Downloaded 12 times


![Slide credit: clinicaloptions.com
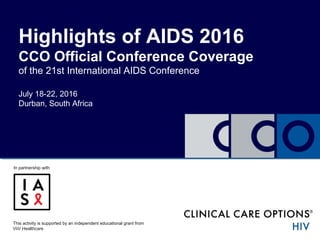
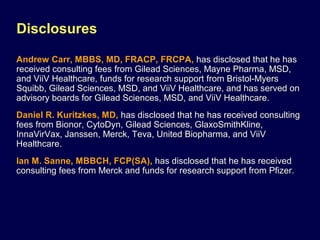
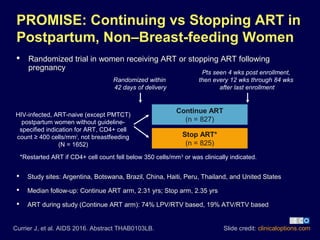
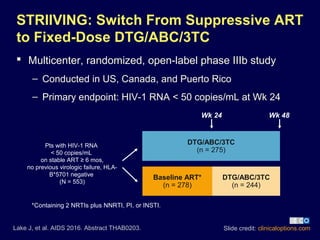
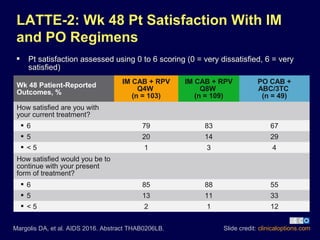
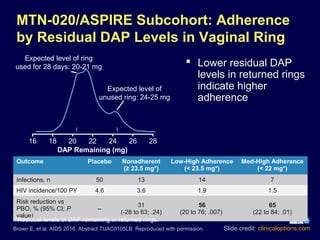
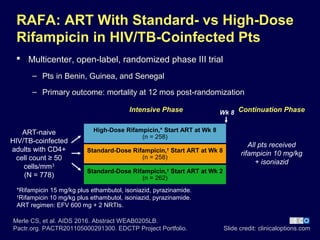
MTN-020/ASPIRE: Dapivirine Vaginal Ring
for HIV Prevention in Women
Multicenter, double-blind, placebo-controlled, randomized phase III
trial in Malawi, South Africa, Uganda, and Zimbabwe
Silicone elastomer vaginal matrix ring containing NNRTI dapivirine
25 mg; ring replaced every 4 wks
Primary endpoints: efficacy and safety
HIV protection efficacy vs placebo: 27% (P = .046)
Brown E, et al. AIDS 2016. Abstract TUAC0105LB.
Baeten JM, et al. N Engl J Med. 2016;[Epub ahead of print].
Dapivirine 25 mg Vaginal Ring Q4W
+ HIV Prevention Service Package
(n = 1313)
Placebo Vaginal Ring Q4W
+ HIV Prevention Service Package
(n = 1316)
Sexually active HIV-
uninfected adult
women
(N = 2629)
≥ 1 yr; endpoint-
driven duration](https://image.slidesharecdn.com/highlightsofaids2016-160807011656/85/Highlights-of-AIDS-2016-22-320.jpg)
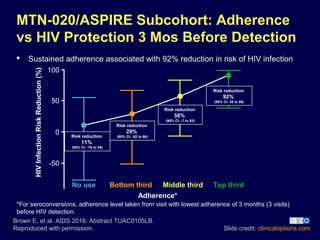
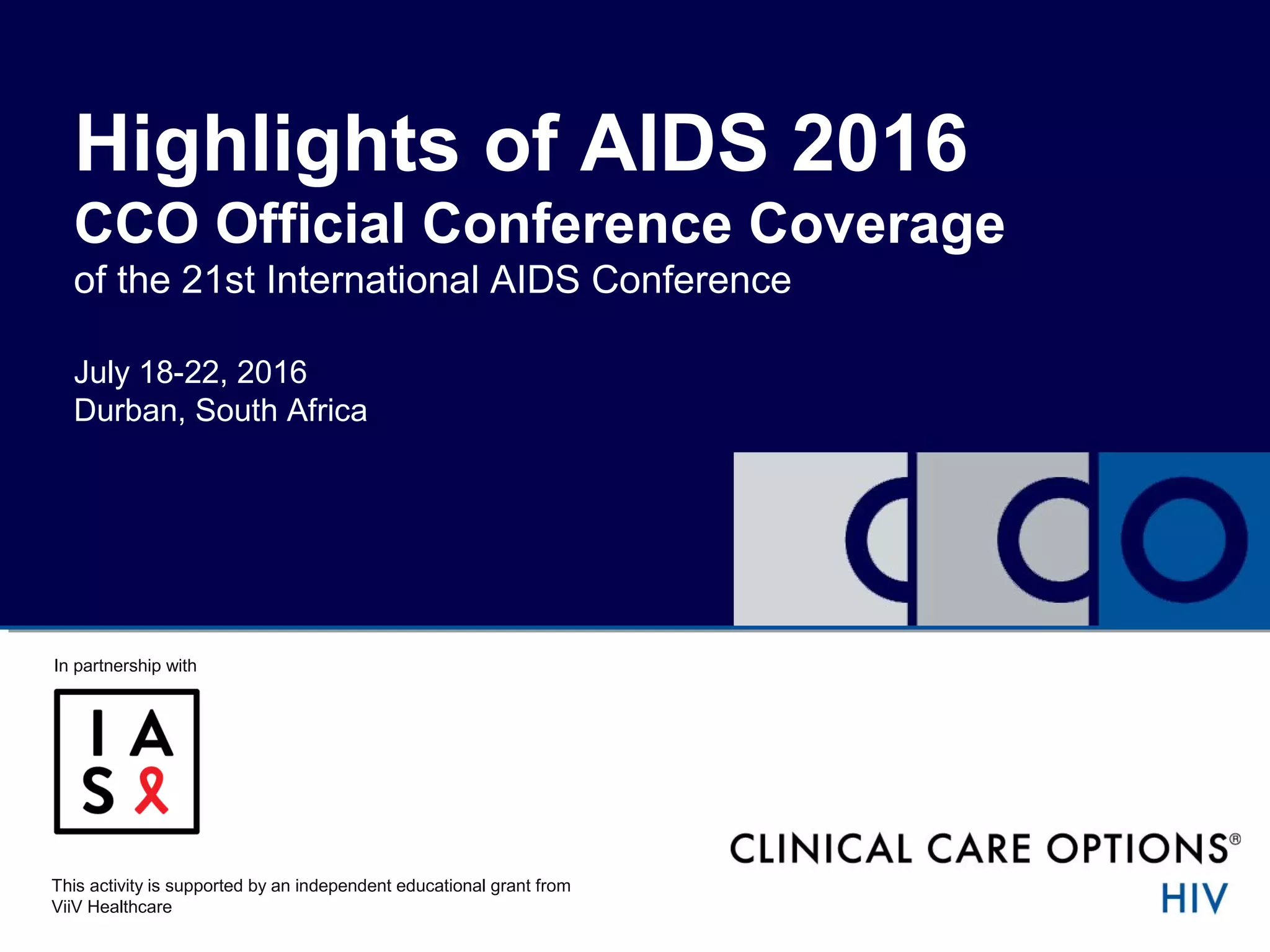
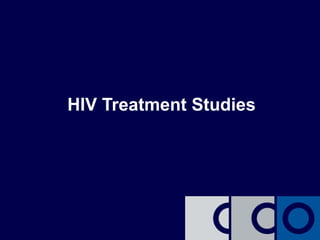
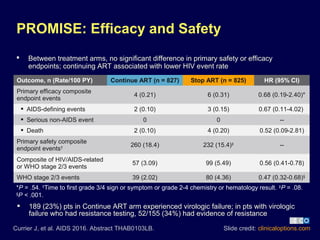
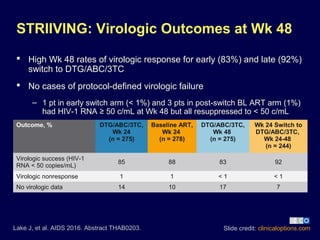
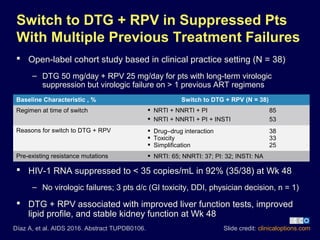
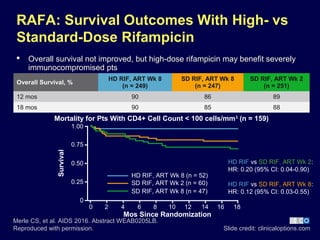
![ ASTRAL-5: multicenter, open-label, single-arm phase III study[1]
– 12 wks of SOF/VEL in HIV/HCV-coinfected, GT 1-6 HCV , tx naive or experienced,
stably suppressed on ART (N = 106)
Sofosbuvir/Velpatasvir in HIV/HCV-
Coinfected Pts
Slide credit: clinicaloptions.com
1. Bräu N, et al. AIDS 2016. Abstract WEAB0301. Reproduced with
permission.
2. Mogalian E,et al. AIDS 2016. Abstract WEAB0302.
Total
(n = 106)
HCV Genotype
BL
NS5A
RAVs
(n = 12)
1a
(n = 66)
1b
(n = 12)
2
(n = 11)
3
(n = 12)
4
(n = 5)
SVR12, % 95 95* 92†
100 92‡
100 100*Relapse, n = 2; LTFU, n = 1. †
LTFU, n = 1. ‡
Withdrew consent, n = 1.
Drug-drug interaction study in healthy volunteers[2]
– 50% reduction in VEL exposure when EFV/TDF/FTC and SOF/VEL coadministered;
EFV not recommended with SOF/VEL
– FTC, EFV, RPV, DTG, RAL, EVG, ATV, RTV, DRV, LPV, not affected by SOF/VEL;
TDF exposure increased ~20% to 81%](https://image.slidesharecdn.com/highlightsofaids2016-160807011656/85/Highlights-of-AIDS-2016-28-320.jpg)
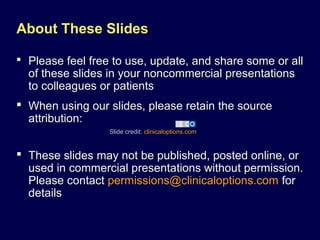
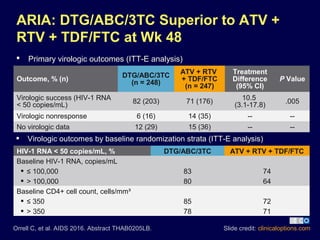
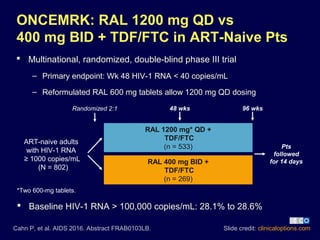
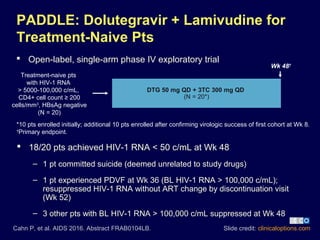
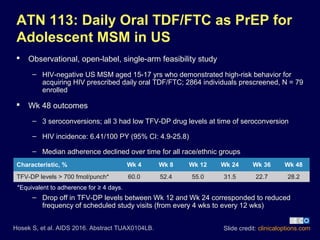
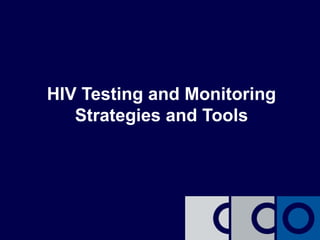
![Additional Studies Assessing HCV
Therapy in Pts With HIV/HCV Coinfection
TURQUOISE-I, Part 2: multicenter phase III trial in which HIV/HCV-
coinfected pts with GT1 or GT4 HCV treated with OBV/PTV/RTV ±
DSV ± RBV (N = 228)[1]
– SVR12 (ITT): GT1, 97% (n/N = 190/195); GT4, 96% (n/N = 27/28)
– Intermittent HIV viremia in 10/228 (4%) pts; HIV-1 RNA < 200 copies/mL
– 4% of pts in each arm had BL HIV-1 RNA ≥ 40 copies/mL
6 wks of SOF/LDV for HIV-infected pts with acute GT1/4 HCV
infection[2]
– SVR12: 77% (n/N = 20/26); 4 virologic failures (1 reinfection), 2 LTFU
– 3 relapsed pts had BL HCV RNA ≥ 7.0 log10 IU/mL
Slide credit: clinicaloptions.com
1. Rockstroh JK, et al. AIDS 2016. Abstract WEAB0304LB.
2. Nelson M, et al. AIDS 2016. Abstract WEPEB059.](https://image.slidesharecdn.com/highlightsofaids2016-160807011656/85/Highlights-of-AIDS-2016-29-320.jpg)
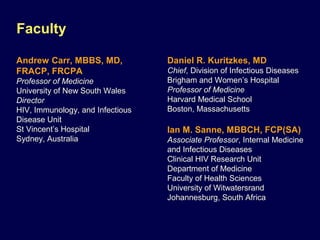
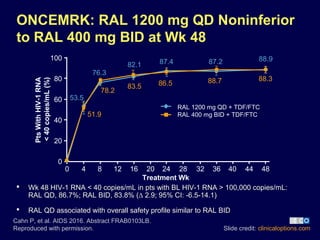
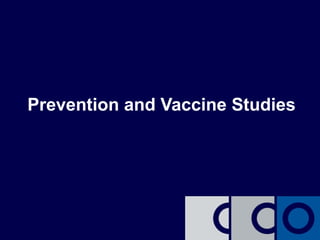
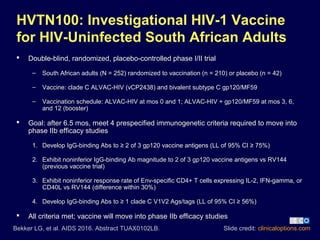
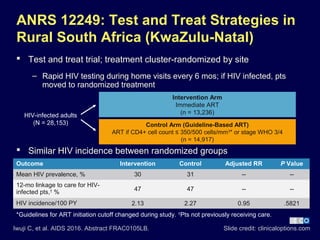
![Slide credit: clinicaloptions.com
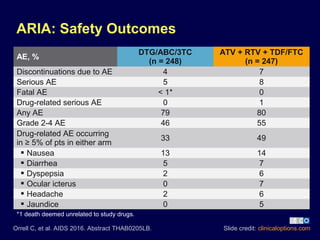
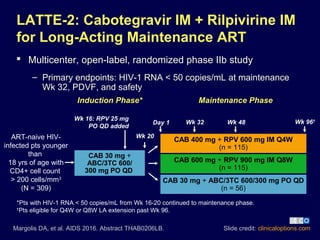
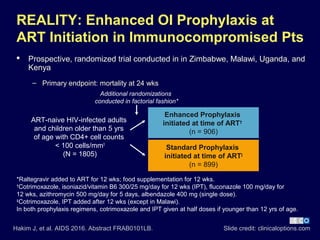
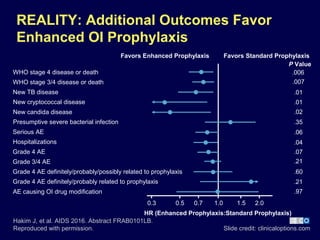
REALITY: Mortality Benefit With Enhanced
OI Prophylaxis for Pts Initiating ART
1. Hakim J, et al. AIDS 2016. Abstract FRAB0101LB.
2. Kityo C, et al. AIDS 2016. Abstract FRAB0102LB.
3.3 lives saved for every 100 treated with enhanced prophylaxis[1]
Additional REALITY factorial randomization assessed mortality for
ART initiation with 2 NRTIs + NNRTI + RAL vs 2 NRTIs + NNRTI[2]
– Addition of RAL to standard 3-drug ART did not affect all-cause mortality
at 24 or 48 wks
Deaths, %[1]
Enhanced
Prophylaxis
(n = 906)
Standard
Prophylaxis
(n = 899)
HR
(95% CI)
P Value
Wk 24* 8.9 12.2
0.73
(0.54-0.97)
.03
Wk 48 11.0 14.4
0.75
(0.58-0.98)
.04
*Primary endpoint.](https://image.slidesharecdn.com/highlightsofaids2016-160807011656/85/Highlights-of-AIDS-2016-32-320.jpg)
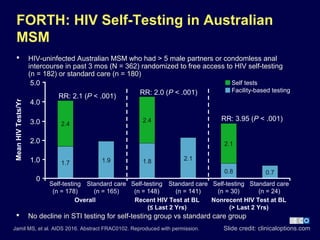
![Further Studies Assessing HIV Testing
Strategies
Strategies to improve male HIV testing for those in relationships in Kenya[1]
– Pregnant or postpartum women with male HIV-uninfected or HIV-unknown partners
randomized to groups in which they gave partner an HIV self-test (HIVST group,
n = 284) or HIV clinic referral voucher (comparison group, n = 286)
Slide credit: clinicaloptions.com
1. Agot K, et al. AIDS 2016. Abstract FRAC0104.
2. Patel VV, et al. AIDS 2016. Abstract FRAC0101.
Outcome, n (%) HIVST Comparison Difference, % (95% CI)
Male partner testing 258 (90.8) 148 (51.7) 39.1 (32.4 to 45.8)
Discuss HIV testing 271 (95.4) 276 (96.5) -1.1 (-4.3 to 2.2)
Couples testing 214 (75.4) 95 (33.2) 42.1 (34.7 to 49.6)
Learned partner’s HIV status 255 (89.8) 145 (50.7) 39.1 (32.3 to 45.9)
Partner violence due to testing 1 (0.4) 1 (0.3) 0.0 (-1.0 to 1.0)
CHALO: e-messaging reminders for HIV testing for MSM in India[2]
– Of pts who completed follow-up (N = 130), intervention increased recent HIV testing
vs baseline (44% vs 32%; P < .05); “avoidance” language emphasizing negative
outcomes was associated with higher rate of testing or intention to test vs
“approach” language highlighting a benefit (82% vs 65%, P =.03)](https://image.slidesharecdn.com/highlightsofaids2016-160807011656/85/Highlights-of-AIDS-2016-39-320.jpg)
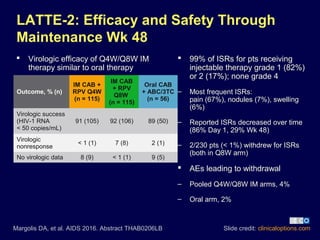
![ Validation of Cepheid GeneXpert HIV-1 Quant for monitoring HIV-1
RNA in pts on ART[1]
– Point-of-care, PCR-based testing system
– Compared with Abbott Real Time HIV-1 assay,
LAg-Avidity for detecting viral breakthrough for pts on ART[2]
Studies Assessing Tools for Monitoring
ART Efficacy and Failure
Slide credit: clinicaloptions.com
1. Kulkarni S, et al. AIDS 2016. Abstract THPDB0205. 2. Nicholas S, et al. AIDS
2016. Abstract THPEB046. 3. Wendel SK, et al. AIDS 2016. Abstract THPEB039.
Study Findings
Validation of GeneXpert HIV-1 Quant for
monitoring HIV-1 RNA in pts on ART[1]
Point-of-care, PCR-based testing system
Assessed samples from Indian pts with varying
HIV-1 RNA levels (N = 219) and controls
Similar detection with GeneXpert
vs standard Real Time assay:
R2
= 0.784
Sensitivity/specificity for detecting
HIV-1 RNA > 200 c/mL: 97%/100%
Assessment of SAMBA-1 for routine
monitoring of HIV-1 RNA in pts on ART[2]
Nearly point-of-care, PCR-based testing system
Assessed pts on first-line ART at hospital/health
centers in Malawi from Aug 2013 to Dec 2015
13675/19036 (72%) received ≥ 1 test
> 80% of tests reviewed the same day
at health centers
LAg-Avidity for detecting viral breakthrough
for pts on ART[3]
Antigen avidity enzyme immunoassay
Assessed samples from US pts pre/post ART
(n = 72) and suppressed pts who had
breakthrough (n = 179)
Sensitivity/specificity for detecting
viral breakthrough: 65%/86%](https://image.slidesharecdn.com/highlightsofaids2016-160807011656/85/Highlights-of-AIDS-2016-40-320.jpg)

The document summarizes the highlights and findings from the 21st International AIDS Conference held from July 18-22, 2016, in Durban, South Africa. It details several studies on HIV treatment, including the efficacy of various drug combinations in different patient populations, while also addressing safety outcomes and virologic success rates. Faculty disclosures and study methodologies are also outlined, emphasizing advances in HIV care and ongoing evaluation of treatment strategies.


























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)










