Download to read offline
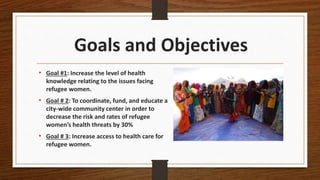
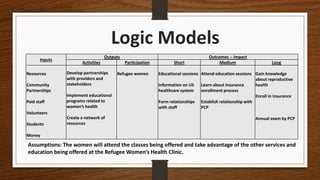

This document outlines a program to address the health needs of refugee women in Dallas-Fort Worth. The program has three goals: 1) increase health knowledge of issues facing refugee women, 2) decrease health threats for refugee women by 30% through education and a community center, and 3) increase access to healthcare. The program will develop partnerships, implement educational programs, and create a resource network. An evaluation plan will assess increases in knowledge, attendance at educational sessions, physician follow-up visits, and health insurance enrollment to measure the program's success in improving refugee women's health.
























































