DEFINITION
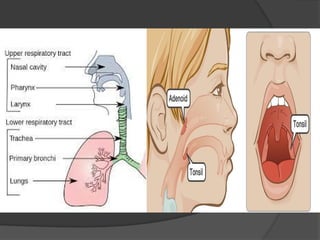
An upperrespiratory tract infection, or
upper respiratory infection, is an
infectious process of any of the
components of the upper airway.
1. Common cold
Colds often go away on their own. Colds can:
Occur at any age.
Have a wide range of symptoms.
Spread through direct contact with respiratory secretions
Last about 7 to 10 days, though a cough can last up to
three weeks.
Lead to complications such as ear infections, eye
infections, sinus infections and pneumonia.
Treatment
Use acetaminophen
Stay hydrated.
Get plenty of rest.
5.
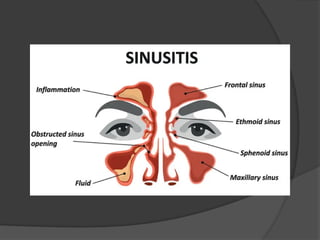
2. Sinusitis
Sinusitis,or a sinus infection, is a common problem.
S/S
Postnasal drip (mucus dripping into throat)
Green mucus from nose.
Stuffiness or congestion.
Pain when press on face, especially on the bones right under
eyes.
Bad breath.
Cough.
Fatigue.
Fever.
Headaches
Treatment
Antibiotics may be needed to clear up a sinus infection in this case
7.
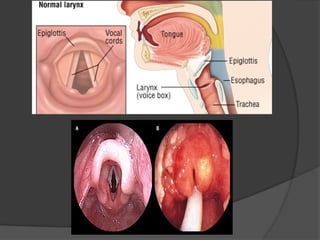
3. Epiglottitis
Epiglottitisis when the epiglottis gets inflamed.
This condition can be serious, it can block your airway.
Symptoms of epiglottitis include:
Difficulty breathing or swallowing.
Fever and Severe sore throat.
Epiglottitis requires treatment at a hospital or medical facility.
Supplemental oxygen
IV fluids to keep you hydrated until you can swallow
without problems.
Antibiotics, if your provider thinks you may have a
bacterial infection.
Steroids to reduce the swelling.
9.
4. Pharyngitis
Pharyngitisis also known as a sore throat.
S/S
Severe throat pain.
Difficulty swallowing and speaking.
Ear pain.
Tender lymph nodes in the neck.
Swollen, red tonsils.
Treatment
If the throat swab (strep test) is positive for strep throat, take a course
of antibiotics, such as penicillin.
If the test is negative, may recommend:
Over-the-counter pain relievers, such as acetaminophen or NSAIDs,
to help with throat pain.
Gargling with warm salt water to soothe your throat.
A single dose of a steroid to help with symptoms.
10.
5. Laryngitis
Laryngitisis when the larynx becomes inflamed.
s/s
Become very hoarse.
Only be able to talk at a low volume.
Lose voice entirely.
a fever, have difficulty swallowing and sore throat.
Treatment
Voice rest. Try not to speak. If you do need to speak, talk in a
low voice rather than a whisper. Whispering can irritate larynx.
Drink plenty of extra fluids.
Breathe in steam.
Use cough suppressants.
12.
Clinical features
Cough.
Fever.
Hoarse voice.
Fatigue and lack of energy.
Red eyes.
Runny nose.
Sore throat.
Swollen lymph nodes (swelling on the
sides of your neck).
Do’s
Live a healthylifestyle:
Wash hands, especially
before eating or
preparing food.
Sneeze and cough into a
tissue and wash hands
after.
Take rest
Avoid contact with sick
Drink plenty of fluids.
Get enough sleep.
Treatment
Head elevation
Gargling
Steam inhalation
Antibiotic therapy
Keep up with routine
checkups and
immunizations.
get the pneumococcal
vaccine, which prevents
pneumonia.
15.
Don’ts
do notlet children breathe in steam from
a bowl of hot water as there's a risk of
scalding
do not give aspirin to children under 16
do not smoke – it may worsen
symptoms
Do not allow visitors
Don’t smoke
Incidence
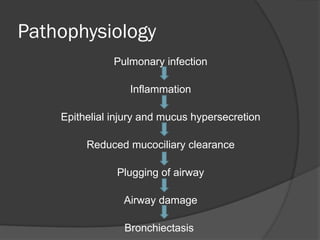
Bronchiectasis predominantlyaffect
extremes of age.
The prevalence of bronchiectasis rises
steeply from 4-5 per 100,000 adults
aged 18-34 years to 250 to 300 per
100,000 individuals aged > 75 years.
19.
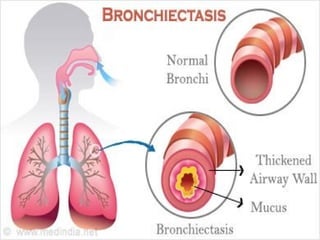
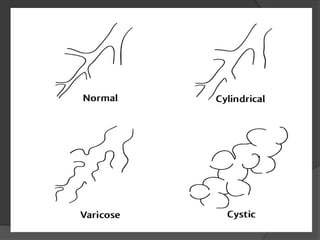
Types
Cylindrical bronchiectasis: it’s a
mildest form and reflects the loss of
the normal tapering of the airways.
Saccular bronchiectasis : its more
severe, with further distortion of the
airway. Produce sputum
Cystic bronchiectasis : is the most
severe form , chronic productive
cough.
21.
Risk factors
• Primarydisorders of structures in the bronchi
• Severe childhood bronchial infection
• Inflammatory disease
• Pneumonia
• Inhaled foreign bodies
• Bronchial tumors
• Tuberculosis
• Cystic fibrosis-Inherited disorder, which affect
the cells that produce mucus, sweat &
digestive juice. Causes these fluid thick &
sticky, then they plug tubes, duct & passage
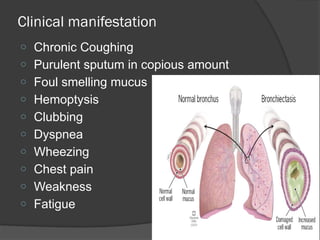
Clinical manifestation
o ChronicCoughing
o Purulent sputum in copious amount
o Foul smelling mucus
o Hemoptysis
o Clubbing
o Dyspnea
o Wheezing
o Chest pain
o Weakness
o Fatigue
24.
Diagnostic measures
Historycollection
Physical examination
Chest x ray-opacities
Blood test
Sputum study
CT scan-excellent view of dilated bronchi
and bronchioles
Bronchoscopy-to find out the cause
PFT-find out the extend & severity of ds
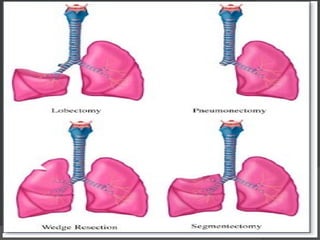
Surgical Management
Segmentalresection. The
diseased segment of a lobe is
removed.
Lobectomy. The diseased lobe is
removed.
Pneumonectomy. The entire
diseased lung segment is
removed, but this rarely happens.
28.
Complication
Atelectasis. Collapseof the alveoli
is a common complication.
Pneumonia. Infection is recurrent in
patients with bronchiectasis.
Empyema. Overproduction of
sputum causes the bronchi to be
filled with pus
29.
Nursing assessment
Nursingassessment of a patient with
bronchiectasis include:
Evaluation of current smoking status.
Evaluation of current exposure to
occupational toxins or pollutants and
in indoor/outdoor pollution.
Assess the patient’s current level of
functioning.
30.
Nursing Diagnosis
Impairedgas exchange related to
ventilation-perfusion imbalance.
Ineffective airway clearance related to
increased mucus production.
Ineffective breathing pattern related to
mucus and airway irritants.
Activity intolerance related to
hypoxemia and ineffective breathing
patterns.
31.
Nursing Intervention
Smokingcessation.
Bronchodilators. Administer
bronchodilators as prescribed.
Postural drainage. Perform postural
drainage with percussion and vibration in
the morning
Antibiotics. Administer antibiotics as
prescribed.
Activities. Encourage alternating activity
with rest periods.
32.
Client education
Smokingcessation.
Postural drainage.
Exposure to infections.
Signs of infection.
Nutrition.