp.2013.10.012. and leader simultaneously, or shift between roles to
- 42. meet the needs of employers, employees, and custom- ers. Striving daily to satisfy these needs requires that the health care professional be honest and demonstrate integrity when interacting with others. Ultimately, it is professionally warranted that health care workers continually research and gain knowledge about the con- cepts of service, followership, and leadership to adapt to an ever-changing health care environment, especially to provide the best possible individualized patient care. Steven M Penny, MA, R.T.(R), RDMS, is the author of several textbooks and articles related to medical imaging, education, and patient care. His imaging specialties include radiography and abdominal, pediatric, and obstetrical/ gynecological sonography. He is the lead instructor for the medical sonography program at Johnston Community College in Smithfield, North Carolina. Reprint requests may be mailed to the American Society of Radiologic Technologists, Publications Department, 15000 Central Ave NE, Albuquerque, NM 87123-3909, or emailed to [email protected] © 2017 American Society of Radiologic Technologists References 1. Riggio RE, Chaleff I, Lipman-Blumen J, eds. The Art of Followership: How Great Followers Create Great Leaders and Organizations. Hoboken, NJ: Jossey-Bass; 2008. 2. Gosling J, Sutherland I, Jones S. Key Concepts in Leadership. London, UK: Sage; 2012. 3. Aronson E. Integrating leadership styles and ethi- cal perspectives. Can J Adm Sci. 2001;18(4):244-256.
- 43. doi:10.1111/j.1936-4490.2001.tb00260.x. 4. Foster C, Roche F. Integrating trait and ability EI in pre- dicting transformational leadership. Leadersh Organ Dev J. 2014;35(4):316-334. doi:10.1108/LODJ-07-2012-0087. 5. Goleman D. Emotional Intelligence: Why It Can Matter More Than IQ. 10th ed. New York City, NY: Bantam Books; 2006. 6. Blanchard K, Miller M. The presentation. In: Great Leaders Grow: Becoming a Leader for Life. San Francisco, CA: Berrett- Koehler Publishers Inc; 2012:108. 7. Eley R, Eley D, Rogers-Clark C. Reasons for entering and leaving nursing: an Australian regional study. Aust J Adv Nurs. 2010;28(1):6-13. http://www.ajan.com.au/Vol28 /28-1_Eley.pdf. Accessed May 3, 2017. 616 RADIOLOGIC TECHNOLOGY, July/August 2017, Volume 88, Number 6 CE Directed Reading Serving, Following, and Leading in Health Care 44. Arnold F. Nurture and develop people. In: What Makes Great Leaders Great: Management Lessons From Icons Who Changed the World. New York City, NY: McGraw Hill; 2012:154. 45. Murayama KM. Pyramids and roundtables: a reflection on leadership. Am J Surg. 2014;208(6):873-880. doi:10.1016/j .amjsurg.2014.09.008.
- 44. 46. Naagarazan, R.S. Textbook on Professional Ethics and Human Values. Daryaganj, India: New Age International; 2006. 47. DuBois M, Hanlon J, Koch J, Nyatuga B, Kerr N. Leadership styles of effective project managers: Techniques and traits to lead high performance teams. J Econ Dev Manage IT Finance Market. 2015;7(1):30-46. 48. Stander FW, de Beer LT, Stander MW. Authentic leadership as a source of optimism, trust in the organisation and work engagement in the public health care sector. SA J Hum Resour Manag. 2015;13(1):1-12. doi:10.4102/sajhrm.v13i1.675. 49. Wooden J, Jamison S. Wooden on Leadership. New York City, NY: McGraw Hill; 2005. 50. Campaign overview. Image Gently website. http://image gently.org. Accessed July 7, 2016. 51. Mattone J. Intelligent Leadership: What You Need to Know to Unlock Your Full Potential. Saranac Lake, NY: AMACOM Books; 2013. 52. McCleskey J. Emotional intelligence and leadership. Int J Organ Anal. 2014;22(1):76-93. doi:10.1108/IJOA-03-2012 -0568. 53. Mathew M, Gupta KS. Transformational leadership: emo- tional intelligence. SCMS J Indian Manage. 2015;12(2):75-89. 54. Batool BF. Emotional intelligence and effective leadership.
- 45. J Business Stud Q. 2013;4(3):84-94. 55. Sadri G. PhD. Emotional intelligence and leadership development. Public Pers Manage. 2012;41(3):535-548. doi:10.1177/009102601204100308. 56. Collins J. Level 5 leadership. In: Good To Great: Why Some Companies Make the Leap…and Others Don’t. New York City, NY: Harper Collins; 2001:17-40. 57. Brookhiser R. George Washington on Leadership. New York City, NY: Basic Books; 2008. 58. Godwin JL, Houghton JD, Neck CP, Mohan EC. Dr. Martin Luther King, Jr.’s “I have a dream” speech as a tool for teach- ing transformational leadership and vision. J Organ Behav Educ. 2011;4:23-41. 59. Kuofie M, Stephens-Craig D, Dool R. An overview perception of introverted leaders. Int J Global Business. 2015;8(1):93-103. 60. Knebel AR, Toomey L, Libby M. Nursing leadership in disaster preparedness and response. Annu Rev Nurs Res. 2012;30(1):21-45. doi:10.1891/0739-6686.30.21. 25. Foley TJ. Followership and student leadership: exploring the relationship. J Leadersh Account Ethics. 2015;12(4):11-23. 26. Alvesson M, Blom M. Less followership, less leadership? An inquiry into the basic but seemingly forgotten downsides of leadership. [email protected]@gement. 2015;18(3):266-282.
- 46. 27. Thomas SARTMA. Followership: leadership’s partner. Can J Med Lab Sci. 2012;74(4):8-10. 28. Lapierre L, Carsten MK. Followership: What Is It and Why Do People Follow? Bradford, UK: Emerald Group Publishing Limited; 2014. 29. Whitlock J. The value of active followership. Nurs Manage. 2013;20(2):20-3. 30. Currie JP. Complementing traditional leadership: the value of followership. Ref User Serv Q. 2014;54(2):15-18. doi:10.5860/rusq.54n2.15. 31. Chester E. Reviving Work Ethic: A Leader’s Guide to Ending Entitlements and Restoring Pride in the Emerging Workplace. Austin, TX: Greenleaf Book Group Press; 2012. 32. Ukey KL. The hues of leadership: a glance at the conven- tional and disruptive style and some general traits of busi - ness leaders. Int J Entrepreneurship Business Environ Perspect. 2013;2(3):480-489. 33. Takala T. Plato on leadership. J Bus Ethics. 1998;17(7):785- 798. doi:10.1023/A:1005789531144. 34. Ronald B. Comprehensive leadership review - literature, theories and research. Adv Manage. 2014;7(5):52-66. 35. Badshah S. Historical study of leadership theories. J Strateg Hum Resour Manag. 2012;1(1):49-59. 36. Blanchard K, Hodges P. Lead Like Jesus. Nashville, TN: Thomas Nelson Inc; 2005.
- 47. 37. Fioravante PL. An effective leadership revelation - blend- ing dark side and positivist traits. J Appl Bus Econ. 2013;15(1):107-125. 38. Giltinane CL. Leadership styles and theories. Nurs Stand. 2013;27(41):35-9. 39. Whitehead DK, Weiss SA, Tappen RM. Essentials of Nursing Leadership and Management. 5th ed. Philadelphia, PA: FA Davis Company; 2010. 40. Levinson MH. A general semantics analysis of the RMS Titanic disaster. et Cetera. 2012;69(2):143-156. 41. Atkins SE. The 9/11 Encyclopedia. Westport, CT: Praeger Security International; 2008. 42. Greenleaf RK. On Becoming a Servant Leader: The Private Writings of Robert K. Greenleaf. San Francisco, CA: John Wiley & Son Inc; 1996. 43. Blanchard K, Miller M. The secret. In: The Secret: What Great Leaders Know and Do. San Francisco, CA; Berrett- Koehler Publishers Inc; 2014:24-29. 617RADIOLOGIC TECHNOLOGY, July/August 2017, Volume 88, Number 6 CE Directed Reading Penny
- 48. 61. James I. Remarkable Physicists: From Galileo to Yukawa. West Nyack, UK: Cambridge University Press; 2004:178. 62. Bleich MR. Leadership and brilliant mistakes. J Contin Educ Nurs. 2015;46(5):203-204. doi:10.3928/00220124-2015 0420-13. 63. Tremblay M, Vandenberghe C, Doucet O. Relationships between leader-contingent and non-contingent reward and punishment behaviors and subordinates’ perceptions of jus- tice and satisfaction, and evaluation of the moderating influ- ence of trust propensity, pay level, and role ambiguity. J Bus Psychol. 2013;28:233-249. doi:10.1007/s10869-012-9275-4. 64. Basińska BA, Wilczek-Rużyczka E. The role of rewards and demands in burnout among surgical nurses. Int J Occup Med Environ Health. 2013;26(4):593-604. doi:10.2478/s13382 -013-0129-8. 65. Baldoni J. Make your presence felt. In: Lead By Example: 50 Ways Great Leaders Inspire Results. New York City, NY: Amacom books; 2009:33. 66. Govaerts N, Kyndt E, Dochy F, Baert H. Influence of learning and working climate on the retention of tal- ented employees. J Workplace Learn. 2011;23:35-55. doi:10.1108/13665621111097245. 67. Ljungholm DP. Effective servant leadership behavior in organizations. Linguist Philosophical Invest. 2016;15:239. 68. The bible. ESV. Matthew 20: 27-28. 69. Winston B, Fields D. Seeking and measuring the essential behaviors of servant leadership. Leadersh Organ Dev J.
- 49. 2015;36(4):413-434. doi:10.1108/LODJ-10-2013-0135. 618 RADIOLOGIC TECHNOLOGY, July/August 2017, Volume 88, Number 6 Directed Reading Quiz continued on next page Read the preceding Directed Reading and choose the answer that is most correct based on the article. QUIZ ID: 17804-01 1.5 Category A credits 2.5 MDCB credits Expires August 31, 2020* Serving, Following, and Leading in Health Care To earn continuing education credit: � Take this Directed Reading quiz online at asrt.org/drquiz. Enter the Quiz ID 17804-01 into the search bar. � Or, transfer your responses to the answer sheet following the quiz and mail it in for grading. * Your answer sheet for this Directed Reading must be received in the ASRT office on or before this date. 4. The ability to recognize the emotions and feelings of others with a minimum distinction placed upon the difference between self and others is known as: a. advocacy.
- 50. b. self-sacrifice. c. attentiveness. d. empathy. 5. Health care professionals who face decreased empathy and reduced altruistic motivation have: a. additional focus and drive. b. a decreased likelihood of burnout. c. less productive and effective patient care. d. better patient engagement. 1. Which of the following is not an element upon which servantship is based? a. sympathy b. empathy c. compassion d. altruism 2. Compassion fatigue is the result of the combination of ______ and ______ . a. secondary traumatic stress; empathy b. burnout; secondary traumatic stress c. burnout; self-sacrifice d. self-sacrifice; empathy 3. Someone who regularly can balance the concern of self and others is considered a: a. mature caregiver. b. self-preserver. c. follower. d. potential caregiver. 619RADIOLOGIC TECHNOLOGY, July/August 2017, Volume 88, Number 6
- 51. Directed Reading Quiz 10. Critiques of EI include that: 1. a definitive model for measuring EI has not been established. 2. participants can falsely self-report their EI. 3. the changing definition of EI causes confusion. a. 1 and 2 b. 1 and 3 c. 2 and 3 d. 1, 2, and 3 11. Which leadership style is used most in health care? a. servant b. transactional c. transformational d. situational 12. Which leadership model encourages the leader to focus on the welfare of the follower rather than on the glorification of the leader? a. servant b. transactional c. transformational d. situational 6. In the courageous follower model, the follower should: 1. take a moral stand when warranted to prevent ethical abuses or to refuse to
- 52. participate in them. 2. participate in any transformation needed to improve the leader-follower relationship and the organization’s performance. 3. constructively challenge the leader or group’s behaviors or policies if these threaten the common purpose. a. 1 and 2 b. 1 and 3 c. 2 and 3 d. 1, 2, and 3 7. The ______ follower will do enough to retain the current position but no more. a. resourceful b. partner c. implementer d. individualistic 8. ______ leadership is demonstrated by a member in a workgroup, such as a collection of staff technologists, in which a secondary leadership role is shared. a. Formal b. Servant c. Informal d. Alternative 9. Which of the following is not a domain of emotional intelligence (EI)? a. knowing one’s emotions b. recognizing the emotions of others c. motivating oneself by organizing emotions
- 53. d. manipulating the emotions of others ✁ Carefully cut or tear here. Serving, Following, and Leading in Health Care Expiration Date: August 31, 2020* Approved for 1.5 Category A credits1 7 8 0 4 - 0 1 -- A passing score is 75% or better. -- Take the quiz online at asrt.org/drquiz for immediate results and your CE certificate. -- Or, mail the original answer sheet to Processing Center 2908 Stewart Creek Blvd., Charlotte, NC 28216. -- ASRT must receive this answer sheet before the quiz expires and before the end of the CE biennium for which you want credit. -- To see a list of the Directed Readings available to you, visit asrt.org/drquiz. -- To evaluate this Directed Reading, visit asrt.org/dreval. CE Answers Section 2 1 A B C D 2 A B C D 3 A B C D
- 54. 4 A B C D 5 A B C D 6 A B C D 7 A B C D 8 A B C D Note: For true/false questions, A=true, B=false. USE A BLACK INK PEN. Completely fill in the circles. Get immediate Directed Reading quiz results and CE credit when you take your test online at asrt.org/drquiz. *Some quizzes are renewed and the expiration date extended. Check online at asrt.org/drquiz or call Member Services at 800- 444-2778. 2 We need your ASRT Member ID and your two-digit Birth Month to track your CE credits. Be sure to use your ASRT Member ID and not your ARRT Registry Number. Birth Month ASRT Member ID 4 3 5 2 5 1 2 To ensure proper credit, please print the following information. Identification Section Member Information Section
- 55. Name City State Email 9 A B C D 10 A B C D 11 A B C D 12 A B C D 0252408281 Copyright of Radiologic Technology is the property of American Society of Radiologic Technologists and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use. 126 What Can Be Done About A Disruptive Physician?
- 56. A Legal Analysis Samuel D. Hodge, Jr.* House, a medical drama about an infectious disease specialist, entertained television audiences for years as the irascible and pill-popping physician solved medical mysteries with the zeal of a modern-day Sherlock Holmes while playing mind games with his coworkers. Uncanny intuition and eccentric thinking earned the physician great respect but his bullish behavior and antisocial tendencies were a distraction at the hospital.1 Not only did Dr. House clash with his fellow physicians but he also insulted patients, flouted hospital rules and caused great conflict with the hospital administrators.2 In fact, his actions often crossed the line into obnoxiousness and rage causing the hospital staff to tiptoe around his dysfunctional behavior.3 In the real world, Dr. House would be labeled a “disruptive physician” and would be subjected to disciplinary action
- 57. including the loss of his hospital privileges. This article will explore the problems caused by being labeled a disruptive physician in a legal context with a focus on the peer review process and the relevant court cases. TABLE OF CONTENTS I. Introduction...................................................................... 127 * The author is a professor at Temple University, where he teaches both law and anatomy. He also serves as a mediator and neutral arbitrator for the Dispute Resolution Institute in Philadelphia and is considered one of the most popular CLE speakers in the country. Professor Hodge has authored more than 175 articles on the intersection between law and medicine, has published ten books and has been named a top lawyer in Pennsylvania on multiple occasions. 1. House (TV Series), Wɪᴋɪᴘᴇᴅɪᴀ, https://en.wikipedia.org/wiki/House_ (TV_series), (last visited Sept. 14, 2019). 2. Id.
- 58. 3. Bob Wachter, Gregory House, MD, RIP, HOSPITAL LEADER BLOG (May 21, 2012), https://thehospitalleader.org/gregory-house-md-rip/. 1 2019 DISRUPTIVE PHYSICIAN? 127 II. What is a Disruptive Physician? .................................. 128 III. The Problem .................................................................. 129 A. Statistics .................................................................... 129 B. Conduct That Is Disruptive ....................................... 130 IV. Remedial Measures ....................................................... 131 A. The American Medical Association ........................... 132 B. The Joint Commission ............................................... 133 C. Federation of State Medical Boards .......................... 134 D. Response by the States .............................................. 135 V. Peer Review Immunity ................................................. 136 VI. Court Action ................................................. ................. 139
- 59. A. Immunity under the Healthcare Quality Improvement Act (HCQIA) ........................................................................ 141 B. Reliance upon Bylaws and Procedures ..................... 147 C. Disruptive Conduct as Justification for Suspension . 150 VII. Conclusion ..................................................................... 152 I. Introduction The practice of medicine is filled with stress from being involved in life and death decisions, to declining revenues while practicing in a heavily regulated environment.4 These facts have triggered the quick response by some physicians to use regulatory schemes to advance their own personal agendas and to protect personal interests.5 Unfortunately, these rules and regulations, which are not well understood by most medical professionals, have caused a great deal of animosity and frustration, leading some doctors to become “disruptive physicians.”6
- 60. The troublesome physician causes untold medical, legal, and psychological problems in the workforce,7 and most health care managers are ill prepared to deal with these doctors.8 For 4. Michael J. Grogan & Paul Knechtges, The Disruptive Physician: A Legal Perspective, 20 Aᴄᴀᴅ. Rᴀᴅɪᴏʟᴏɢʏ 9, 1069–73 (2013). 5. Zachary L. Erwin, Analyzing the Disruptive Physician: How State and Federal Courts Should Handle Whistleblower Cases Brought by Disruptive Physicians, 44 Dᴜǫ. L. Rᴇᴠ. 275, 275 (2006). 6. Id. at 276. 7. Id. 8. Eugene Fibuch & Jennifer J. Robertson, Bringing Value: Dealing Fairly With Disruptive Physicians, AM. ASS’N PHYSICIAN LEADERSHIP (Mar. 8, 2019), https://www.physicianleaders.org/news/bringing-value-dealing- fairly- 2https://digitalcommons.pace.edu/plr/vol40/iss1/3 128 PACE LAW REVIEW 40.1 example, disruptive physicians can lead to a hostile work
- 61. environment, cause morale problems, increased litigation, compromised patient care, communication issues, and obstruction in the regular running of the organization.9 As noted by Alexander Vaccaro M.D., the President of the Rothman Institute, “There is no place in medicine for disruptive physicians and every study that has examined the issue has concluded that a disruptive doctor increases the chance of an adverse event. In fact, these physicians have a higher complication rate and receive negative feedback in patient satisfaction surveys.”10 Addressing this conduct head-on is critical, but recognizing the proper course of remedial action can be a daunting task.11 II. What is a Disruptive Physician? No single definition exits to describe a disruptive physician but a number of organizations and court decisions have addressed the issue. Some medical professionals claim that
- 62. they have an “instinctive understanding” of what represents disruptive behavior and do not need guidance.12 On the other hand, the Court in Gordon v. Lewistown defines a disruptive physician as one who is unruly, “contentious, threatening, unreachable, insulting and frequently litigious. He will not, or cannot, play by the rules, nor is he able to relate to or work well with others.”13 It is important to note, however, that a sole occurrence of troublesome behavior is inadequate to be labeled a disruptive physician and anticipating complete harmony in the workplace is unrealistic. The tag should also not be used to disruptive-physicians. 9. Erwin, supra note 5, at 275–76. 10. Alexander Vaccaro, M.D., Ph.D, MBA, is an orthopedic surgeon and the President of Rothman Institute, one of the largest orthopedic practices in the country. He is also the Richard H. Rothman Professor and Chair in the Department of Orthopaedic Surgery, and a Professor of Neurosurgery at
- 63. Thomas Jefferson University in Philadelphia, Pennsylvania. His comments were obtained in a telephone interview conducted by the author on September 20, 2019. 11. Alicia Gallegos, Disruptive Physicians: Is This an HR or MEC Issue?, MDEDGE (Sept. 16, 2018), https://www.mdedge.com/internalmedicine/article /174921/businessmedicine/disruptive-physicians-hr-or-mec- issue. 12. Grogan & Knechtges, supra note 4, at 2. 13. Gordon v. Lewistown Hosp., 714 A.2d 539, 544 (Pa. Commw. Ct. 1998). 3 2019 DISRUPTIVE PHYSICIAN? 129 describe a doctor who has had a bad day or demonstrates an occasional outburst that is out of character. Nor should the label apply to a physician who has quirks, tends to be disagreeable, or annoys others on the medical staff.14 Rather, the characterization should be reserved for those who show a pattern of seriously inappropriate conduct that is “deep-seated
- 64. and habitual.”15 A single incident that is improper must still be addressed but the label “disruptive physician” is reserved for more sustained and inappropriate behaviors over a period of time.16 III. The Problem As the sophistication and intricacies of medicine and managed health care increase, the need to work in a conducive atmosphere of cooperation intensifies. Contemporaneously, the pressures, burdens, and distractions involving physicians correspondingly escalate. Because doctors occupy an esteemed position in society, inappropriate actions by these individuals become magnified and have a greater probability for disruption.17 Acknowledged in the medical literature for more than a century,18 there is little evidence to demonstrate that the number of episodes of disruptive physicians has increased in recent years, but the problem has moved to the forefront of
- 65. healthcare management. Likewise, doctors who demonstrate inappropriate behavior are being sanctioned with greater frequency.19 A. Statistics 14. Grogan & Knechtges, supra note 4, at 3; See also Mahmoodian v. United Hosp. Ctr., 404 S.E.2d 750 (W. Va. 1991). 15. Norman T. Reynolds, Disruptive Physician Behavior: Use and Misuse of the Label, 98 J. MED. REG. 1, 10 (2012). 16. Id. at 9–10. 17. Brian J. Santin & Krista L. Kaups, The Disruptive Physician: Addressing the Issues, BULL. AM. COLL. SURGEONS (Feb. 1, 2015), http://bulletin.facs.org/2015/02/the-disruptive-physician- addressing-the- issues/. 18. Llewellyn E. Piper, Addressing the Phenomenon of Disruptive Physician Behavior, 22 HEALTH CARE MANAGER 335, 335– 39 (2003). 19. Santin & Kaups, supra note 17.
- 66. 4https://digitalcommons.pace.edu/plr/vol40/iss1/3 130 PACE LAW REVIEW 40.1 Most physicians and other health care workers have seen their contemporaries engage in disruptive conduct with co- employees, patients, and other individuals.20 In fact, more than seventy percent of doctors surveyed indicate that disruptive conduct happens at least once a month at their workplace, and more than ten percent admit that such episodes occur on a daily basis.21 This disruptive behavior runs the gamut from cursing to the refusal to follow established procedures.22 Most responders expressed concern about the consequences of this inappropriate conduct on their practices, and nearly all are of the opinion that the disruptive physician affects patient care. Surprisingly, twenty-six percent of doctors acknowledged that they have engaged in disruptive conduct at some point during their careers and the most proffered reasons for these inappropriate actions
- 67. are “workload and learned behaviors.”23 Demographically, nurses are the main victims of this unseemly conduct,24 and a number have left their jobs as a result.25 The greatest offenders are those with the highest stress level jobs, with surgeons being labeled the greatest culprits, followed by obstetricians/gynecologists, orthopedic doctors, and primary care physicians.26 Other specialists with less frequent episodes include cardiologists, anesthesiologists, ophthalmologists, cardiac/vascular surgeons, kidney specialists, radiologists, oncologists, and psychiatrists.27 B. Conduct That Is Disruptive 20. Id. 21. Owen MacDonald, Disruptive Physician Behavior, QUANTIAMD 1, 2 (May 15, 2011), http://www.quantiamd.com/q- qcp/Disruptive_Physician_ Behavior.pdf. 22. Id. at 2. 23. Id.
- 68. 24. Stephen Lazoritz, Don’t Tolerate Disruptive Physician Behavior, AM. NURSE TODAY (Apr. 11, 2011), https://www.americannursetoday.com/dont- tolerate-disruptive-physician-behavior-2/. 25. Charles P. Samenow et. al., ACME Course Aimed at Addressing Disruptive Physician Behavior, PHYSICIAN EXEC. 32 (Jan.– Feb. 2008), https://www.mc.vanderbilt.edu/root/pdfs/cph/Samenow.pdf. 26. Alan H. Rosenstein et. al., Legal Entanglements in Dealing with Disruptive Behavior, PHYSICIAN LEADERSHIP J., May–June 2016, at 46, 48 fig. 2. 27. Id. 5 2019 DISRUPTIVE PHYSICIAN? 131 Inappropriate conduct takes many forms, with the highest level of encounters being degrading comments, insults, and yelling. Other types of disruptive behavior are less obvious but no less concerning. These include a physician’s refusal to
- 69. cooperate with others and the inability to adhere to established protocols. Conduct which occurs less frequently includes physician assaults, discriminatory behavior, incompetence, retaliation, spreading malicious rumors, throwing objects, and substance abuse.28 Female physicians are slightly less likely to engage in disruptive conduct as compared to their male counterparts.29 It is believed that disruptive physicians direct their actions against those who are perceived as having a status below the doctor. It is theorized that the hierarchical character of the medical profession has produced alphas who feel compelled to flaunt their status. Therefore, it should come as no surprise that one study ascertained that fifty percent of the conflicts dealing with disruptive doctors involve coworkers with less professional clout.30 Critics of this label maintain that being designated a disruptive physician has been applied improperly by hospital management to jettison unwanted competition and anti-
- 70. administration practices. It is also asserted that the phrase “disruptive physician” is buried in the bylaws and left intentionally broad, subjective, and undefined so that health care executives can construe it anyway they wish.31 Therefore, it is critical that hospitals implement rules and regulations that will assist them in the handling of disruptive doctors whil e shielding physicians from bogus claims of disruptive conduct.32 IV. Remedial Measures 28. MacDonald, supra note 21, at 4–5. 29. Id. at 5. 30. Brian M. Peters, Disruptive or Targeted Physician?: Compliance Strategies, HOSP. & HEALTH SYS. INST., February 9, 2006, Am. Health Law. Ass’n, AHLA-Papers P0209-608 (citing David O. Weber, Poll Results: Doctors’ Disruptive Behavior Disturbs Physician Leaders, PHYSICIAN EXEC., Sept.–Oct. 2004, at 6). 31. Lawrence R. Huntoon, Abuse of the “Disruptive Physician” Clause, 9 J. AM. PHYSICIANS AND SURGEONS 68, 68 (2004).
- 71. 32. Peters, supra note 30, at 4. 6https://digitalcommons.pace.edu/plr/vol40/iss1/3 132 PACE LAW REVIEW 40.1 A. The American Medical Association The first remedial attempt by the medical profession occurred at the 1999 Annual Meeting of the AMA House of Delegates who adopted Resolution 9 (A-99) dealing with the disruptive physician. The pronouncement requested the AMA to “identify and study behavior by physicians that is disruptive to high quality patient care.”33 The end result was the enactment of AMA Policy E-9.045 titled Physicians with Disruptive Behavior. This rule of ethics labels disruptive behavior as personal conduct, whether verbal or physical, that negatively affects or that potentially may adversely impact patient care. This inappropriate conduct is not limited to those actions that interfere with one’s ability to work with others on
- 72. the health care team. Physician criticism, however, that is provided in good faith with the intent of improving patient care should not be classified as disruptive behavior.34 The AMA also published a Model Medical Code of Conduct that can be used by health care facilities in drafting their bylaws.35 This Code defines disruptive behavior as “any abusive conduct including sexual or other forms of harassment, or other forms of verbal or nonverbal conduct that harms or intimidates others to the extent that the quality of care or patient safety likely would be compromised.”36 Inappropriate behavior is discouraged, but if such conduct persists, it will be transformed into disruptive behavior. Examples include: belittling or berating patients or members of their care team, use of profanity or disrespectful 33. Dudley M. Stewart, Jr., Physicians with Disruptive Behavior, Report of the Council on Ethical and Judicial Affairs, CEJA Report 3- 1-09, AMERICAN
- 73. MEDICAL ASS’N 1, 1 (2009), https://www.ama- assn.org/sites/ama-assn.org/ files /corp/media-browser/public/about- ama/councils/Council%20Reports/council- on-ethics-and-judicial-affairs/i09-ceja-physicians-disruptive- behavior.pdf. 34. Id. at 2 (citing AMA Opinion 9.045 – Physicians with Disruptive Behavior). 35. AMERICAN MEDICAL ASS’N, Model Medical Staff Code of Conduct (2012), https://www.slideshare.net/BarneyCohen/amamedicalstaffcodeof conduct (last visited Oct.4, 2019). 36. Id. at 1. 7 2019 DISRUPTIVE PHYSICIAN? 133 language, inappropriate comments written in a patient’s chart, blatant failure to respond to a patient’s needs, deliberate lack of cooperation with members of the medical staff, the deliberate refusal to return calls, and use of intentionally
- 74. demeaning language that negatively impacts patient care.37 The Code goes on to note that complaints about a physician should be in writing and directed to the president of the medical staff. A copy of the complaint, Code of Conduct, and bylaws should be given to the accused within thirty days. In turn, the offending member shall have the opportunity to respond in writing.38 B. The Joint Commission The Joint Commission, which is the accrediting agency for more than 22,000 health care organizations in the United States,39 published Standard LD.03.01.01. This provision acknowledges that a disruptive physician engages in “behavior that intimidates others and affects morale or staff turnover[,] undermines a culture of safety and can be harmful to patient care.”40 As a result, the Joint Commission requires health care organizations to establish a code of conduct that defines
- 75. behaviors that are “acceptable,” “disruptive,” and “inappropriate.”41 This problem is so significant that the Joint Commission subsequently issued a Sentinel Event Alert which notes that intimidating and disruptive behaviors can lead to medical errors, poor patient satisfaction, increased cost of care, and 37. Id. at 2–3. 38. Id. at 5. 39. About the Joint Commission, JOINT COMMISSION, https:// www.jointcommission.org/about_us/about_the_joint_commissio n_main.aspx (last visited Oct. 4, 2019). 40. LD.03.01.01: Leaders Create and Maintain a Culture of Safety and Quality Throughout the Hospital, JOINT COMMISSION 1, 1 https:// medschool.ucla.edu/workfiles/Site- AcademicAffairs/Events/17.Joint- Commission.pdf (last visited Oct. 4, 2019). 41. Stewart, Jr., supra note 33, at 1–2. 8https://digitalcommons.pace.edu/plr/vol40/iss1/3
- 76. 134 PACE LAW REVIEW 40.1 avoidable adverse outcomes.42 In response to criticism that the term “disruptive behavior” is both ambiguous and inaccurate, the definition was changed to “behavior or behaviors that undermine a culture of safety.”43 C. Federation of State Medical Boards The Federation of State Medical Boards recognized the need to issue guidance on the disruptive physician when it issued the 2000 Report of the Special Committee on Professional Conduct and Ethics, as well as in the 2011 Policy on Physician Impairment.44 The Special Committee’s Report defines disruptive behavior as “personal interaction with physicians, hospital personnel, patients, family members, or others that interferes with patient care.”45 Furthermore, disruptive behavior is not a diagnosis but a descriptive label that impairs the ability of the healthcare team to operate effectively, thereby placing patients at risk. More specifically, it identified several
- 77. ways in which disruptive conduct interferes with the doctor/patient relationship: 1. The physician’s inappropriate behaviors or emotional outbursts shift the physician’s focus from the patient, which can result in errors in clinical judgment and performance. 2. Physician’s emotional outbursts or other inappropriate behavior can increase apprehension and anxiety of the physician’s patients as well as other patients who may witness such outbursts and inappropriate behavior. 42. JOINT COMMISSION, Behaviors that Undermine a Culture of Safety (July 9, 2008), https://www.jointcommission.org/assets/1/18/SEA_40.pdf. 43. Joint Commission Changes Term “Disruptive Behavior” in the Standards, HCPRO (Nov. 10, 2011), https://www.hcpro.com/ACC-273165- 851/Joint-Commission-changes-term-disruptive-behavior-in-the- standards.html.
- 78. 44. Reynolds, supra note 15, at 8. 45. Federation of State Medical Boards, Report of the Special Committee on Professional Conduct and Ethics 1, 5, (Apr. 2000), http://www.fsmb.org /siteassets/advocacy/policies/report-of-the-special-committee- on-professional- conduct-and-ethics.pdf. 9 2019 DISRUPTIVE PHYSICIAN? 135 3. Decreased effectiveness of the entire health team. Peers, nurses, allied health professionals, and other members of the health care team may be intimidated and anxious, causing a loss of their clinical focus and productivity and thereby increasing the propensity for medical errors. 4. Decrease in effective communications among the health care team.46
- 79. The Report went on to note that disruptive behavior in doctors is frequently the result of underlying pathology such as: “(1) addiction (2) stress (3) psychiatric disorders (e.g., bipolar disorder) or (4) personality disorders (e.g., narcissism).”47 Personality disorders seem to be the cause of most referrals for disruptive behavior which may be treated, without or concurrent with punitive action.48 D. Response by the States States have also taken steps to curb unprofessional medical conduct. For instance, New York lists a number of ways that individuals can engage in professional misconduct under its public health law including “willfully harassing, abusing, or intimidating a patient either physically or verbally.”49 The Texas Medical Association deems a health care professional who engages in conduct that leads to a breakdown in safety measures or acts in an intimidating manner towards a member of the medical staff to be engaged in disruptive behavior.50
- 80. Pennsylvania enacted the Peer Review Protection Act which provides that one offering information to any review organization shall be granted immunity unless the information is not related to the functions of the review entity or if the 46. Id. at 5–6. 47. Id. at 6. 48. Id. 49. N.Y. Educ. § 6530(31) (McKinney 2008). 50. Crystal Conde, Joint Commission Tries to Regulate Physicians’ Behavior, TEX. MED. (Dec. 2009), https://www.texmed.org/Template.aspx?id =8189. 10https://digitalcommons.pace.edu/plr/vol40/iss1/3 136 PACE LAW REVIEW 40.1 materials provided are false and the individual knew or had reason to think the material was false.51 Failure of the facility to implement remedial measure to
- 81. deal with disruptive physicians can result in expensive litigation. This is evidenced by a number of costly discrimination/harassment lawsuits against health care facilities as the result of the disruptive physician.52 For instance, Chopourian v. Mercy General Hospital involved a federal matter in which the jury awarded $168 million to a forty- five-year-old physician’s assistant who claimed that she was tormented and harassed by the surgeons and medical staff.53 The plaintiff testified that one harasser informed her, “you’ll give in to me” and a surgeon told her that “I’m horny” and slapped her buttocks.54 A “bullying surgeon” stuck her with a needle and another called her a “stupid chick” in the operating room.55 V. Peer Review Immunity Interacting with disruptive physicians can be a time- consuming and emotionally exhausting endeavor for both management and the organization. Nevertheless, health care
- 82. leaders have a duty to investigate and stop unprofessional conduct in the workplace.56 This requires the implementation of an organized approach such as educating the staff as to what constitutes improper behavior and to clearly identify the penalties for engaging in such conduct.57 For example, a code of conduct or bylaws should be created which applies to all members of the health care team. These directives should define what constitutes appropriate and inappropriate behavior in 51. 63 PA. STAT. and CONS. STAT. ANN. § 425.3(a) (West 2019). 52. Alice Gosfield, 2013 Health Law Handbook, Section 11:2. Scope of the Problem, at *4. 53. Eugene Lee, Largest Sexual Harassment Verdict in History - $168 Million, CAL. LAB. & EMP. L., https://calaborlaw.com/largest- sexual- harassment-verdict-in-history-168-million/ (last visited Oct. 4, 2019). See also Chopourian v. Catholic Healthcare West, No. CIV S–09–2972, 2012 WL
- 83. 1551728 (E.D. Cal. 2012). 54. Lee, supra note 53. 55. Gosfield, supra note 52, at *4. 56. Fibuch & Robertson, supra note 8. 57. Id. 11 2019 DISRUPTIVE PHYSICIAN? 137 clear and precise language and contain a well-defined due process clause with an appeal process. In turn, each physician should be asked to read and sign the document indicating an understanding of the rules.58 A number of hospitals publish these rules under the category of “professionalism,” and mandate that physicians exhibit a minimum level of acceptable behavior towards co- workers and patients. Any violation of the rules may act as support for starting disciplinary action to address the conduct.59 While differences in language and procedures among health car e
- 84. facilities is expected, common elements, include: Clearly explained behaviors that are expected; The repercussions for deviation from these behaviors should be explained in detail; Penalties should be staggered according to the severity of the incident; Those who commit repeat violations will be treated more harshly; and Every incident must be reported and documented.60 This plan of action helps foster a positive atmosphere within the organization and members of the team are put on notice as to what is expected of them in the workplace.61 Discipline against a disruptive physician, however, can result in retaliation by the offender, especially if the doctor’s hospital privileges are suspended.62 A key event in this regard occurred in 1988 when the United States Supreme Court decided Patrick v. Burget.63 This matter involved whether Oregon law protected physicians against federal antitrust liability as the result of their serving on a peer-review committee.64 The facts reveal that the plaintiff declined an invitation by the defendants
- 85. to join their surgical practice.65 Instead, the plaintiff opened his own clinic but experienced problems in his dealings with the defendants.66 The dispute escalated into a peer-review proceeding to terminate the plaintiff’s hospital privileges at the 58. Id. 59. Santin & Kaups, supra note 17, at 3. 60. Id. 61. Fibuch & Robertson, supra note 8. 62. See Hein-Muniz v. Aiken Reg’l Med. Ctr., 905 F. Supp. 2d 729 (D.S.C. 2012). 63. Patrick v. Burget, 486 U.S. 94 (1988). 64. Id. at 95–96. 65. Id. at 96. 66. Id. 12https://digitalcommons.pace.edu/plr/vol40/iss1/3 138 PACE LAW REVIEW 40.1
- 86. city’s only hospital on the ground that his care of patients was below the hospital’s standards.67 The plaintiff filed a federal lawsuit claiming violations of the Sherman Act by the defendant’s charges and by their participating in the peer-review proceeding in order to reduce competition from the plaintiff rather than to improve patient care.68 The Supreme Court ruled that the state’s law failed to shield the defendants from liability for their activities on the hospital peer-review committee.69 This ruling prompted Congress to enact the Health Care Quality Improvement Act of 1986.70 The legislature found that the threat of money damages under Federal law unreasonably dissuaded doctors from serving on professional peer review committees. Therefore, there is a national overriding interest to protect physicians who serve in this capacity.71 This statute offers immunity under Federal and State laws to those on a peer review body who act in the reasonable belief that their action was in the furtherance of quality health care,
- 87. and they act after a reasonable effort to obtain the facts even though their actions adversely impact the clinical privileges or professional society membership of a physician.72 This statute sets forth the specific requirements and standards for immunity and applies to disruptive physician cases.73 Only a good faith review qualifies for immunity, so whether the standards are followed by the peer review committee is very important to the final disposition of most disruptive physician cases and is the subject of much litigation.74 It must be noted, however, that the Act only grants immunity to “professional review actions.”75 This is defined as an action or recommendation by the professional review body which is done during a review activity, that is premised on the competence or professional actions of a doctor, and which may 67. Id. at 97. 68. Id. at 97–98. 69. Patrick, 486 U.S. at 105.
- 88. 70. Health Care Quality Improvement Act of 1986, 42 U.S.C. § 11101 (2019). 71. Id. 72. Id. 73. Erwin, supra note 5, at 281–80. 74. Id. at 280. 75. Gosfield, supra note 52, at *1. 13 2019 DISRUPTIVE PHYSICIAN? 139 adversely affect the clinical privileges of the physician.76 VI. Court Action Being labeled a disruptive physician, especially if sanctions are imposed, can have serious professional implications including the loss of one’s hospital privileges. In fact, it can have career ending repercussions. State and federal agencies can also
- 89. discipline a physician who is labeled disruptive if the offending conduct is determined to influence the quality of patient care or if it implies moral, ethical, or unprofessional deficiencies.77 Unhappy patients can register a complaint with the health plan or managed health care firm triggering an investigation that can cause the loss of a physician’s affiliation with the plan or hospital. Intimating and unprofessional conduct can also be reported to the National Practitioner Data Bank, thereby resulting in other investigations and charges against the physician who seeks a hospital affiliation or credentialing.78 This data bank79 maintains a listing of actions taken by authorized organizations regarding health care practitioners, entities, providers, and suppliers who do not meet professional standards. These adverse reports are permanently kept unless modified or removed by the entity that submitted them.80 In turn, the information can be used in rendering decisions dealing with licensure, employment, contracting, membership or clinical privileges, or when conducting investigations. Under the