Downloaded 16 times

![Boosted PIs in Clinical Practice
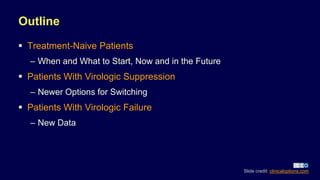
ACTG A5257[1]
– Similar efficacy between
RAL, DRV/RTV, and
ATV/RTV
– Better tolerability for RAL or
DRV/RTV than ATV/RTV
DRV/COBI and ATV/COBI
available for simplification[2,3]
Consider boosted PIs when
high barrier to resistance is
needed[4]
– If starting ART prior to
availability of resistance
data, if high risk of poor
adherence
Boosted PIs more widely
used in those with
transmitted or acquired
drug resistance
1. Lennox JL, et al. Ann Intern Med. 2014;161:461-471. 2. Gallant JE, et al. J Infect Dis.
2013;208:32-39. 3. Tashima K, et al. AIDS Res Ther. 2014;11:39. 4. DHHS guidelines. March 2018. Slide credit: clinicaloptions.com](https://image.slidesharecdn.com/hivtreatmentoptimization-180601010111/85/2018-HIV-Treatment-Optimization-2018-8-320.jpg)
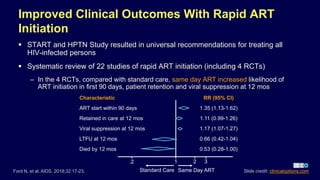
![Novel Darunavir-Containing First-line Therapy:
Efficacy at Wk 48
1. Gallant J, et al. EACS 2017. Abstract PS8/2. 2. Figueroa MI, et al. CROI 2018. Abstract 489. Slide credit: clinicaloptions.com
*Primary endpoint: HIV-1 RNA < 50 c/mL by FDA snapshot.
AMBER: Virologic Outcomes[1]
DRV/COBI/FTC/TAF (n = 362)
DRV/COBI + FTC/TDF (n = 363)
Treatment difference: 2.7%
(95% CI: -1.6% to 7.1%)
91.4 88.4
3.3
(n = 12)
4.4
(n = 16)
Patients(%)
100
80
60
40
20
0
Virologic
Success*
HIV-1 RNA
≥ 50 c/mL
93 9194 92
0
20
40
60
80
100
All Patients Patients With BL HIV-1
RNA > 100,000 c/mL
(n = 35)
Patients(%)
ANDES: HIV-1 RNA < 50 copies/mL (ITT)[2]
Treatment difference: -1.0%
(95% CI: -7.5% to 5.6%)
Treatment difference: -1.4%
(95% CI: -17.2% to 14.4%)
No Virologic
Data
4
8
DRV/RTV + 3TC DRV/RTV + 3TC/TDF
70/
145
66/
145
n/N =
20/
35
12/
35](https://image.slidesharecdn.com/hivtreatmentoptimization-180601010111/85/2018-HIV-Treatment-Optimization-2018-9-320.jpg)

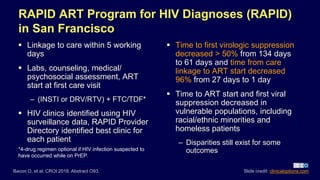
![BIC/FTC/TAF vs DTG-Containing Regimens
for Treatment-Naive Patients
Slide credit: clinicaloptions.com
GS-1489: Wk 48 Virologic Efficacy[1] GS-1490: Wk 48 Virologic Efficacy[2]
Patients(%)
Patients(%)
100
80
60
40
20
0
HIV-1 RNA
< 50 c/mL
HIV-1 RNA
≥ 50 c/mL
No Virologic
Data
BIC/FTC/TAF (n = 314)
DTG/ABC/3TC (n = 315)
92 93
1 3 7 4
100
80
60
40
20
0
HIV-1 RNA
< 50 c/mL
No Virologic
Data
BIC/FTC/TAF (n = 320)
DTG + FTC/TAF (n = 325)
89 93
4 1
66
Treatment difference: -0.6%
(95% CI: -4.8% to 3.6%)
Treatment difference: -3.5%
(95% CI: -7.9% to 1.0%)
1. Gallant J, et al. Lancet. 2017;390:2063-2072. 2. Sax PE, et al. Lancet. 2017;390:2073-2082.
No resistance selected for in any DTG- or BIC-containing regimen
HIV-1 RNA
≥ 50 c/mL](https://image.slidesharecdn.com/hivtreatmentoptimization-180601010111/85/2018-HIV-Treatment-Optimization-2018-12-320.jpg)
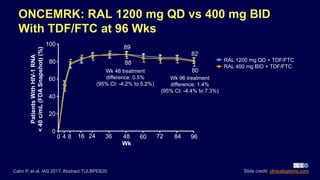
![BIC/FTC/TAF FDA Approved: March 2018
Once-daily single-tablet regimen with novel, unboosted INSTI
BIC/FTC/TAF [package insert]. 2018.
Key US Label Information
Indications
For treatment-naive patients
For patients with HIV-1 RNA < 50 copies/mL for ≥ 3 mos, no history of
treatment failure, and no resistance to regimen components
Key DDIs
Contraindicated with rifampin, dofetilide
May increase metformin concentrations
Polyvalent cation–containing supplements/medications (including antacids)
may decrease BIC concentration
Special
populations
Not recommended for patients with estimated CrCl < 30 mL/min
BIC only available in combination STR; not approved for use with other ARVs
Slide credit: clinicaloptions.com](https://image.slidesharecdn.com/hivtreatmentoptimization-180601010111/85/2018-HIV-Treatment-Optimization-2018-13-320.jpg)
![Class DHHS[1] IAS-USA*[2]
INSTI BIC/TAF/FTC
DTG/ABC/3TC
DTG + (TAF or TDF)/FTC
EVG/COBI/(TAF or TDF)/FTC
RAL + (TAF or TDF)/FTC
DTG/ABC/3TC
DTG + TAF/FTC
EVG/COBI/TAF/FTC
RAL + TAF/FTC
DHHS, IAS-USA Guidelines:
Recommended Regimens for First-line ART
Recommendations may differ based on BL HIV-1 RNA, CD4+ cell count,
CrCl, eGFR, HLA-B*5701 status, HBsAg status, and osteoporosis status
With FDA approval of 1200-mg RAL,[3] all options now available QD (except
in pregnancy)
1. DHHS guidelines. March 2018. 2. Günthard HF, et al.
JAMA. 2016;316:191-210. 3. Raltegravir [package insert]. 2018.
Bold text identifies single-tablet regimens. *IAS-USA guidelines not updated since the approval of BIC/TAF/FTC.
Slide credit: clinicaloptions.com](https://image.slidesharecdn.com/hivtreatmentoptimization-180601010111/85/2018-HIV-Treatment-Optimization-2018-14-320.jpg)
![Choosing Integrase Inhibitors
Agent Advantages Disadvantages
Bictegravir
STR once daily
Available with TAF
Few drug or food interactions
Potentially high barrier to resistance
Least amount of data
Only available as STR with TAF/FTC
Dolutegravir
Only non-TFV QD STR
High barrier to resistance
Few drug or food interactions
Active against some RAL- and
EVG-resistant viruses
STR only with ABC/3TC
Increases metformin levels
Elvitegravir
STR once daily
Available with TAF and TDF
Requires COBI boosting
COBI drug interactions
Raltegravir
Longest experience
Few drug or food interactions
Multiple pills
No STR
DHHS guidelines. March 2018. Dolutegravir [package insert]. 2017. Slide credit: clinicaloptions.com](https://image.slidesharecdn.com/hivtreatmentoptimization-180601010111/85/2018-HIV-Treatment-Optimization-2018-15-320.jpg)
![Doravirine for Treatment-Naive Patients:
Efficacy at Wk 48
n = 1 noncompliant patient d/c at Wk 24,
developed DOR and FTC resistance
1. Molina JM, et al. Lancet HIV. 2018;[Epub ahead of print].
2. Squires KE, et al. IAS 2017. Abstract TUAB0104LB.
0
HIV-1 RNA
< 50 c/mL
HIV-1 RNA
≥ 50 c/mL
No Data in
Window
Patients(%)
100
80
60
40
20
84 81
DOR/3TC/TDF (n = 364)
EFV/FTC/TDF (n = 364)
11 10
5
9
Treatment difference: 3.5%
(95% CI: -2.0% to 9.0%)
DRIVE-AHEAD[2]
Virologic
Nonresponse
HIV-1 RNA
< 50 c/mL
No Data
100
80
60
40
20
0
Patients(%)
84 80
11 13
5 7
Treatment difference: 3.9%
(95% CI: -1.6% to 9.4%)
DOR + 2 NRTIs (n = 383)
DRV + RTV + 2 NRTIs (n = 383)
DRIVE-FORWARD[1]
1° NNRTI resistance, n (%): DOR, 6 (1.6);
EFV, 12 (3.3); no unanticipated mutations
observed
Slide credit: clinicaloptions.com](https://image.slidesharecdn.com/hivtreatmentoptimization-180601010111/85/2018-HIV-Treatment-Optimization-2018-17-320.jpg)
![Dual Therapy With Boosted PIs in ART-Naive
Patients
Randomized, open-label phase III
noninferiority trial (N = 805)
Randomized, open-label phase III
noninferiority trial (N = 416)
Overall
BL HIV-1 RNA < 100,000 c/mL
BL HIV-1 RNA ≥ 100,000 c/mL
CD4+ cell count < 200 cells/mm3*
CD4+ cell count ≥ 200 cells/mm3*
Adjusted Difference in Proportions of Failure at Wk 96, % (95% CI)
RAL +
DRV/RTV
TDF/FTC +
DRV/RTV
*Interaction test P = .010
NEAT: DRV/RTV + RAL
vs DRV/RTV + TDF/FTC[1]
GARDEL: LPV/RTV + 3TC
vs LPV/RTV + 2 NRTIs[2]
Wks
Patients(%)
Difference: 4.6%
(95% CI: -2.2% to 11.8%;
P = .171)
1. Raffi F, et al. Lancet. 2014;384:1942-1951. 2. Cahn P, et al. Lancet Infect Dis. 2014;14:572-580. Slide credit: clinicaloptions.com
HIV-1 RNA < 50 copies/mL
17.8
7.4
36.8
43.2
13.7
13.8
7.3
27.3
20.9
12.3
-5 0 5 1015 20253035 40
Dual therapy
Triple therapy
0
100
80
60
40
20
0 4 8 12 24 36 48](https://image.slidesharecdn.com/hivtreatmentoptimization-180601010111/85/2018-HIV-Treatment-Optimization-2018-19-320.jpg)
![ACTG A5353: Pilot Study of Dolutegravir +
Lamivudine in Treatment-Naive Patients
Single-arm, 52-wk phase II study
(N = 120)[1]
– HIV-1 RNA ≥ 1000 to < 500,000 c/mL;
no PI, INSTI, or reverse transcriptase
resistance; no active HBV infection
– Median age, 30 yrs; male, 87%; median
CD4+ cell count, 387 cells/mm3; median
HIV-1 RNA, 4.61 log10 copies/mL
Primary efficacy outcome
– 90% achieved HIV RNA-1 < 50 copies/mL
at Wk 24 (FDA Snapshot)
No discontinuations due to AEs
1. Taiwo BO, et al. Clin Infect Dis. 2017;[Epub ahead of print].
2. ClinicalTrials.gov. NCT02831673. 3. ClinicalTrials.gov. NCT02831673. Slide credit: clinicaloptions.com
Outcome, %
BL HIV-1 RNA, c/mL
> 100,000
(n = 37)
≤ 100,000
(n = 83)
HIV-1 RNA < 50 c/mL 89 90
Virologic nonsuccess
HIV-1 RNA ≥ 50 c/mL
D/c for other reasons* while
HIV-1 RNA ≥ 50 c/mL
8
0
0
2
Virologic Outcomes at Wk 24[1]
Fully powered phase III
GEMINI-1[2] and -2[3] under way](https://image.slidesharecdn.com/hivtreatmentoptimization-180601010111/85/2018-HIV-Treatment-Optimization-2018-20-320.jpg)
![Within Class
EFV RPV[1]
RAL EVG[2] or DTG[3]
DTG BIC[4]
Boosted DRV, DRV/C/FTC/TAF[5]
boosted ATV,
or LPV/RTV
TDF or ABC TAF[6,7]
Switch Studies With Evidence of Sustained
Efficacy
Between Class
Boosted PI RPV[8]
Boosted PI EVG,[9] DTG,[10] or
BIC[11]
NNRTI EVG[12] or DTG[3]
References in slidenotes Slide credit: clinicaloptions.com](https://image.slidesharecdn.com/hivtreatmentoptimization-180601010111/85/2018-HIV-Treatment-Optimization-2018-23-320.jpg)
![BIC/FTC/TAF for Initial/Maintenance Therapy
Once-daily single-tablet regimen with novel, unboosted INSTI
BIC/FTC/TAF [package insert]. 2018.
Key US Label Information
Indications
For treatment-naive patients
For patients with HIV-1 RNA < 50 copies/mL for ≥ 3 mos, no history of
treatment failure, and no resistance to regimen components
Key DDIs
Contraindicated with rifampin, dofetilide
May increase metformin concentrations
Polyvalent cation–containing supplements/medications (including antacids)
may decrease BIC concentration
Special
populations
Not recommended for patients with estimated CrCl < 30 mL/min
BIC only available in combination STR; not approved for use with other ARVs
Slide credit: clinicaloptions.com](https://image.slidesharecdn.com/hivtreatmentoptimization-180601010111/85/2018-HIV-Treatment-Optimization-2018-25-320.jpg)
![DTG/RPV FDA Approved for Maintenance
Therapy: November 2017
Once-daily single-tablet regimen of DTG/RPV
– First 2-drug STR approved by FDA for use as a complete regimen in the US
DTG/RPV [package insert]. 2018. DHHS guidelines. March 2018.
Key US Label Information
Indication
For patients who have been virologically suppressed for ≥ 6 mos
Patients must have no history of treatment failure and no resistance to DTG or RPV
Administration
requirements
Must be taken with a meal
Key DDIs
Separate dose of DTG/RPV and antacid/polyvalent cation–containing medications
Avoid PPIs (eg, omeprazole, pantoprazole)
Dose
adjustments
None required for patients with mild/moderate renal impairment; in patients with CrCl
< 30 mL/min, increase monitoring for AEs
DHHS Consider when NRTIs not desirable
Slide credit: clinicaloptions.com](https://image.slidesharecdn.com/hivtreatmentoptimization-180601010111/85/2018-HIV-Treatment-Optimization-2018-27-320.jpg)
![ASPIRE: DTG + 3TC Maintenance Therapy
DTG + 3TC as effective as
standard 3-drug therapy
(blips, n = 1)
– Virologic failure, n = 1 in each arm
– No emergence of resistance
CD4+ cell count gain was similar
Both regimens well tolerated
– D/c due to AE: dual therapy, n = 1
– Similar changes in lipids and CrCl
Fully powered phase III TANGO enrolling
Taiwo BO, et al. Clin Infect Dis. 2017;[Epub ahead of print]. Slide credit: clinicaloptions.com
Wk 48Wk 24 Wk 24
100
80
60
40
20
0
Patients(%)
1 0
93 91 91 89
Wk 48 treatment
difference: 2.0%
(95% CI: -12.6%
to 16.5%)
DTG + 3TC (n = 44)
Continue triple therapy (n = 45)
Virologic Outcomes (FDA Snapshot)
Wk 48
Virologic Failure HIV-1 RNA < 50 c/mL
0 0](https://image.slidesharecdn.com/hivtreatmentoptimization-180601010111/85/2018-HIV-Treatment-Optimization-2018-30-320.jpg)
![1. Margolis DA, et al. Lancet 2017;390:1499-1510. 2. ClinicalTrials.gov. NCT02951052.
3. Clinical Trials.gov. NCT02938520. 4. Clinical Trials.gov. NCT03299049.
Fully powered phase III
ATLAS, FLAIR (every
month)[2,3] and ATLAS-2M
(every 2 months)[4] enrolling
LATTE-2: Maintenance Therapy With
Cabotegravir IM + RPV IM
Multicenter, open-label phase IIb study comparing continuation of oral CAB +
ABC/3TC vs switching to IM CAB + RPV Q4W or Q8W (after induction with oral
CAB + ABC/3TC)[1]
Virologic Outcomes
94
HIV-1RNA<50c/mL(%)
Virologic
Success
Virologic
Nonresponse
No Virologic
Data
87
100
80
60
40
20
0
Q8W IM CAB + RPV (n = 115)
Q4W IM CAB + RPV (n = 115)
Oral CAB + ABC/3TC (n = 56)
84
4
0 2
13
2
14
Slide credit: clinicaloptions.com](https://image.slidesharecdn.com/hivtreatmentoptimization-180601010111/85/2018-HIV-Treatment-Optimization-2018-31-320.jpg)
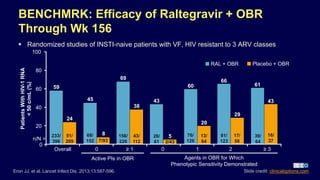
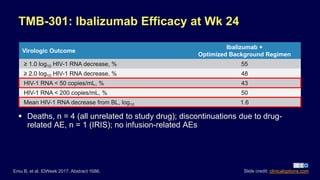
![TMB-311: Ibalizumab in Pretreated Patients
Infected With Multidrug-Resistant HIV
Ibalizumab: humanized mAb to CD4 receptor that blocks HIV entry into
CD4+ T-cells[1]
– FDA approved March 2018 as IV injection for heavily treatment–experienced adults with
multidrug-resistant HIV infection and virologic failure
Single-arm, open-label phase III trial in patients on a failing regimen (N = 40)[2,3]
Patients with HIV-1 RNA
> 1000 c/mL; on ART ≥ 6 mos,
on stable ART ≥ 8 wks;
resistant to ≥ 1 ARV from
3 classes, sensitive to
≥ 1 ARV for OBR
(N = 40)
Wk 25
Ibalizumab
2000 mg IV Day 7
(loading dose)
Continue Failing ART
Days 0-14
Ibalizumab
800 mg IV Day 21, Q2W
(maintenance dose)
Switch to OBR
Day 14
Primary Endpoint:
Day 14Control Period:
Day 0-7
1. Ibalizumab [package insert]. 2018. 2. Emu B, et al.
IDWeek 2017. Abstract 1686. 3. ClinicalTrials.gov. NCT02475629. Slide credit: clinicaloptions.com](https://image.slidesharecdn.com/hivtreatmentoptimization-180601010111/85/2018-HIV-Treatment-Optimization-2018-37-320.jpg)

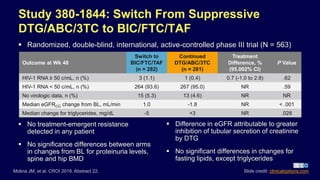
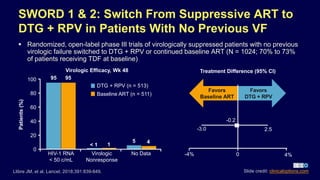
The document provides an overview of HIV treatment optimization strategies as discussed by Dr. Eric S. Daar, highlighting the importance of immediate ART initiation and newer treatment regimens for various patient scenarios including treatment-naive and those with virologic suppression. It reviews clinical studies supporting rapid ART initiation and compares the efficacy of novel therapies such as bictegravir and doravirine. Recommendations for switching therapy in patients with virologic suppression are also outlined, focusing on maintaining viral control while considering tolerability and drug interactions.

















































































