35NURSING ECONOMIC$/January-February 2011/Vol. 29/No. 1
T
HE WORLD OF ARISTOTLE AND
Ptolemy believed that Earth
was positioned at the cen-
ter of the universe. Thanks
to Galileo and Copernicus’s studies
in the 16th century, we know this
is not true and that the sun is the
center of our universe. Pers -
pectives of health care have
undergone similar, radical changes
in perception. For centuries we
had a hospital-centric view; an
illness-based model, where the majority of care was
provided in hospitals, when we were ill. In the last
few decades, that model has migrated to a more con-
tinuum of care view; a wellness/health maintenance
model, where emphasis of care is outside the hospital
in other venues such as outpatient, ambulatory/clin-
ic, and home care (see Figure 1).
But as we all know, this is still not where we need
to be to support the highest quality care at the right
cost. Despite a focus on moving care out of the hospi-
tals, one only needs to think about the process of
medication reconciliation between care venues to
realize the lack of seamless integration of care deliv-
ery and the challenges of supporting interoperability
across the continuum. Hence, here I am proposing the
patient centric view, where the patient actively partic-
ipates in his or her care and we look at delivering care
from a patient’s point of view. This allows us to break
down some of the barriers we have struggled with on
our journeys to promote higher quality care through
the use of health information technology (HIT). Now
we need to consider how the health care system
should revolve around the patient, rather than the
patient rotating around the hospital. Considering a
patient-centric point of view when implementing and
optimizing the use of HIT provides new perspectives
on the meaning of “integrated” health care.
Patient-Centric Care
It might seem odd that a health care organization
needs to be reminded to involve the patient in his or
her care. After all, this approach would certainly be
supported from a patient’s perspective. And, of
course, the health care industry has compelling rea-
sons to incorporate a strong customer and service
focus in order to improve patient satisfaction and
impact patient loyalty. But as health care systems
Patient as Center of the Health Care Universe:
A Closer Look at Patient-Centered Care
JUDY MURPHY, RN, FACMI, FHIMSS, is Vice President-
Information Services, Aurora Health Care, Milwaukee, WI; a
HIMSS Board Member; Co-Chair of the Alliance for Nursing
Informatics; a member of the federal HIT Standards Committee;
and is a Nursing Economic$ Editorial Board Member. Comments
and suggestions can be sent to [email protected]
EXECUTIVE SUMMARY
We need to consider how the health care system
should revolve around the patient, rather than the
patient rotating around the hospital.
Considering a patient-centric point of view when
implementing and optimizing the use of health infor-
mation technology (HIT) provides new perspect ...
From Patients to ePatients Driving a new paradigm for online clinical collabo...ddbennett
CareTech eHealth Innovation Series
From Patients to ePatients Driving a new paradigm for online clinical collaboration and health management
David Bennett, SVP, Interactive Solutions
StayWell Custom Communications
Anthony Chipelo, Director, Portal Strategies
CareTech Solutions
· Normalize the following ER diagram. TABLE TALKTh.docxodiliagilby
· Normalize the following ER diagram.
TABLE TALK
The Growing Role of Patient
Engagement: Relationship-based
Care in a Changing Health Care
System
A
s health care providers, we rarely partici-
pate in discussions, watch interviews, or
read articles about our changing health
care system that do not concern patient engage-
ment. The Center for Advancing Health defines
patient engagement as
Actions individuals must take to obtain the
greatest benefit from the health care services
available to them. . . . Engagement is not syn-
onymous with compliance. . . . [Engagement]
signifies that a person is involved in a process in
which he [or she] harmonizes robust information
and professional advice with his [or her] own
needs, preferences, and abilities in order to
prevent, manage, and cure disease.
1
Patient engagement strategies have been shown
to improve care delivery and translate into better
outcomes related to patient satisfaction and re-
covery. One author captured the importance of
patient engagement with this statement: “If pa-
tient engagement were a [medication], it would
be the blockbuster [medication] of the century
Patient engagement begins with relationship-based care. (Nurse’s warm-up jacket
and cap not shown.)
http://dx.doi.org/10.1016/j.aorn.2014.02.007
� AORN, Inc, 2014 April 2014 Vol 99 No 4 � AORN Journal j 517
http://dx.doi.org/10.1016/j.aorn.2014.02.007
and malpractice not to use it.”
2
Yet widespread
consensus among health care providers about how
to engage patients is still being determined.
The nursing profession’s role in patient engage-
ment and advocacy is key to the care that we de-
liver and continues to evolve to meet the needs of
patients. For example, before the 1970s, there was
not a high demand for patient’s rights.
3
In 2006,
AORN published a position statement on creating
an environment of safety, which set the ground-
work for patient-centered care as an important
element in defining the perioperative culture.
4
A
number of ethical, philosophical, and professional
considerations related to the rights of patients
have led to the nurse’s role as patient advocate.
According to one author, the three components of
this role are
1. informing patients of their rights,
2. providing patients with information necessary
to making informed decisions, and
3. supporting patients in their decisions.5
Regarding the patient’s role in engagement, one
author, who is also a perioperative RN, shared his
experiences as a surgical patient. In his article,
McGowan suggested that almost every patient en-
ters the surgical suite with anxiety and looks to
the perioperative team for reassurances. He be-
lieves that inaccurate portrayals of surgery in the
media “contribute to patients’ perceptions of sur-
gery and not always in a positive way.”
6(p493)
Critical to the health care provider’s ability to
establish trust is communicating in a manner that
informs and empowers the pa ...
Overview of Patient Experience Definitions and Measurement ToolsInnovations2Solutions
This publication will provide an overview of patient experience, how it is measured, and how to achieve it optimally within the healthcare setting. Sodexo’s definition of Patient Experience will also be explored.
Patient Centered Medical home talk at WVUPaul Grundy
To employers the cost of healthcare is now a business issue and this talk is about what one large buyer IBM did to drive transformation via broad coalition with other large employers to form the Patient Centered Medical Home movement and the covenant between buyer and provider away from the garbage we now buy episodic uncoordinated disintegrated care. In the change of convenient conversation we have worked with the Primary care providers to give us coordinated, integrated, accessible and compressive care with a set of principles know as the Patient centered medical home.
A Patient Centered Medical Home (PCMH) happens when primary care healers keeping that core healing relationship with their patients step up to become specialists in Family and Community Medicine. The move is to the discipline of leading a team that delivers population health management, patent centered prevention, care that is coordination, comprehensive accessible 24/7 and integrated across a deliver system. PCMH happens when the specialists in Family and Community Medicine wake up every morning and ask the question how will my team improve the health of my community today?
All over the world three huge factors are in play that is driving the concept of Patient Centered Medical Home. They are:
1) Cost and demography
2) Information technology and data (information that is actionable will equal a demand for accountability by the payer or buyer of the care)
3) Consumer demand to engage healthcare differently (at least as well as they can their bank- on line) have a question about lab results why not e-mail?
But at its core it is a move toward integration of a healing relationship in primary care and population management all at the point of care with the tools to do just that.
TABLE TALKThe Growing Role of PatientEngagement Relatio.docxperryk1
TABLE TALK
The Growing Role of Patient
Engagement: Relationship-based
Care in a Changing Health Care
System
A
s health care providers, we rarely partici-
pate in discussions, watch interviews, or
read articles about our changing health
care system that do not concern patient engage-
ment. The Center for Advancing Health defines
patient engagement as
Actions individuals must take to obtain the
greatest benefit from the health care services
available to them. . . . Engagement is not syn-
onymous with compliance. . . . [Engagement]
signifies that a person is involved in a process in
which he [or she] harmonizes robust information
and professional advice with his [or her] own
needs, preferences, and abilities in order to
prevent, manage, and cure disease.
1
Patient engagement strategies have been shown
to improve care delivery and translate into better
outcomes related to patient satisfaction and re-
covery. One author captured the importance of
patient engagement with this statement: “If pa-
tient engagement were a [medication], it would
be the blockbuster [medication] of the century
Patient engagement begins with relationship-based care. (Nurse’s warm-up jacket
and cap not shown.)
http://dx.doi.org/10.1016/j.aorn.2014.02.007
� AORN, Inc, 2014 April 2014 Vol 99 No 4 � AORN Journal j 517
http://dx.doi.org/10.1016/j.aorn.2014.02.007
and malpractice not to use it.”
2
Yet widespread
consensus among health care providers about how
to engage patients is still being determined.
The nursing profession’s role in patient engage-
ment and advocacy is key to the care that we de-
liver and continues to evolve to meet the needs of
patients. For example, before the 1970s, there was
not a high demand for patient’s rights.
3
In 2006,
AORN published a position statement on creating
an environment of safety, which set the ground-
work for patient-centered care as an important
element in defining the perioperative culture.
4
A
number of ethical, philosophical, and professional
considerations related to the rights of patients
have led to the nurse’s role as patient advocate.
According to one author, the three components of
this role are
1. informing patients of their rights,
2. providing patients with information necessary
to making informed decisions, and
3. supporting patients in their decisions.5
Regarding the patient’s role in engagement, one
author, who is also a perioperative RN, shared his
experiences as a surgical patient. In his article,
McGowan suggested that almost every patient en-
ters the surgical suite with anxiety and looks to
the perioperative team for reassurances. He be-
lieves that inaccurate portrayals of surgery in the
media “contribute to patients’ perceptions of sur-
gery and not always in a positive way.”
6(p493)
Critical to the health care provider’s ability to
establish trust is communicating in a manner that
informs and empowers the patient. For example,
he stated that, as a pa.
S28 September-October 2016HASTINGS CENTER REPORTUndispu.docxWilheminaRossi174
S28 September-October 2016/HASTINGS CENTER REPORT
Undisputedly, the United States’ health care sys-
tem is in the midst of unprecedented complexi-
ty and transformation. In 2014 alone there were
well over thirty-five million admissions to hospitals in
the nation,1 indicating that there was an extraordinary
number of very sick and frail people requiring highly
skilled clinicians to manage and coordinate their com-
plex care across multiple care settings. Medical advances
give us the ability to send patients home more efficiently
than ever before and simultaneously create ethical ques-
tions about the balance of benefits and burdens associ-
ated with these advances. New treatments for cancer or
complex heart disease may prolong life until the disease
becomes irreversible while causing significant morbidity
that undermines functional status, independence, and
quality of life in ways that patients find unacceptable.
Some patients and families voice concerns about access
to treatments and about the quality and safety of the care
they or their loved ones receive.
Every day on every shift, nurses at the bedside feel
these pressures and the intense array of ethical issues that
they raise. A staggering 17.5 percent of trained nurses are
leaving their roles or the profession after less than one
year of service,2 and increasing levels of moral distress
and burnout contribute to their decisions.3 Meanwhile,
research supports the common-sense understanding that
patients and health care organizations fare better when
nurses are not harried, are supported in their work en-
vironments, and are able to practice high-quality, ethical
care.
At the same time, administrators, policy-makers, and
regulators struggle to balance commitments to patients,
families, staff members, and governing boards. Health
care organizations are compelled by laws, regulations,
and accrediting bodies to pursue externally reported
measures of effectiveness that can put their mission and
values at risk. While health care systems declare their
commitment to core ethical values, many clinicians
struggle to understand institutional priorities, budgets,
policies, and decisions seemingly inconsistent with their
values as professionals.
Increasingly clinicians find their ability to provide
compassionate care at odds with the intensifying focus
on matters such as clinical pathways aimed at standard-
izing care, cost-cutting efficiencies, electronic medical
records, and hospital policies and procedures.4 Arguably,
each of these have merit in the current system, but what
is not accounted for are the unintended consequences
of diverting attention from the core ethical values of the
professions. For example, the advent of the EMR requires
clinicians to focus on documentation rather than being
fully present during patient encounters. An emphasis on
clinical pathways increases the risk of reducing patient
symptoms and diseases to what fits a rote app.
From Patients to ePatients Driving a new paradigm for online clinical collabo...ddbennett
CareTech eHealth Innovation Series
From Patients to ePatients Driving a new paradigm for online clinical collaboration and health management
David Bennett, SVP, Interactive Solutions
StayWell Custom Communications
Anthony Chipelo, Director, Portal Strategies
CareTech Solutions
· Normalize the following ER diagram. TABLE TALKTh.docxodiliagilby
· Normalize the following ER diagram.
TABLE TALK
The Growing Role of Patient
Engagement: Relationship-based
Care in a Changing Health Care
System
A
s health care providers, we rarely partici-
pate in discussions, watch interviews, or
read articles about our changing health
care system that do not concern patient engage-
ment. The Center for Advancing Health defines
patient engagement as
Actions individuals must take to obtain the
greatest benefit from the health care services
available to them. . . . Engagement is not syn-
onymous with compliance. . . . [Engagement]
signifies that a person is involved in a process in
which he [or she] harmonizes robust information
and professional advice with his [or her] own
needs, preferences, and abilities in order to
prevent, manage, and cure disease.
1
Patient engagement strategies have been shown
to improve care delivery and translate into better
outcomes related to patient satisfaction and re-
covery. One author captured the importance of
patient engagement with this statement: “If pa-
tient engagement were a [medication], it would
be the blockbuster [medication] of the century
Patient engagement begins with relationship-based care. (Nurse’s warm-up jacket
and cap not shown.)
http://dx.doi.org/10.1016/j.aorn.2014.02.007
� AORN, Inc, 2014 April 2014 Vol 99 No 4 � AORN Journal j 517
http://dx.doi.org/10.1016/j.aorn.2014.02.007
and malpractice not to use it.”
2
Yet widespread
consensus among health care providers about how
to engage patients is still being determined.
The nursing profession’s role in patient engage-
ment and advocacy is key to the care that we de-
liver and continues to evolve to meet the needs of
patients. For example, before the 1970s, there was
not a high demand for patient’s rights.
3
In 2006,
AORN published a position statement on creating
an environment of safety, which set the ground-
work for patient-centered care as an important
element in defining the perioperative culture.
4
A
number of ethical, philosophical, and professional
considerations related to the rights of patients
have led to the nurse’s role as patient advocate.
According to one author, the three components of
this role are
1. informing patients of their rights,
2. providing patients with information necessary
to making informed decisions, and
3. supporting patients in their decisions.5
Regarding the patient’s role in engagement, one
author, who is also a perioperative RN, shared his
experiences as a surgical patient. In his article,
McGowan suggested that almost every patient en-
ters the surgical suite with anxiety and looks to
the perioperative team for reassurances. He be-
lieves that inaccurate portrayals of surgery in the
media “contribute to patients’ perceptions of sur-
gery and not always in a positive way.”
6(p493)
Critical to the health care provider’s ability to
establish trust is communicating in a manner that
informs and empowers the pa ...
Overview of Patient Experience Definitions and Measurement ToolsInnovations2Solutions
This publication will provide an overview of patient experience, how it is measured, and how to achieve it optimally within the healthcare setting. Sodexo’s definition of Patient Experience will also be explored.
Patient Centered Medical home talk at WVUPaul Grundy
To employers the cost of healthcare is now a business issue and this talk is about what one large buyer IBM did to drive transformation via broad coalition with other large employers to form the Patient Centered Medical Home movement and the covenant between buyer and provider away from the garbage we now buy episodic uncoordinated disintegrated care. In the change of convenient conversation we have worked with the Primary care providers to give us coordinated, integrated, accessible and compressive care with a set of principles know as the Patient centered medical home.
A Patient Centered Medical Home (PCMH) happens when primary care healers keeping that core healing relationship with their patients step up to become specialists in Family and Community Medicine. The move is to the discipline of leading a team that delivers population health management, patent centered prevention, care that is coordination, comprehensive accessible 24/7 and integrated across a deliver system. PCMH happens when the specialists in Family and Community Medicine wake up every morning and ask the question how will my team improve the health of my community today?
All over the world three huge factors are in play that is driving the concept of Patient Centered Medical Home. They are:
1) Cost and demography
2) Information technology and data (information that is actionable will equal a demand for accountability by the payer or buyer of the care)
3) Consumer demand to engage healthcare differently (at least as well as they can their bank- on line) have a question about lab results why not e-mail?
But at its core it is a move toward integration of a healing relationship in primary care and population management all at the point of care with the tools to do just that.
TABLE TALKThe Growing Role of PatientEngagement Relatio.docxperryk1
TABLE TALK
The Growing Role of Patient
Engagement: Relationship-based
Care in a Changing Health Care
System
A
s health care providers, we rarely partici-
pate in discussions, watch interviews, or
read articles about our changing health
care system that do not concern patient engage-
ment. The Center for Advancing Health defines
patient engagement as
Actions individuals must take to obtain the
greatest benefit from the health care services
available to them. . . . Engagement is not syn-
onymous with compliance. . . . [Engagement]
signifies that a person is involved in a process in
which he [or she] harmonizes robust information
and professional advice with his [or her] own
needs, preferences, and abilities in order to
prevent, manage, and cure disease.
1
Patient engagement strategies have been shown
to improve care delivery and translate into better
outcomes related to patient satisfaction and re-
covery. One author captured the importance of
patient engagement with this statement: “If pa-
tient engagement were a [medication], it would
be the blockbuster [medication] of the century
Patient engagement begins with relationship-based care. (Nurse’s warm-up jacket
and cap not shown.)
http://dx.doi.org/10.1016/j.aorn.2014.02.007
� AORN, Inc, 2014 April 2014 Vol 99 No 4 � AORN Journal j 517
http://dx.doi.org/10.1016/j.aorn.2014.02.007
and malpractice not to use it.”
2
Yet widespread
consensus among health care providers about how
to engage patients is still being determined.
The nursing profession’s role in patient engage-
ment and advocacy is key to the care that we de-
liver and continues to evolve to meet the needs of
patients. For example, before the 1970s, there was
not a high demand for patient’s rights.
3
In 2006,
AORN published a position statement on creating
an environment of safety, which set the ground-
work for patient-centered care as an important
element in defining the perioperative culture.
4
A
number of ethical, philosophical, and professional
considerations related to the rights of patients
have led to the nurse’s role as patient advocate.
According to one author, the three components of
this role are
1. informing patients of their rights,
2. providing patients with information necessary
to making informed decisions, and
3. supporting patients in their decisions.5
Regarding the patient’s role in engagement, one
author, who is also a perioperative RN, shared his
experiences as a surgical patient. In his article,
McGowan suggested that almost every patient en-
ters the surgical suite with anxiety and looks to
the perioperative team for reassurances. He be-
lieves that inaccurate portrayals of surgery in the
media “contribute to patients’ perceptions of sur-
gery and not always in a positive way.”
6(p493)
Critical to the health care provider’s ability to
establish trust is communicating in a manner that
informs and empowers the patient. For example,
he stated that, as a pa.
S28 September-October 2016HASTINGS CENTER REPORTUndispu.docxWilheminaRossi174
S28 September-October 2016/HASTINGS CENTER REPORT
Undisputedly, the United States’ health care sys-
tem is in the midst of unprecedented complexi-
ty and transformation. In 2014 alone there were
well over thirty-five million admissions to hospitals in
the nation,1 indicating that there was an extraordinary
number of very sick and frail people requiring highly
skilled clinicians to manage and coordinate their com-
plex care across multiple care settings. Medical advances
give us the ability to send patients home more efficiently
than ever before and simultaneously create ethical ques-
tions about the balance of benefits and burdens associ-
ated with these advances. New treatments for cancer or
complex heart disease may prolong life until the disease
becomes irreversible while causing significant morbidity
that undermines functional status, independence, and
quality of life in ways that patients find unacceptable.
Some patients and families voice concerns about access
to treatments and about the quality and safety of the care
they or their loved ones receive.
Every day on every shift, nurses at the bedside feel
these pressures and the intense array of ethical issues that
they raise. A staggering 17.5 percent of trained nurses are
leaving their roles or the profession after less than one
year of service,2 and increasing levels of moral distress
and burnout contribute to their decisions.3 Meanwhile,
research supports the common-sense understanding that
patients and health care organizations fare better when
nurses are not harried, are supported in their work en-
vironments, and are able to practice high-quality, ethical
care.
At the same time, administrators, policy-makers, and
regulators struggle to balance commitments to patients,
families, staff members, and governing boards. Health
care organizations are compelled by laws, regulations,
and accrediting bodies to pursue externally reported
measures of effectiveness that can put their mission and
values at risk. While health care systems declare their
commitment to core ethical values, many clinicians
struggle to understand institutional priorities, budgets,
policies, and decisions seemingly inconsistent with their
values as professionals.
Increasingly clinicians find their ability to provide
compassionate care at odds with the intensifying focus
on matters such as clinical pathways aimed at standard-
izing care, cost-cutting efficiencies, electronic medical
records, and hospital policies and procedures.4 Arguably,
each of these have merit in the current system, but what
is not accounted for are the unintended consequences
of diverting attention from the core ethical values of the
professions. For example, the advent of the EMR requires
clinicians to focus on documentation rather than being
fully present during patient encounters. An emphasis on
clinical pathways increases the risk of reducing patient
symptoms and diseases to what fits a rote app.
How can population health change the face of healthcare and predictive medicine? Understanding patient ailments in a new wave to help doctors and physicians build trust in software and in advanced means of healthcare.
Leanne Wells, Chief Executive Officer, Consumers Health Forum of Australia, gave the Ian Webster Health for All Oration to the annual forum of the Centre for Primary Health Care and Equity on 13 August 2015.
3.1 INTRODUCTION
When the health community makes reference to patients having access to care, the reference is
generally limited. The concept of access is too often described as individuals getting to and from
health services and having the ability to pay for the services either by virtue of a third party or
out-of-pocket. We believe access to be much more than this and suggest that a redefinition of
access is long overdue. True access means being able to get to and from health services, having the
ability to pay for the services needed, and getting your needs met once you enter the health system.
This text introduces a framework for assessing the strengths and weaknesses of selective healthcare
systems, and determining if the system is providing true access to health care. The framework is
called “The Eight Factor Model.”
The comparison of health systems is made by utilizing The Eight Factor Model, which was
developed by the authors, and has “true access” as the driving value. As illustrated in Figure 3-1 ,
the model has true access at its core, and eight surrounding factors that are important for health
systems to demonstrate in order to provide that true access. A solid directional arrow from the
factor to the core depicts a system that has demonstrated evidence to support that it is providing
true access. A broken directional arrow from the core to the factor suggests the system is not
providing true access, and much work must be done to achieve it. Table 3-1 (a format for assessing
true access) provides a template for learners to formulate their own opinions about the extent to
which countries discussed in this text provide true access. Table 7 in Chapter 16 , The Eight Factor
Model for True Access, summarizes author observations regarding the extent to which each of the
11 countries discussed in the “Health Care in Industrialized (Developed) Countries and “Health
Care in Developing Countries” sections of this text have addressed true access. This will hopefully
enable the learner to briefly review it against the Eight Factor Model illustrated in Figure 3-1 . Table
7, The Eight Factor Model for True Access, which appears at the end of Chapter 16 (Comparative
health perspectives) should be fully reviewed as the l ...
The role of health information managers in the healthcare delivery systemResearchWap
The study was an “The Role of Health Information Managers in Healthcare Delivery System (A Case Study of University of Uyo Health Centre. Uyo, Akwa Ibom State). The main objective of the study was to access the academic and knowledge level of Health information managers in their practice, while specific objective are: To assess the strength of Health Information managers in academic level. To verify factors affecting the efficiency of health information managers in the hospital. To examine the availability of equipment for effective and efficient functioning of health information management staff in their practice. Related literature were reviewed base on several authors which worked into 16 sub-topics related to the role of health information managers. Descriptive survey design was adopted and 110 respondents were selected using purposive sampling to chores 20 health information management staff from unit and 90 other staff from the health centre. The finding showed that 74.5% of the respondents accepted that, the higher the health information managers academic level, the more they gained knowledge while their practice gives them experience to understand the study also revealed that inadequate storage space and equipment for killing patients records are the factors affecting the efficiency of health information managers in the health centre. While 26.5% disagree. The researcher recommended that hospital management should try to address the problems that affect health information management for them to function effectively and efficiency in the health centre. However, the researcher also found it necessary for further studies to be extended to other hospital
Heritage Healthcare:-
Legacy healthcare refers to the traditional model of healthcare that has been in vogue for many years. It is characterized by a fee-for-service payment model, where healthcare providers are reimbursed for each service they provide to patients. This model has been a foundation of the US healthcare system for many years, but it has faced increasing criticism for its high costs and inefficiencies. In this essay, we'll explore the history, challenges, and possible solutions to legacy healthcare.
History of Legacy Healthcare
Legacy healthcare emerged in the United States in the early 20th century. At the time, health care was largely provided by individual physicians and hospitals, and patients paid for services out of pocket. However, with the rise of employer-sponsored health insurance during World War II, a new payment model emerged. This model was based on a fee-for-service system, where healthcare providers were reimbursed for each service they provided to patients. The system was designed to encourage healthcare providers to provide more services, with the assumption that more services would lead to better health outcomes.
Over the past few years, the fee-for-service model has become deeply ingrained in the US healthcare system. It has been the foundation of the Medicare and Medicaid programs, which provide healthcare for millions of Americans. However, as the cost of health care continues to rise, the limits of this model are becoming increasingly apparent.
Challenges of Legacy Healthcare
One of the main challenges of legacy healthcare is its high cost. The fee-for-service model incentivizes healthcare providers to provide more services, whether those services are truly needed or not. This has given rise to a phenomenon known as overuse, where patients receive more tests, procedures and treatments than they actually need. This not only increases the cost of health care but can also cause harm to patients. For example, unnecessary tests and procedures can expose patients to radiation and other risks.
Another challenge of legacy healthcare is its fragmentation. The fee-for-service model encourages healthcare providers to work independently of each other, rather than collaborating to provide coordinated care. This can lead to a lack of communication between healthcare providers, resulting in duplication of services and missed opportunities to meet the health needs of patients. Fragmentation also makes it difficult for patients to navigate the health care system, as they may need to see multiple providers for different health problems.
Finally, legacy health care is often criticized for its lack of focus on prevention and population health. The fee-for-service model incentivizes healthcare providers to treat serious illnesses and injuries instead of addressing the underlying causes of poor health. more details
doctors and nurses can be differentiated in an effortless manner. Doctors study and cure disease, while nurses study and heal people. Too know more visit: https://at.tumblr.com/medicalsaffairsusa/what-can-nurses-do-that-doctors-cannot/31c42h37gaen
THIS IS THE FEEDBACK I RECEEIVED. Only one patient responded to my.docxjuliennehar
THIS IS THE FEEDBACK I RECEEIVED. Only one patient responded to my post. Hope this helps
Ryan,
Inadequate levels of nursing professionals were first discussed more than 80 years ago (Whelan, n.d.). Recently, scholars have opined many reasons for the shortage of nurses. Factors such as work stress, burnout, violence against healthcare professionals, a lack of qualified nursing instructors, and nurses unable to adapt to changing technology or clinical environments have been addressed (Haddad & Toney-Butler, 2019). As many nurses may attest, doing more with less can lead to mistakes and dissatisfaction with a nursing career. Ultimately, patient care suffers.
Organizations employ various tactics to help strengthen nurse retention. Halter et al. (2017) suggest strong nursing leadership and assigning preceptors to new nurses can help minimize nursing resignation rates. At the writer’s employment, hospital administrators use several ways to retain nurses. Each quarter, a nurse is recognized for outstanding achievement by receiving a certificate, gift card, and editorial mention on the hospital’s intranet. Moreover, the hospital caters lunch for all employees, dayside and nighttime staff, twice a year for meeting quality targets. Also, the hospital uses various national celebration days such as ice cream, donuts, coffee, bagels, and candy to reward all employees. Creating a level of goodwill and institutional collaboration can help retain nurses and improve job satisfaction (Kurnat-Thoma et al., 2017).
Reference
Haddad, L.M., & Toney-Butler, T.J. (2019). Nursing shortage. StatPearls Publishing.
Halter, M., Pelone, F., Boiko, O., Beighton, C., Harris, R., Gale, J., Gourlay, S., & Drennan, V. (2017). Interventions to reduce adult nursing turnover: A systematic review of systematic reviews. The Open Nursing Journal, 11, 108-123. https://doi.org/10.2174/1874434601711010108
Kurnat-Thoma, E., Ganger, M., Peterson, K., & Channell, L. (2017). Reducing annual hospital and registered nurse staff turnover: A 10-element onboarding program intervention. SAGE Open Nursing, 3. https://doi.org/10.1177/2377960817697712
Whelan, J.C. (n.d.). Where did all the nurses go? Retrieved from https://www.nursing.upenn.edu/nhhc/workforce-issues/where-did-all-the-nurses-go/
By Thomas C. Ricketts and Erin P. Fraher
Reconfiguring Health Workforce
Policy So That Education,
Training, And Actual Delivery
Of Care Are Closely Connected
ABSTRACT There is growing consensus that the health care workforce in
the United States needs to be reconfigured to meet the needs of a health
care system that is being rapidly and permanently redesigned.
Accountable care organizations and patient-centered medical homes, for
instance, will greatly alter the mix of caregivers needed and create new
roles for existing health care workers. The focus of health system
innovation, however, has largely been on reorganizing care delivery
processes, reengineering workflows, and adopting electronic technolo ...
Changing scenario needs an ever changing rational approach to healthcare terms and services.Where "tools"[your knowledge,interpretations,etc] helps you to make the picture better.
How do we see the healthcare's digital future and its impact on our lives?Jane Vita
"Healthcare is undergoing major changes spurred on by, but not limited to, technology.
Digitalisation is changing the way we think about health, what taking care of it really entails, our personal role in healthcare systems and the way we interact with technology in the context of health.
In many ways, we are entering a post-institutional age of increased personal responsibility, which presents healthcare service providers and other players in the field with major opportunities and great risks. Technology has the potential to empower people and help them become more active in the management of their and their families’ health. This will change the relationship of the patient and the caregiver in profound ways." Mirkka Länsisalo
A co-creation with Mirkka Läansisalo and Sala Heinänen, at Futurice.
Healthcare is undergoing major changes spurred on by, but not limited to, technology.
Digitalisation is changing the way we think about health, what taking care of it really entails, our personal role in healthcare systems and the way we interact with technology in the context of health.
In many ways, we are entering a post- institutional age of increased personal responsibility, which presents healthcare service providers and other players in the eld with major opportunities and great risks. Technology has the potential to empower people and help them become more active in the management of their and their families’ health. This will change the relationship of the patient and the caregiver in profound ways.
(No Plagiarism) Explain the statement Although many leading organi.docxtamicawaysmith
(No Plagiarism) Explain the statement: "Although many leading organizations have invested significant resources in developing the culture and routines for this innovation processes, most organizations continue to rely on the efforts of a handful of people and chance. An innovative organization is one that can perfect these routines in addition to creating an innovation culture in the organization that engages people. Five key routines can facilitate its management of the innovation process” (Dooley & O'Sullivan, 2003).
.
What made you choose this career path What advice do you hav.docxtamicawaysmith
What made you choose this career path?
What advice do you have for those hoping to enter this career path?
What were some obstacles you faced upon graduating from college?
Does your career require graduate school? What programs would be acceptable?
Is there anything you wish you would have done differently?
Is it difficult to find a job in this area?
What is a typical work week like?
Etcetera, depending on the field and what you’re interested in.
.
Patient Population The student will describe the patient populati.docxtamicawaysmith
Patient Population: The student will describe the patient population that is impacted by the clinical issue. With a focus on the diversity of the human condition found within this patient population, the student will describe the influence that cultural values may have on the proposed solution. Proposed
Solution
: The student will set the stage for proposing the best solution to the clinical problem by using appropriate evidence-based data and integrating data from peer-reviewed journal articles. In this paper, the student will: i. Propose a clear solution to the clinical problem that is supported by a minimum of three scholarly, peer-reviewed journal articles.ii. Expand on the ethical considerations when developing the plan.
.
Dr. Paul Murray Bessie Coleman Jean-Bapiste Bell.docxtamicawaysmith
Dr. Paul Murray
Bessie Coleman
Jean-Bapiste Belley
Harriet Elizabeth Brown
Monte Irvin
Shirley Graham Dubois
Vernon Dahmer
Hale Woodruff
Jo Ann Robinson
Eugene "Pineapple" Jackson
Dr. Francis Cress Welsing
Dr. Kenneth Clark
Amy Jacques Garvey
Ophelia DeVore
Augusta Fells Savage
Eugene Jacques Bullard
Bobby Timmons
Clyde Kennard
Madison Washington
Joseph Winters
Sam Sharpe
Joseph Rainey
Bessie Stringfield
DJ Kool Herc
Lonnie Clayton
Mrs. Mamie Lang Kirkland
Lucius Septimius Bassianus
Carolyn Gudger
Jasmine Twitty
Daisy Bates
Ella Jenkins
Lewis Henry Douglass
Cynthia Robinson
Sylvester Magee
Mabel Fairbanks
Cathay Williams
Clara Belle Williams
John Baxter Taylor Jr.
Anna J. Cooper
The Black Seminoles
Dr. Daniel Hale Williams
Matthew Williams
Phillipa Schuyler
Yarrow Mamout
Mamie "Peanut" Johnson
Frank E. Petersen
"Miss Maggie" Walker
Paul Robeson
Olivia J. Hooker
Dr. Henry T Sampson
Lovie Yancy
Willie James Howard
Toni Stone (Marcenia Lyle Alberga)
Lucien Victor Alexis
Mevinia Sheilds
Dr. Lonnie Smith
Rosewood
Miss Jane Pittman
Lucy Terry
Abraham Galloway
Thomas Jennings
Irene Morgan
Paul Lawrence Dunbar
Jean Toomer
Doris Payne
Ann Petry
Madam C.J. Walker
Dr. May Edward Chinn
Greenwood, Tulsa, OK
Karen Bass
Dr. Dorothy Height
Dr. Geneva Smitherman
Michaëlle Jean
Robin Kelly
Mary Macleod Bethune
Jane Bolin
Donna Edwards
Dame Eugenia Charles
Dr. Thomas Elkins
Wilma Rudolph
Annie Malone
Ann Lowe
Black Wall Street
Cathy Hughes
Kamala Harris
Fannie Lou Hamer
Sarah Rector
Ruth Simmons
Claudette Colvin
MC Lyte
Benajin Banneker
Benjamin O. Davis, Jr.
Thurgood Marshall
Doris "Dorie" Miller
Cecil Noble
WC Handy
Dorothy Counts
Bayard Rustin
Dr. Eliza Ann Grier
Matthew Henson
Jesse Owens
Nina Simone
Wendell Scott
Adam Clayton Powell
Percy Julian
Dr. Charles Drew
Thomas "Fats" Waller
Satchel Paige
Bass Reeves
Marian Anderson
Josephine Baker
Joe Louis
Walter White
William Hastie
Elijah McCoy
Jan Matzelger
Lewis Latimer
Granville T. Woods
Fred Jones
Nella Larsen
Lloyd Hall
A. Philip Randolph
Althea Gibson
Barbara C. Jordon
Marcus Garvey
Malcolm X
James Meridith
Guy Buford
Hazel Scott
Stokely Carmichal
Denmark Vessey
Alex Haley
Virginia Hamilton
Ishmael Reed
Nalo Hopkinson
George Schuyler
Patricia Roberts Harris
John Lewis
Les McCann
Martin Delany
Derek Walcott
Carter Godwin Woodson
Alvin Ailey
Debbie Allen
Ralph Abernathy
Arthur Ashe
Crispus Attucks
Amiri Baraka
Seko.
More Related Content
Similar to 35NURSING ECONOMIC$January-February 2011Vol. 29No. 1T.docx
How can population health change the face of healthcare and predictive medicine? Understanding patient ailments in a new wave to help doctors and physicians build trust in software and in advanced means of healthcare.
Leanne Wells, Chief Executive Officer, Consumers Health Forum of Australia, gave the Ian Webster Health for All Oration to the annual forum of the Centre for Primary Health Care and Equity on 13 August 2015.
3.1 INTRODUCTION
When the health community makes reference to patients having access to care, the reference is
generally limited. The concept of access is too often described as individuals getting to and from
health services and having the ability to pay for the services either by virtue of a third party or
out-of-pocket. We believe access to be much more than this and suggest that a redefinition of
access is long overdue. True access means being able to get to and from health services, having the
ability to pay for the services needed, and getting your needs met once you enter the health system.
This text introduces a framework for assessing the strengths and weaknesses of selective healthcare
systems, and determining if the system is providing true access to health care. The framework is
called “The Eight Factor Model.”
The comparison of health systems is made by utilizing The Eight Factor Model, which was
developed by the authors, and has “true access” as the driving value. As illustrated in Figure 3-1 ,
the model has true access at its core, and eight surrounding factors that are important for health
systems to demonstrate in order to provide that true access. A solid directional arrow from the
factor to the core depicts a system that has demonstrated evidence to support that it is providing
true access. A broken directional arrow from the core to the factor suggests the system is not
providing true access, and much work must be done to achieve it. Table 3-1 (a format for assessing
true access) provides a template for learners to formulate their own opinions about the extent to
which countries discussed in this text provide true access. Table 7 in Chapter 16 , The Eight Factor
Model for True Access, summarizes author observations regarding the extent to which each of the
11 countries discussed in the “Health Care in Industrialized (Developed) Countries and “Health
Care in Developing Countries” sections of this text have addressed true access. This will hopefully
enable the learner to briefly review it against the Eight Factor Model illustrated in Figure 3-1 . Table
7, The Eight Factor Model for True Access, which appears at the end of Chapter 16 (Comparative
health perspectives) should be fully reviewed as the l ...
The role of health information managers in the healthcare delivery systemResearchWap
The study was an “The Role of Health Information Managers in Healthcare Delivery System (A Case Study of University of Uyo Health Centre. Uyo, Akwa Ibom State). The main objective of the study was to access the academic and knowledge level of Health information managers in their practice, while specific objective are: To assess the strength of Health Information managers in academic level. To verify factors affecting the efficiency of health information managers in the hospital. To examine the availability of equipment for effective and efficient functioning of health information management staff in their practice. Related literature were reviewed base on several authors which worked into 16 sub-topics related to the role of health information managers. Descriptive survey design was adopted and 110 respondents were selected using purposive sampling to chores 20 health information management staff from unit and 90 other staff from the health centre. The finding showed that 74.5% of the respondents accepted that, the higher the health information managers academic level, the more they gained knowledge while their practice gives them experience to understand the study also revealed that inadequate storage space and equipment for killing patients records are the factors affecting the efficiency of health information managers in the health centre. While 26.5% disagree. The researcher recommended that hospital management should try to address the problems that affect health information management for them to function effectively and efficiency in the health centre. However, the researcher also found it necessary for further studies to be extended to other hospital
Heritage Healthcare:-
Legacy healthcare refers to the traditional model of healthcare that has been in vogue for many years. It is characterized by a fee-for-service payment model, where healthcare providers are reimbursed for each service they provide to patients. This model has been a foundation of the US healthcare system for many years, but it has faced increasing criticism for its high costs and inefficiencies. In this essay, we'll explore the history, challenges, and possible solutions to legacy healthcare.
History of Legacy Healthcare
Legacy healthcare emerged in the United States in the early 20th century. At the time, health care was largely provided by individual physicians and hospitals, and patients paid for services out of pocket. However, with the rise of employer-sponsored health insurance during World War II, a new payment model emerged. This model was based on a fee-for-service system, where healthcare providers were reimbursed for each service they provided to patients. The system was designed to encourage healthcare providers to provide more services, with the assumption that more services would lead to better health outcomes.
Over the past few years, the fee-for-service model has become deeply ingrained in the US healthcare system. It has been the foundation of the Medicare and Medicaid programs, which provide healthcare for millions of Americans. However, as the cost of health care continues to rise, the limits of this model are becoming increasingly apparent.
Challenges of Legacy Healthcare
One of the main challenges of legacy healthcare is its high cost. The fee-for-service model incentivizes healthcare providers to provide more services, whether those services are truly needed or not. This has given rise to a phenomenon known as overuse, where patients receive more tests, procedures and treatments than they actually need. This not only increases the cost of health care but can also cause harm to patients. For example, unnecessary tests and procedures can expose patients to radiation and other risks.
Another challenge of legacy healthcare is its fragmentation. The fee-for-service model encourages healthcare providers to work independently of each other, rather than collaborating to provide coordinated care. This can lead to a lack of communication between healthcare providers, resulting in duplication of services and missed opportunities to meet the health needs of patients. Fragmentation also makes it difficult for patients to navigate the health care system, as they may need to see multiple providers for different health problems.
Finally, legacy health care is often criticized for its lack of focus on prevention and population health. The fee-for-service model incentivizes healthcare providers to treat serious illnesses and injuries instead of addressing the underlying causes of poor health. more details
doctors and nurses can be differentiated in an effortless manner. Doctors study and cure disease, while nurses study and heal people. Too know more visit: https://at.tumblr.com/medicalsaffairsusa/what-can-nurses-do-that-doctors-cannot/31c42h37gaen
THIS IS THE FEEDBACK I RECEEIVED. Only one patient responded to my.docxjuliennehar
THIS IS THE FEEDBACK I RECEEIVED. Only one patient responded to my post. Hope this helps
Ryan,
Inadequate levels of nursing professionals were first discussed more than 80 years ago (Whelan, n.d.). Recently, scholars have opined many reasons for the shortage of nurses. Factors such as work stress, burnout, violence against healthcare professionals, a lack of qualified nursing instructors, and nurses unable to adapt to changing technology or clinical environments have been addressed (Haddad & Toney-Butler, 2019). As many nurses may attest, doing more with less can lead to mistakes and dissatisfaction with a nursing career. Ultimately, patient care suffers.
Organizations employ various tactics to help strengthen nurse retention. Halter et al. (2017) suggest strong nursing leadership and assigning preceptors to new nurses can help minimize nursing resignation rates. At the writer’s employment, hospital administrators use several ways to retain nurses. Each quarter, a nurse is recognized for outstanding achievement by receiving a certificate, gift card, and editorial mention on the hospital’s intranet. Moreover, the hospital caters lunch for all employees, dayside and nighttime staff, twice a year for meeting quality targets. Also, the hospital uses various national celebration days such as ice cream, donuts, coffee, bagels, and candy to reward all employees. Creating a level of goodwill and institutional collaboration can help retain nurses and improve job satisfaction (Kurnat-Thoma et al., 2017).
Reference
Haddad, L.M., & Toney-Butler, T.J. (2019). Nursing shortage. StatPearls Publishing.
Halter, M., Pelone, F., Boiko, O., Beighton, C., Harris, R., Gale, J., Gourlay, S., & Drennan, V. (2017). Interventions to reduce adult nursing turnover: A systematic review of systematic reviews. The Open Nursing Journal, 11, 108-123. https://doi.org/10.2174/1874434601711010108
Kurnat-Thoma, E., Ganger, M., Peterson, K., & Channell, L. (2017). Reducing annual hospital and registered nurse staff turnover: A 10-element onboarding program intervention. SAGE Open Nursing, 3. https://doi.org/10.1177/2377960817697712
Whelan, J.C. (n.d.). Where did all the nurses go? Retrieved from https://www.nursing.upenn.edu/nhhc/workforce-issues/where-did-all-the-nurses-go/
By Thomas C. Ricketts and Erin P. Fraher
Reconfiguring Health Workforce
Policy So That Education,
Training, And Actual Delivery
Of Care Are Closely Connected
ABSTRACT There is growing consensus that the health care workforce in
the United States needs to be reconfigured to meet the needs of a health
care system that is being rapidly and permanently redesigned.
Accountable care organizations and patient-centered medical homes, for
instance, will greatly alter the mix of caregivers needed and create new
roles for existing health care workers. The focus of health system
innovation, however, has largely been on reorganizing care delivery
processes, reengineering workflows, and adopting electronic technolo ...
Changing scenario needs an ever changing rational approach to healthcare terms and services.Where "tools"[your knowledge,interpretations,etc] helps you to make the picture better.
How do we see the healthcare's digital future and its impact on our lives?Jane Vita
"Healthcare is undergoing major changes spurred on by, but not limited to, technology.
Digitalisation is changing the way we think about health, what taking care of it really entails, our personal role in healthcare systems and the way we interact with technology in the context of health.
In many ways, we are entering a post-institutional age of increased personal responsibility, which presents healthcare service providers and other players in the field with major opportunities and great risks. Technology has the potential to empower people and help them become more active in the management of their and their families’ health. This will change the relationship of the patient and the caregiver in profound ways." Mirkka Länsisalo
A co-creation with Mirkka Läansisalo and Sala Heinänen, at Futurice.
Healthcare is undergoing major changes spurred on by, but not limited to, technology.
Digitalisation is changing the way we think about health, what taking care of it really entails, our personal role in healthcare systems and the way we interact with technology in the context of health.
In many ways, we are entering a post- institutional age of increased personal responsibility, which presents healthcare service providers and other players in the eld with major opportunities and great risks. Technology has the potential to empower people and help them become more active in the management of their and their families’ health. This will change the relationship of the patient and the caregiver in profound ways.
(No Plagiarism) Explain the statement Although many leading organi.docxtamicawaysmith
(No Plagiarism) Explain the statement: "Although many leading organizations have invested significant resources in developing the culture and routines for this innovation processes, most organizations continue to rely on the efforts of a handful of people and chance. An innovative organization is one that can perfect these routines in addition to creating an innovation culture in the organization that engages people. Five key routines can facilitate its management of the innovation process” (Dooley & O'Sullivan, 2003).
.
What made you choose this career path What advice do you hav.docxtamicawaysmith
What made you choose this career path?
What advice do you have for those hoping to enter this career path?
What were some obstacles you faced upon graduating from college?
Does your career require graduate school? What programs would be acceptable?
Is there anything you wish you would have done differently?
Is it difficult to find a job in this area?
What is a typical work week like?
Etcetera, depending on the field and what you’re interested in.
.
Patient Population The student will describe the patient populati.docxtamicawaysmith
Patient Population: The student will describe the patient population that is impacted by the clinical issue. With a focus on the diversity of the human condition found within this patient population, the student will describe the influence that cultural values may have on the proposed solution. Proposed
Solution
: The student will set the stage for proposing the best solution to the clinical problem by using appropriate evidence-based data and integrating data from peer-reviewed journal articles. In this paper, the student will: i. Propose a clear solution to the clinical problem that is supported by a minimum of three scholarly, peer-reviewed journal articles.ii. Expand on the ethical considerations when developing the plan.
.
Dr. Paul Murray Bessie Coleman Jean-Bapiste Bell.docxtamicawaysmith
Dr. Paul Murray
Bessie Coleman
Jean-Bapiste Belley
Harriet Elizabeth Brown
Monte Irvin
Shirley Graham Dubois
Vernon Dahmer
Hale Woodruff
Jo Ann Robinson
Eugene "Pineapple" Jackson
Dr. Francis Cress Welsing
Dr. Kenneth Clark
Amy Jacques Garvey
Ophelia DeVore
Augusta Fells Savage
Eugene Jacques Bullard
Bobby Timmons
Clyde Kennard
Madison Washington
Joseph Winters
Sam Sharpe
Joseph Rainey
Bessie Stringfield
DJ Kool Herc
Lonnie Clayton
Mrs. Mamie Lang Kirkland
Lucius Septimius Bassianus
Carolyn Gudger
Jasmine Twitty
Daisy Bates
Ella Jenkins
Lewis Henry Douglass
Cynthia Robinson
Sylvester Magee
Mabel Fairbanks
Cathay Williams
Clara Belle Williams
John Baxter Taylor Jr.
Anna J. Cooper
The Black Seminoles
Dr. Daniel Hale Williams
Matthew Williams
Phillipa Schuyler
Yarrow Mamout
Mamie "Peanut" Johnson
Frank E. Petersen
"Miss Maggie" Walker
Paul Robeson
Olivia J. Hooker
Dr. Henry T Sampson
Lovie Yancy
Willie James Howard
Toni Stone (Marcenia Lyle Alberga)
Lucien Victor Alexis
Mevinia Sheilds
Dr. Lonnie Smith
Rosewood
Miss Jane Pittman
Lucy Terry
Abraham Galloway
Thomas Jennings
Irene Morgan
Paul Lawrence Dunbar
Jean Toomer
Doris Payne
Ann Petry
Madam C.J. Walker
Dr. May Edward Chinn
Greenwood, Tulsa, OK
Karen Bass
Dr. Dorothy Height
Dr. Geneva Smitherman
Michaëlle Jean
Robin Kelly
Mary Macleod Bethune
Jane Bolin
Donna Edwards
Dame Eugenia Charles
Dr. Thomas Elkins
Wilma Rudolph
Annie Malone
Ann Lowe
Black Wall Street
Cathy Hughes
Kamala Harris
Fannie Lou Hamer
Sarah Rector
Ruth Simmons
Claudette Colvin
MC Lyte
Benajin Banneker
Benjamin O. Davis, Jr.
Thurgood Marshall
Doris "Dorie" Miller
Cecil Noble
WC Handy
Dorothy Counts
Bayard Rustin
Dr. Eliza Ann Grier
Matthew Henson
Jesse Owens
Nina Simone
Wendell Scott
Adam Clayton Powell
Percy Julian
Dr. Charles Drew
Thomas "Fats" Waller
Satchel Paige
Bass Reeves
Marian Anderson
Josephine Baker
Joe Louis
Walter White
William Hastie
Elijah McCoy
Jan Matzelger
Lewis Latimer
Granville T. Woods
Fred Jones
Nella Larsen
Lloyd Hall
A. Philip Randolph
Althea Gibson
Barbara C. Jordon
Marcus Garvey
Malcolm X
James Meridith
Guy Buford
Hazel Scott
Stokely Carmichal
Denmark Vessey
Alex Haley
Virginia Hamilton
Ishmael Reed
Nalo Hopkinson
George Schuyler
Patricia Roberts Harris
John Lewis
Les McCann
Martin Delany
Derek Walcott
Carter Godwin Woodson
Alvin Ailey
Debbie Allen
Ralph Abernathy
Arthur Ashe
Crispus Attucks
Amiri Baraka
Seko.
In depth analysis of your physical fitness progress Term p.docxtamicawaysmith
In depth analysis of your physical fitness progress
Term paper should include details of:
▪ What worked and why (include all documentation)
▪ What didn’t and why
▪ Are your physical fitness results in alignment with your health continuum goals (include documentation)
▪ What are your current goals
▪ What are your future goals
▪ Develop a road map to get achieve those goals Due no later than November 30, 2020.
samples
Physical fitness benchmark assessments
Fitness assessment data sheet
Exercise charts
Personal physical fitness progress chart
Self assessment: Individual Health Continuum
.
Information systems infrastructure evolution and trends Str.docxtamicawaysmith
Information systems infrastructure: evolution and trends
Strategic importance of cloud computing in business organizations
Big data and its business impacts
Managerial issues of a networked organization
Emerging enterprise network applications
Mobile computing and its business implications
Instructions:
9- 10 pages (does not include Title page and references )
can Include images (not more than two)
Minimum six (6) sources – at least two (2) from peer reviewed journals
Include an abstract, introduction, and conclusion
.
⦁One to two paragraph brief summary of the book. ⦁Who is the.docxtamicawaysmith
⦁One to two paragraph brief summary of the book.
⦁Who is the author and his/her background?
⦁Does the author have any particular ideological viewpoint that he or she is trying to advance or do you consider the author to have been neutral and presented both sides of controversial issues? (You will find asking this same question will help you in other courses and your future career.)
⦁When was this book written? Does the author reflect the views (biases) of the time when the book was written? Why or why not?
⦁What did you find most interesting in the book? Least interesting?
⦁What additional topics should the author have included in the book? Why?
⦁How had people before the age of the telegraph attempted to communicate faster over distances?
⦁How did the telegraph reflect scientific and technological developments, both in the United States and other countries?
⦁Why did the telegraph represent such a revolutionary development and not just an incremental improvement in communication?
⦁How did the telegraph impact politics, journalism, business, military strategy and society in general?
⦁How were the American and European experiences similar or different in developing the telegraph? Did the telegraph have a similar impact in the United States and Europe?
⦁What do you think of the author’s title? Is the Victorian-era telegraph really the equivalent of today’s internet in terms of its impact or is that an exaggeration? Why or why not?
⦁Do you think the author makes the material interesting, understandable and relevant to the general public? Why or why not?
⦁If you were the editor in the publishing company, what changes would you make to the author’s draft?
⦁Did the book increase your interest in a particular issue that you would like to learn more about?
⦁Do you think it is worthwhile learn about the historical impact of scientific and technological developments?
⦁Would you recommend this book to a friend? Why or why not?
⦁Would you recommend that I continue to use this book in this course with future students?
.
100.0 Criteria10.0 Part 1 PLAAFP The PLAAFP thoroughly an.docxtamicawaysmith
100.0 %Criteria
10.0 %Part 1: PLAAFP
The PLAAFP thoroughly and adeptly incorporates student's academic strengths, evaluations, performance in classes, and any other relevant issues.
10.0 %Part 2: Present Levels for Transition COE 3.8 [CEC 5.1, ICSI.5.S8, ICSI.5.S15, IGC.5.K1, IGC.5.S7, IGC.5.S23, IGC.5.S24; InTASC 1(b), 2(d), 5(f), 6(v), 8(s), 9(h); MC2, MC3, MC4, MC5]
Preferential learning environment, strengths and interests relating to the transition, and areas in need of improvement for transition are substantially described.
15.0 %Part 2: Transition Plan COE: 3.10 [CEC 5.5, ICSI.5.S8, ICSI.5.S8, ICSI.5.S15, ICSI.5.S17, ICSI.5.S19, IGC.5.K1, IGC.5.K3, IGC.5.K8, IGC.5.S1, IGC.5.S2, IGC.5.S11 IGC.5.S23, IGC.5.S24; InTASC 7(b), 7(e); MC1, MC2, MC4, MC5]
The transition plan demonstrates best practices in identifying proficient, measureable transition plan goals that are aligned with student's interests and present levels. Also includes quality aligned activities/services, persons/agency involved and realistic expected dates of achievement.
10.0 %Part 3: Rationale - Justification COE: 5.1 [ACEI 5.0; CEC 6.1, ICSI.6.K2, ICSI.6.K4 ICSI.6.S1, ICSI.6.S2, ICSI.6.S3, ICSI.6.S4, ICSI.6.S5, ICSI.6.S7, IGC.6.K4, IGC.6.K6, IGC.6.S2; InTASC 9(l), 9(o); MC2, MC3, MC4]
Rationale skillfully justifies content and decisions displayed in PLAAFP, annual goals, and transition plan, convincingly demonstrating how they meet the needs of the student. Claims are fully grounded in CEC Code of Ethics.
15.0 %Part 4: Rationale - Confidentiality COE: 5.8 [CEC 6.1, ICSI.6.S1, ICSI.6.S2, ICSI.6.S4, ICSI.7.S1, IGC.6.K1, IGC.6.K6; InTASC 5(k); MC1, MC2, MC4, MC5]
The rationale thoroughly defends the legal, ethical, and quality requirements related to the management of confidential student information.
10.0 %Reflection COE: 5.4 [CEC 6.2, ICSI.6.S1, ICSI.6.S2, ICSI.6.S4, IGC.6.K1, IGC.6.K2, IGC.6.K3; InTASC 10(h); MC1, MC2, MC4; COE 5.4]
Reflection convincingly relates how foundational knowledge developed relating to providing professional, ethical and legal educational services will be used in future professional practice.
5.0 %Research
Research strongly supports the information presented. Sources are timely, distinctive and clearly address all of the criteria stated in the assignment.
10.0 %Organization
The content is well-organized and logical. There is a sequential progression of ideas that relate to each other. The content is presented as a cohesive unit and provides the audience with a clear sense of the main idea.
10.0 %Mechanics of Writing (includes spelling, punctuation, grammar, language use)
Submission is virtually free of mechanical errors. Word choice reflects well-developed use of practice and content-related language. Sentence structures are varied and engaging.
5.0 %Documentation of Sources (citations, footnotes, references, bibliography, etc., as appropriate to assignment and style)
Sources are documented completely and correctly, as appropria.
102120151De-Myth-tifying Grading in Sp.docxtamicawaysmith
10/21/2015
1
De-Myth-tifying Grading
in Special Education
1980 2015
10/21/2015
2
Primary Purpose
• “the primary purpose of…grades…
(is) to communicate student
achievement to students, parents,
school administrators,
post-secondary institutions and
employers.” and
• To provide teachers with information
for instructional planning.
Taken from “Reporting Achievement at the Secondary School Level: What and How?”, in Communicating Student
Learning: ASCD Yearbook 1996, p. 120.
What makes grading so
hard?
• Teacher preparation programs seldom include course work or
even discussions of recommended practices for grading
students in general, much less for students who may be
struggling learners. As a result, teachers at all grade levels
grapple with issues of fairness in grading.
• Despite the magnitude of this problem, few recommendations
for grading struggling learners can be found in the research
literature or in education policy.
• Urban Grading Legends
10/21/2015
3
Urban Legends:
Bigfoot/Sasquatch
Urban Legends
• I can’t fail a special education
student.
• I give all my Life Skills students an
85.
• The report card grade does not really
mean anything.
10/21/2015
4
Urban Legends
• The grade on the report card can’t be less
than the IEP mastery level (default 70%)
• I teach a lot in my classroom, but I can
only grade the things that are on the IEP.
• I don’t do the grades for my special
education students in my classroom, the
special education teacher does that for
me.
What’s the
problem??
• Some students are not getting REAL
grades.
• Multiple court cases regarding failing
students who are not receiving
appropriate specially designed instruction
or students only get “A’s” and it doesn’t
truly reflect how he/she really performs in
relation to the curriculum
10/21/2015
5
What does the law really
say?
• Neither the Individuals with Disabilities Education Act
(IDEA) nor any other federal education laws contain
requirements for grading. Therefore, each state has
discretion on the issue.
• The TEC is the set of state laws our state legislators have
passed that relate to education. ARD committees do not
have the authority to override state laws. The Texas
Administrative Code (TAC) is the set of rules that the State
Legislature has authorized Texas Education Agency (TEA)
or the State Board to write. ARD committees must also
follow these rules.
• The state statutes apply to all public school students in
Texas regardless of special education eligibility.
Local Grading Policies
TEC §28.0216
(1) “must require a classroom teacher to assign a grade that
reflects the students’ relative mastery of an assignment;
[and]
(2) may not require a classroom teacher to assign a
minimum grade for an assignment without regard to the
student’s quality of work.”
(3) may allow a student a reasonable opportunity to make up
or redo a class .
100.0 %Criteria
30.0 %Flowchart Content
The flowchart skillfully depicts the two possible discipline paths following the manifestation determination. In addition, there are two comprehensively aligned IEP goals for each determination.
40.0 %Legal Issues Analysis
A compelling analysis is included regarding any legal issues raised by the change in Carrie's transportation, proficiently incorporating relevant statutes, regulations, and case decisions.
5.0 %Research
Research strongly supports the information presented. Sources are timely, distinctive and clearly address all of the criteria stated in the assignment.
5.0 %Rationale Organization
The content is well organized and logical. There is a sequential progression of ideas related to each other. The content is presented as a cohesive unit and the audience is provided with a clear sense of the main idea.
5.0 %Overall Flowchart Presentation
The work is well presented. The overall appearance is neat and professional. Work would be highly desirable for public dissemination.
10.0 %Mechanics of Writing (includes spelling, punctuation, grammar, language use)
Submission is virtually free of mechanical errors. Word choice reflects well-developed use of practice and content-related language. Sentence structures are varied and engaging.
5.0 %Documentation of Sources (citations, footnotes, references, bibliography, etc., as appropriate to assignment and style)
Sources are documented completely and correctly, as appropriate to assignment and style, and format is free of error.
100 %Total Weightage
.
100 words agree or disagree to eac questions Q 1.As her .docxtamicawaysmith
100 words agree or disagree to eac questions
Q 1.
As her defense attorney, I will argue that the officer did not only not read Sally's Miranda rights; he also did not respect her right to consul. After Sally made her allegedly verbal utterance, the Officer should have known to read Sally her rights. I will bring up that during New Jersey v. James P. Kucinski, Oct 26, 2016, the defendant was arrested for the bludgeoning death of his brother. The defendant was taken to police headquarters for questioning after the defendant was advised of his Miranda rights; he requested an attorney. The law enforcement officers terminated the interrogation, spoked with their supervisor, and approximately eight minutes later, the officers returned into the room and advised the defendant that he was being charged with murder. The scare tactic worked, and the defendant asked to speak with the officers. The defendant reluctantly answered a series of questions. Before trial, the defendant moved for suppression motion because the officers did not honor his request for counsel. The court denied the motion, during further questioning the defendant claimed to have acted in self-defense, the defense counsel moved for a mistrial. The trial court denied the motion for mistrial but instructed the jury that the defendant's right to remain silent should be limited to assessing his credibility. The defendant was charged with first-degree murder and third-degree possession of a weapon for unlawful purposes The Appellate Division reversed the defendant's conviction and motion for a new trial due to the prosecutor's question doing cross-examination was improper. The panel concluded that the defendant invoked his right to remain silent by telling law enforcement officers that he did not want to talk or answer questions. The Appellate Division found that the trial court instructions to the jury were flaws, and the supreme court agreed and affirmed. The officers should have stopped all questioning and contacted the defendant's attorney.
New Jersey v. Kucinski (2017). https://law.justia.com/cases/new-jersey/supreme-court/2017/a-58-15.html
Q 2.
My last name begins with a K. so I am answering in the role of prosecutor. Sally was originally pulled over because she had shown probable cause of drunk driving. Upon her traffic stop, Sally was then searched after being arrested and the handgun and drugs were found on her body. The police asked about the two items but did not “interrogate” her. Sally voluntarily answered the arresting officers’ questions and in doing so piled new charges onto her initial arrest charge. I believe that the judge will deny the request to suppress the admission of Sally’s statements. Sally does have rights under the Fifth Amendment, but her statements to the police officers were not coerced out of her. The Cornell Law School website states that the Fifth Amendment, under the self-incrimination clause, if an individual makes a spo.
101118, 4(36 PMCollection – MSA 603 Strategic Planning for t.docxtamicawaysmith
10/11/18, 4(36 PMCollection – MSA 603 Strategic Planning for the Admin ...
Page 1 of 1https://blackboard.cmich.edu/webapps/discussionboard/do/message?ac…_146240_1&nav=discussion_board_entry&isSearch=N&requestType=print
Collection
Users can Collect posts into a printable, sortable format. Collections are a good way to organize posts for quick
reading. A Collection must be created to tag posts. More Help
Thread: dis 4
Post: dis 4
Author:
Posted Date: October 9, 2018 8:50 PM
Status: Published
Overall Rating:
Tags: None
(Post is Read)
Brian Mcleod
I would say that for them to move the work and still be ethical defensible are work conditions,
respect for labor laws of the parent company, and job opportunities for the long-term
employees.
To expand on this would be the work conditions. The conditions that the workers have to work
under should be the same conditions that workers in the US have to work under. This involves
safety and environmental protection for the workers.
Labor laws of the host country and “most” of the internally recognized laws must be observed.
Overtime and child labor are a couple of items.
The long-term employees should be given the opportunity to move to another US based plant if
possible or to the new country.
Sometimes because of the state of the industry companies do have to make these decisions or
face possible bankruptcy. This alternative may not be the perfect solution but better than
bankrupting a company that still has operation in the US.
← OK
�
https://blackboard.cmich.edu/webapps/discussionboard/do/message?action=collectPrint&conf_id=_248584_1&forum_id=_382697_1&course_id=_146240_1&nav=discussion_board_entry&isSearch=N&requestType=print#
javascript:self.close()
10/11/18, 4(38 PMCollection – MSA 603 Strategic Planning for the Admin ...
Page 1 of 1https://blackboard.cmich.edu/webapps/discussionboard/do/message?ac…_146240_1&nav=discussion_board_entry&isSearch=N&requestType=print
Collection
Users can Collect posts into a printable, sortable format. Collections are a good way to organize posts for quick
reading. A Collection must be created to tag posts. More Help
Thread: DB4
Post: DB4
Author:
Posted Date: October 10, 2018 8:51 PM
Status: Published
Overall Rating:
Tags: None
(Post is Read)
Christina Lacroix
It is ethically defensible to outsource production when the outcome of not outsourcing
would negatively impact stakeholders. Organizations define their most important
stakeholders, often the shareholders, as they invested capital. While some risk is
assumed by shareholders as a fiduciary managers have an obligation to the
shareholders to protect their interest when possible. A company risks shareholder
investment (access to capital) and jeopardizes all other stakeholders such as
employees, suppliers, and creditors. An organization cannot risk itself and the other
stakeholders depending upon in order to save employees.
The organization should do its due diligence in securing its outso.
100 words per question, no references needed or quotations. Only a g.docxtamicawaysmith
100 words per question, no references needed or quotations. Only a general idea or opinion.
A.
· Compare and contrast two works from the Italian Baroque period with two works from the Renaissance. Be sure to note the appearance in the works of the defining characteristics from each period.
· Discuss why artistic expression shifted from the restrained stoicism of the Renaissance to that of the heightened emotion in the religious and other works of the Baroque.
B. From video
Goya -
The Third of May
- If you cannot see this video, click here -
https://youtu.be/e7piV4ocukg
Respond in writing to the following questions after reading Chapter 12, watching the video, and exploring the sites above.
1. Heroism, nationalism, and passion are themes associated with Romanticism. Which
three
landmarks of the nineteenth century are most representative of these themes? You can discuss art, philosophy, or literature.
2. Compare Neoclassicism and Romanticism as styles and sensibilities. What do their differences reflect about patronage, popular taste, and historical change? Provide specific examples from the chapters.
C.
1. From the arts of West Africa, what are some characteristics of African cultural heritage?
2. How did their religious beliefs influence their art and music.
D.
Watch video below
Manet -
Déjeuner
sur
l’herbe -
If you cannot see this video, click
https://youtu.be/3xBGF8H3bQ4
1. Viewers of Manet’s
Déjeuner sur l’herbe
initially responded to its public display by attacking the canvas with their umbrellas. Why?
2. What kind of art has evoked a comparable response in our own time? Do some research online. Find a recent work of art that caused controversy. Summarize the reasons for the controversy and your reaction to it. Try not post the same article as someone else. (This board is not POST FIRST, so you will be able to see what others have posted right away.) If you can, attach a picture of the image you are describing to your posting.
E.
Watch the video below. If you cannot see the video, click here:
https://youtu.be/XyLNPumMMTs
George Braque, Violin and Pitcher, (1909)
•
Pablo Picasso, Guernica, (1937)
•
Marcel Duchamp, Nude Descending a Staircase, (1912)
Respond in writing to the following question after reading Chapter 14 in your text, watching the video above, viewing the Web Assignments, and the sites above.
1. Describe how they three have departed from styles such as symbolism and impressionism of the late nineteenth century.
F.
Take some time to reflect on all we have covered in this course. Then, respond in writing to the following question.
1. After your experience in this course, describe why you feel the humanities are important.
.
100A 2
2 4 4
5
1A 1034 5
1B 1000 10
1C 1100 1
1D 1123 20
1E 1210 5
20 10 10
7
1A 2180 20
1B 1283 20
1C 3629 5
1D 3649 3
1E 4051 15
1F 4211 1
1G 5318 5
100B 1
2 4 1
3
1A 2180 10
1B 1283 10
1C 3629 5
100C 2
0 0 0
3
1A 6774 5
1B 6869 5
1C 6879 2
0 0 0
4
1A 6774 2
1B 6869 5
1C 6879 1
1D 7555 10
100D 1
10 5 3
3
1A 2180 5
1B 3649 2
1C 4211 3
Self-care and Residency Reflection Paper Scoring Rubric -
Content
80 Points
Points Earned
Additional Comments:
All key elements of the assignment are covered in a substantive way.
Write a 700- to 1,050-word paper to reflect on your residency experience and outline your plan for self-care. Please use the self-care and residency reflection paper template posted in Student Materials for this assignment.
Consider the following questions when writing your reflection:
a) What have you learned about yourself during residency?
b) What have you learned about yourself as a counselor-in-training during residency?
c) What are aspects of residency that you enjoyed? Why did you enjoy these aspects?
d) What aspects of residency did you not enjoy? Why did you not enjoy these aspects?
e) What is counselor self-care? Why is it important? Include two separate in-text and end of work references.
f) What strategies for maintaining self-care did you try throughout this program? How can you implement these strategies?
g) How will you know when you are experiencing burnout? What can you do to prevent this?
The content is comprehensive, accurate, and /or persuasive.
The paper links theory to relevant examples of current experience and industry practice and uses the vocabulary of the theory correctly. This refers to the use of literary references. Generally you will need one separate literary reference for each main point (objective) of your paper.
Major points are stated clearly and are supported by specific details, examples, or analysis.
Organization / Development
35 Points
Points Earned
Additional Comments:
The paper has a structure that is clear, logical, and easy to follow.
The paper develops a central theme or idea, directed toward the appropriate audience.
The introduction provides sufficient background on the topic and previews major points.
The conclusion is logical, flows from the body of the paper, and reviews the major points.
Transitions between sentences/ paragraphs/sections aid in maintaining the flow of thought.
The tone is appropriate to the content and assignment.
Mechanics
35 Points
Points Earned
Additional Comments:
The paper, including the title page, reference page, tables, and appendices follow APA guidelines for format.
Citations of original works within the body of the paper follow APA guidelines.
The paper is laid out with effective use of headings, font styles, and white space.
Rules of grammar, usage, and punctuation are followed.
Sentences are complete, clear, concise, and varied.
Spelling is correct.
.
10122018Week 5 Required Reading and Supplementary Materials - .docxtamicawaysmith
10/12/2018
Week 5 Required Reading and Supplementary Materials - MGMT 670 9042 Strategic Management Capstone (2188)
https://learn.umuc.edu/d2l/le/content/333174/viewContent/13406413/View
/2
Required Readings:
From the UMUC library: (Note: You must search for these articles in the UMUC library. In the case of video links in the UMUC library, exact directions are given on how to find the video.)
Porter's Five-Forces model. (2009). In Encyclopedia of management (6th Ed., pp. 714-717).
From Other websites:
Evaluating the industry. (2012). In Mastering strategic management. Washington, DC: Saylor Academy. Retrieved from https://saylordotorg.github.io/text_mastering-strategic-management/s07-03-evaluating-the-industry.html
The impact of external and internal factors on strategy. (2016, 31 May). In Boundless Management. Retrieved from https://courses.lumenlearning.com/boundless-management/chapter/strategic-management/
Mapping strategic groups. (2012). In Mastering strategic management. Washington, DC: Saylor Academy. Retrieved from https://saylordotorg.github.io/text_mastering-strategic-management/s07-04-mapping-strategic-groups.html
The PESTEL and SCP frameworks. (2016, 26 May). In Boundless management. Retrieved from https://courses.lumenlearning.com/boundless-management/chapter/external-inputs-to-strategy/
The relationship between an organization and its environment. (2012). In Mastering strategic management. Washington, DC: Saylor Academy. Retrieved from https://saylordotorg.github.io/text_mastering-strategic-management/s07-01-the-relationship-between-an- or.html
Strategic group mapping. (2010, October 5). MBA lectures. Retrieved from http://mba-lectures.com/management/strategic- management/1000/strategic-group-mapping.html
Supplementary Materials:
From the UMUC library: (Note: You must search for these articles in the UMUC library. In the case of video links in the UMUC library, exact directions are given on how to find the video.)
Anand, B. N. (2006). Crafting business strategy and environmental scanning [Video]. Harvard Business School Faculty Seminar Series.
Follow these steps to find this video:
Go to http://sites.umuc.edu/library/index.cfm
Type in the entire name of the article: "Crafting business strategy and environmental scanning," into the search box and click on "search."
Click on "multimedia" in the upper left hand corner of the webpage (under "Ask a Librarian.)
Type in the entire name of the article: "Crafting business strategy and environmental scanning," in the box at the top of the page to the left of the word, "Search."
Make sure only "Business Videos" and "Find all my search term" are the only boxes that are checked. Uncheck both "Image Collection" and "Apply equivalent
subjects"
Click on "Search" at the bottom right hand corner of the webpage. It is a small word in a box. The next page shows the article. Click on the article.
Dahab, S. (2008). Five forces. In S. R. Clegg & J. R. Bailey (Eds.), International en.
101416 526 PMAfter September 11 Our State of Exception by .docxtamicawaysmith
10/14/16 5:26 PMAfter September 11: Our State of Exception by Mark Danner | The New York Review of Books
Page 1 of 11http://www.nybooks.com/articles/2011/10/13/after-september-11-our-state-exception/?printpage=true
After September 11: Our State of Exception
Mark Danner OCTOBER 13, 2011 ISSUE
We are in a fight for our principles, and our first responsibility is to live by them.
—George W. Bush, September 20, 2001
1.
We are living in the State of Exception. We don’t know when it will end, as we don’t know when the War on Terror will
end. But we all know when it began. We can no longer quite “remember” that moment, for the images have long since
been refitted into a present-day fable of innocence and apocalypse: the perfect blue of that late summer sky stained by acrid
black smoke. The jetliner appearing, tilting, then disappearing into the skin of the second tower, to emerge on the other
side as a great eruption of red and yellow flame. The showers of debris, the falling bodies, and then that great blossoming
flower of white dust, roiling and churning upward, enveloping and consuming the mighty skyscraper as it collapses into the
whirlwind.
To Americans, those terrible moments stand as a brightly lit portal through which we were all compelled to step, together,
into a different world. Since that day ten years ago we have lived in a subtly different country, and though we have grown
accustomed to these changes and think little of them now, certain words still appear often enough in the news—
Guantánamo, indefinite detention, torture—to remind us that ours remains a strange America. The contours of this
strangeness are not unknown in our history—the country has lived through broadly similar periods, at least half a dozen or
so, depending on how you count; but we have no proper name for them. State of siege? Martial law? State of emergency?
None of these expressions, familiar as they may be to other peoples, falls naturally from American lips.
What are we to call this subtly altered America? Clinton Rossiter, the great American scholar of “crisis government,”
writing in the shadow of World War II, called such times “constitutional dictatorship.” Others, more recently, have spoken
of a “9/11 Constitution” or an “Emergency Constitution.” Vivid terms all; and yet perhaps too narrowly drawn, placing as
they do the definitional weight entirely on law when this state of ours seems to have as much, or more, to do with politics
—with how we live now and who we are as a polity. This is in part why I prefer “the state of exception,” an umbrella term
that gathers beneath it those emergency categories while emphasizing that this state has as its defining characteristic that it
transcends the borders of the strictly legal—that it occupies, in the words of the philosopher Giorgio Agamben, “a position
at the limit between politics and law…an ambiguous, uncertain, borderline fringe, at the intersection of the legal and the
political.”
Call it, then, the s.
100 words per question, no references needed or quotations. Only.docxtamicawaysmith
100 words per question, no references needed or quotations. Only a general idea or opinion.
A.
· Compare and contrast two works from the Italian Baroque period with two works from the Renaissance. Be sure to note the appearance in the works of the defining characteristics from each period.
· Discuss why artistic expression shifted from the restrained stoicism of the Renaissance to that of the heightened emotion in the religious and other works of the Baroque.
B. From video
Goya -
The Third of May
- If you cannot see this video, click here -
https://youtu.be/e7piV4ocukg
Respond in writing to the following questions after reading Chapter 12, watching the video, and exploring the sites above.
1. Heroism, nationalism, and passion are themes associated with Romanticism. Which
three
landmarks of the nineteenth century are most representative of these themes? You can discuss art, philosophy, or literature.
2. Compare Neoclassicism and Romanticism as styles and sensibilities. What do their differences reflect about patronage, popular taste, and historical change? Provide specific examples from the chapters.
C.
1. From the arts of West Africa, what are some characteristics of African cultural heritage?
2. How did their religious beliefs influence their art and music.
D.
Watch video below
Manet -
Déjeuner
sur
l’herbe -
If you cannot see this video, click
https://youtu.be/3xBGF8H3bQ4
1. Viewers of Manet’s
Déjeuner sur l’herbe
initially responded to its public display by attacking the canvas with their umbrellas. Why?
2. What kind of art has evoked a comparable response in our own time? Do some research online. Find a recent work of art that caused controversy. Summarize the reasons for the controversy and your reaction to it. Try not post the same article as someone else. (This board is not POST FIRST, so you will be able to see what others have posted right away.) If you can, attach a picture of the image you are describing to your posting.
E.
Watch the video below. If you cannot see the video, click here:
https://youtu.be/XyLNPumMMTs
George Braque, Violin and Pitcher, (1909)
•
Pablo Picasso, Guernica, (1937)
•
Marcel Duchamp, Nude Descending a Staircase, (1912)
Respond in writing to the following question after reading Chapter 14 in your text, watching the video above, viewing the Web Assignments, and the sites above.
1. Describe how they three have departed from styles such as symbolism and impressionism of the late nineteenth century.
F.
Take some time to reflect on all we have covered in this course. Then, respond in writing to the following question.
1. After your experience in this course, describe why you feel the humanities are important.
Edit question's body
.
Biological screening of herbal drugs: Introduction and Need for
Phyto-Pharmacological Screening, New Strategies for evaluating
Natural Products, In vitro evaluation techniques for Antioxidants, Antimicrobial and Anticancer drugs. In vivo evaluation techniques
for Anti-inflammatory, Antiulcer, Anticancer, Wound healing, Antidiabetic, Hepatoprotective, Cardio protective, Diuretics and
Antifertility, Toxicity studies as per OECD guidelines
How to Make a Field invisible in Odoo 17Celine George
It is possible to hide or invisible some fields in odoo. Commonly using “invisible” attribute in the field definition to invisible the fields. This slide will show how to make a field invisible in odoo 17.
Unit 8 - Information and Communication Technology (Paper I).pdfThiyagu K
This slides describes the basic concepts of ICT, basics of Email, Emerging Technology and Digital Initiatives in Education. This presentations aligns with the UGC Paper I syllabus.
A Strategic Approach: GenAI in EducationPeter Windle
Artificial Intelligence (AI) technologies such as Generative AI, Image Generators and Large Language Models have had a dramatic impact on teaching, learning and assessment over the past 18 months. The most immediate threat AI posed was to Academic Integrity with Higher Education Institutes (HEIs) focusing their efforts on combating the use of GenAI in assessment. Guidelines were developed for staff and students, policies put in place too. Innovative educators have forged paths in the use of Generative AI for teaching, learning and assessments leading to pockets of transformation springing up across HEIs, often with little or no top-down guidance, support or direction.
This Gasta posits a strategic approach to integrating AI into HEIs to prepare staff, students and the curriculum for an evolving world and workplace. We will highlight the advantages of working with these technologies beyond the realm of teaching, learning and assessment by considering prompt engineering skills, industry impact, curriculum changes, and the need for staff upskilling. In contrast, not engaging strategically with Generative AI poses risks, including falling behind peers, missed opportunities and failing to ensure our graduates remain employable. The rapid evolution of AI technologies necessitates a proactive and strategic approach if we are to remain relevant.
Macroeconomics- Movie Location
This will be used as part of your Personal Professional Portfolio once graded.
Objective:
Prepare a presentation or a paper using research, basic comparative analysis, data organization and application of economic information. You will make an informed assessment of an economic climate outside of the United States to accomplish an entertainment industry objective.
Embracing GenAI - A Strategic ImperativePeter Windle
Artificial Intelligence (AI) technologies such as Generative AI, Image Generators and Large Language Models have had a dramatic impact on teaching, learning and assessment over the past 18 months. The most immediate threat AI posed was to Academic Integrity with Higher Education Institutes (HEIs) focusing their efforts on combating the use of GenAI in assessment. Guidelines were developed for staff and students, policies put in place too. Innovative educators have forged paths in the use of Generative AI for teaching, learning and assessments leading to pockets of transformation springing up across HEIs, often with little or no top-down guidance, support or direction.
This Gasta posits a strategic approach to integrating AI into HEIs to prepare staff, students and the curriculum for an evolving world and workplace. We will highlight the advantages of working with these technologies beyond the realm of teaching, learning and assessment by considering prompt engineering skills, industry impact, curriculum changes, and the need for staff upskilling. In contrast, not engaging strategically with Generative AI poses risks, including falling behind peers, missed opportunities and failing to ensure our graduates remain employable. The rapid evolution of AI technologies necessitates a proactive and strategic approach if we are to remain relevant.
1. 35NURSING ECONOMIC$/January-February 2011/Vol. 29/No.
1
T
HE WORLD OF ARISTOTLE AND
Ptolemy believed that Earth
was positioned at the cen-
ter of the universe. Thanks
to Galileo and Copernicus’s studies
in the 16th century, we know this
is not true and that the sun is the
center of our universe. Pers -
pectives of health care have
undergone similar, radical changes
in perception. For centuries we
had a hospital-centric view; an
illness-based model, where the majority of care was
provided in hospitals, when we were ill. In the last
few decades, that model has migrated to a more con-
tinuum of care view; a wellness/health maintenance
model, where emphasis of care is outside the hospital
in other venues such as outpatient, ambulatory/clin-
ic, and home care (see Figure 1).
But as we all know, this is still not where we need
to be to support the highest quality care at the right
cost. Despite a focus on moving care out of the hospi-
tals, one only needs to think about the process of
medication reconciliation between care venues to
realize the lack of seamless integration of care deliv-
2. ery and the challenges of supporting interoperability
across the continuum. Hence, here I am proposing the
patient centric view, where the patient actively partic-
ipates in his or her care and we look at delivering care
from a patient’s point of view. This allows us to break
down some of the barriers we have struggled with on
our journeys to promote higher quality care through
the use of health information technology (HIT). Now
we need to consider how the health care system
should revolve around the patient, rather than the
patient rotating around the hospital. Considering a
patient-centric point of view when implementing and
optimizing the use of HIT provides new perspectives
on the meaning of “integrated” health care.
Patient-Centric Care
It might seem odd that a health care organization
needs to be reminded to involve the patient in his or
her care. After all, this approach would certainly be
supported from a patient’s perspective. And, of
course, the health care industry has compelling rea-
sons to incorporate a strong customer and service
focus in order to improve patient satisfaction and
impact patient loyalty. But as health care systems
Patient as Center of the Health Care Universe:
A Closer Look at Patient-Centered Care
JUDY MURPHY, RN, FACMI, FHIMSS, is Vice President-
Information Services, Aurora Health Care, Milwaukee, WI; a
HIMSS Board Member; Co-Chair of the Alliance for Nursing
Informatics; a member of the federal HIT Standards Committee;
and is a Nursing Economic$ Editorial Board Member.
Comments
and suggestions can be sent to [email protected]
3. EXECUTIVE SUMMARY
We need to consider how the health care system
should revolve around the patient, rather than the
patient rotating around the hospital.
Considering a patient-centric point of view when
implementing and optimizing the use of health infor-
mation technology (HIT) provides new perspectives
on the meaning of “integrated” health care.
Not only do we need to give patients the opportuni-
ties to participate as true partners in their health care,
we must convince them why this partnership makes
sense.
We should not be naive and believe all patients want
this involvement in their care today and are ready to
do all their health care transactions electronically.
But considering and using these practices are impor-
tant steps in the health care reform journey to
improve quality and decrease cost.
Many patients will benefit by our working with them to
demystify the health care experience through patient-
centric practices and the use of HIT.
Information Systems & Technology
Judy Murphy
Judy Murphy
Figure 1.
Patient as Center of the Health Care Universe
Hospitals
Specialists
Primary Care
4. Home Care
eHealth
Patient
NURSING ECONOMIC$/January-February 2011/Vol. 29/No.
136
have grown more complex and fragmented, and as cli-
nicians have felt pressured to be more productive,
care has become more centered around the needs of
the system – often at the patient’s expense.
Patient-centric care includes the patient and her
or his significant others as an integral part of the care
team. They collaborate with health professionals to
make decisions about their wellness and illness care.
Patient-centered care encourages patients to take
responsibility for important aspects of their preven-
tive self-care practices, as well as any disease manage-
ment strategies and monitoring. Patient-centric care
helps the flow between health care settings be more
seamless, as the patient is an active participant and
the health care providers are paying attention to the
needs of the patient. When care is centered around
the patient, opportunity exists to remove unneeded
and unwanted services. So, just how can technology
help to support patient-centric care and help improve
patient outcomes? Let’s investigate four practices
where technology can help.
eHealth
5. The HIT industry has just begun to tap into the
potential of eHealth and the value of patients partici-
pating in their own care using web-based tools. Often
this is seen as a “self-service” option, and possibly as
a productivity enhancer for the health care organiza-
tion. But, opening our registration systems and sched-
uling books so patients can arrange appointments
when it is most convenient for them serves the more
important purpose of demonstrating they are true
partners in their care. Further, to have patients update
their demographics, insurance, allergies, and medica-
tion lists puts the accountability for the accuracy of
this information, not only where it belongs, but where
the source of truth lies. This is, of course, the under-
lying principle of Microsoft’s HealthVault, Google
Health, Relay Health, or other personal health records
(PHRs) tethered to a health care organization’s elec-
tronic health records (EHRs), where patients create
their own account and store their personal health
information in a health record bank.
There is no other part of the human experience
where such a passive role is played as patients man-
aging their own health care. This needs to be turned
around if we are to reach the next level of care quali-
ty. It is the patient who is the constant across the care
continuum. By focusing on the patient, and not the
care venue, we can create the seamless integration
needed to provide the best care.
This area has one of the largest potentials for
impacting the quality of health care. Online storage of
immunization records, advanced directives, medica-
tion lists, medical histories, and a cadre of other per-
tinent medical information just makes sense and
6. allows the patient and practitioner to access them any
time from any care venue. Furthermore, computer-
generated health maintenance and disease manage-
ment reminders can support the evidence-based care
all clinicians strive to provide. Our challenge is clear:
not only do we need to give patients the opportunities
to participate as true partners in their health care, we
must convince them why this partnership makes
sense. But as their advocate, that is our job, too.
Nursing has a long history working as the
patient’s advocate. In this case, we need to work with
our patients so they can understand the importance of
their participation as a partner in their care, instead of
playing a passive role. One way we can do that is to
encourage our patients to actively use a PHR to man-
age their own health care and to partner with their
health care providers.
Primary Care
Little is known about the extent to which primary
care physicians support or practice patient-centered
care, which is one of the Institute of Medicine’s (2001)
six dimensions of quality. A Commonwealth Fund
study (Audet, Davis, & Schoenbaum, 2006) of patient-
centered practices by primary care physicians focused
on 11 specific patient-centered care practices: same-
day appointments, e-mail with patients, reminder
notices for preventive or follow-up care, registries of
patients with chronic conditions, patient medication
lists, electronic medical records, information from
referral physicians promptly available, medical
records/test results readily available when needed,
patient survey data fed back to practice, patient ratings
7. of care affect compensation, and information on quali-
ty of care of referral physicians available. The
researchers rated physicians’ patient-centered practice
scores as low, medium, or high based on how many of
these 11 patient-centered care practices they adopted.
Twenty percent scored in the low range (0-2 practices
adopted), 58% in the medium range (3-5), and 22% in
the high range (6-11). Actually, these results aren’t too
bad, but automation in the physician office could
improve these patient-centered practices even more.
This same study documented that only 16% of
primary care physicians used e-mail to communicate
with their patients, 74% experienced problems with
the availability of their patients’ medical records or
test results, and only 50% had adopted patient
reminder systems. Imagine if the physician office was
fully automated with an electronic patient record
integrated with a patient portal for eHealth. First and
foremost, the patient’s medical record would always
be available. Results and reminders would be generat-
ed electronically and sent to the patient. The patient
could respond with questions, and document other
results for the physician. A good medication list
could be co-owned and maintained. It is easy to see
how shifting the focus to the patient and away from
the provider or clinic system could impact patient
care and satisfaction in a positive way.
37NURSING ECONOMIC$/January-February 2011/Vol. 29/No.
1
The Patient Centered Medical Home (PCMH)
model in primary care promotes patient-centered care
8. by facilitating a partnership between individual
patients and their personal physicians. Care is facili-
tated by registries, information technology, health
information exchange, and other means to assure
patients get the indicated care when and where they
need and want it in a culturally and linguistically
appropriate manner. The National Committee for
Quality Assurance has published PCMH standards
and has a recognition program for primary care prac-
tices. This is another way to encourage the patient-
centric model and patients’ participation in their care.
Hospital Care
Focusing on the patient is not a new concept for the
inpatient setting, and probably is the venue that has the
richest history of incorporating patient-centric care
practices. But even here we can enhance the patient
experience by using technology to enable the hospital-
ized patient to participate more fully in his or her care.
What if hospitals implemented change-of-shift
walking rounds with computers-on-wheels, using
online shift report or task lists to remind patients of
what went on during the previous shift and inform
them of what is to come on the next shift? What about
a computer-generated “itinerary” of patient activities
for the day, so they know what to expect from lab,
nursing, and radiology, and can participate more fully
in their care? Why not include interactive patient
teaching modules patients could complete through
the TV? What about including patients on their own
outcome facilitation team, having them participate in
discharge planning rounds, or having them help
update their online care plan? Patient outcomes can
only be better if they know what we are working on
9. and can actively participate with us.
Health Information Exchange
One of the most important changes to improve
care coordination and create a patient-centric health
system in the United States is related to the ability to
exchange health care information between all care
venues: hospitals, clinics, physicians, home care, and
pharmacies. Of course, moving paper health records
around would never adequately serve this purpose, so
this initiative has been directly linked to EHRs. There
are local, regional, state, and federal initiatives under-
way to create the foundation and implementation
specifications for data interoperability between all
care venues and between varying EHR systems.
Significant parts of the American Recovery and
Reinvestment Act’s HITECH funding has gone toward
advancing the interoperability and portability of elec-
tronic health records. This includes sharing EHR
information with the PHR.
Imagine if a patient’s problem list, family history,
medication list, allergy list, and vital signs were
always available to any care provider in any location.
Imagine if the patient’s lab data, last chest x-ray, or
last mammogram result were readily available during
a followup exam. Imagine if all histories and physi-
cals, consults, outpatient reports, and discharge sum-
maries were accessible. There would certainly be less
repeats of tests because previous results were not
available, and there would be better care decisions
because data would be available. These are practices
that focus on the patient and promote patient-centric
care, enabled by HIT.
10. Summary
The federal EHR Incentive Program identified
many of the principles discussed here in the criteria
to qualify for “meaningful use” of certified EHR
incentives. Two of the five meaningful use initiatives
incorporate specific objectives focused on patient-
centric care: engaging patients and families, and
improving care coordination. This includes ensuring
the EHR can customize delivery of information to the
patient, provide an electronic copy of discharge
instructions and a summary of care, as well as the
ability to electronically transmit health information
from one care venue to another.
We should not be naive and believe all patients
want this involvement in their care today and are
ready to do all their health care transactions electron-
ically, but considering and using these practices are
important steps in the health care reform journey to
improve quality and decrease cost in the United
States. Many patients will benefit by our help in
demystifying the health care experience through
patient-centric practices and the use of HIT. $
REFERENCES
Audet, A.M., Davis, K., Schoenbaum, S.C. (2006). Adoption of
patient-centered care practices by physicians – Results from a
national survey. Archives of Internal Medicine, 166, 754-759.
Institute of Medicine. (2001). Crossing the quality chasm: A
new
health system for the 21st century. Washington, DC: Author.
11. Copyright of Nursing Economic$ is the property of Jannetti
Publications, Inc. and its content may not be copied
or emailed to multiple sites or posted to a listserv without the
copyright holder's express written permission.
However, users may print, download, or email articles for
individual use.
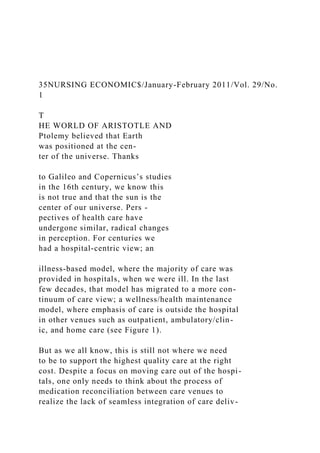
![ery and the challenges of supporting interoperability
across the continuum. Hence, here I am proposing the
patient centric view, where the patient actively partic-
ipates in his or her care and we look at delivering care
from a patient’s point of view. This allows us to break
down some of the barriers we have struggled with on
our journeys to promote higher quality care through
the use of health information technology (HIT). Now
we need to consider how the health care system
should revolve around the patient, rather than the
patient rotating around the hospital. Considering a
patient-centric point of view when implementing and
optimizing the use of HIT provides new perspectives
on the meaning of “integrated” health care.
Patient-Centric Care
It might seem odd that a health care organization
needs to be reminded to involve the patient in his or
her care. After all, this approach would certainly be
supported from a patient’s perspective. And, of
course, the health care industry has compelling rea-
sons to incorporate a strong customer and service
focus in order to improve patient satisfaction and
impact patient loyalty. But as health care systems
Patient as Center of the Health Care Universe:
A Closer Look at Patient-Centered Care
JUDY MURPHY, RN, FACMI, FHIMSS, is Vice President-
Information Services, Aurora Health Care, Milwaukee, WI; a
HIMSS Board Member; Co-Chair of the Alliance for Nursing
Informatics; a member of the federal HIT Standards Committee;
and is a Nursing Economic$ Editorial Board Member.
Comments
and suggestions can be sent to [email protected]](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)