Downloaded 17 times



![Healthdata.be
Catalogue (PROD) with
Registry form definition
Data provider
Sending Data Through an
API & Prefilling Forms for
less Manual Work
Legend
Identifiers (SSIN, RIZIV, …)
Neeadata (internal ID, type data, …)
Medical data
CSV
24/7
HD4DP
and / or
HD4DP : Healthdata for Data Providers
healthdata.be
data we care for
• All manual input remains available
(structured and coded, according to
[inter]national standard) in local
database of DP:
• Import in future upgrade of
EPD/LIMS;
• Re-Use for internal BI & QI
All manual input remains available
(structured and coded, according to
[inter]national standard, based on CBBs)
in local database of DP:
• Import in future upgrade of
EPD/LIMS;
• Re-Use for internal BI & QI
• All manual input remains available
(structured and coded, according to
[inter]national standard) in local
database of DP:
• Import in future upgrade of
EPD/LIMS;
• Re-Use for internal BI & QI
Clinical Building Blocks .BE](https://image.slidesharecdn.com/20151027hdcbbsv01-151113114359-lva1-app6892/75/20151027-healthdata-be-workshop-Clinical-Building-Blocks-with-NICTIZ-and-NFU-16-2048.jpg)



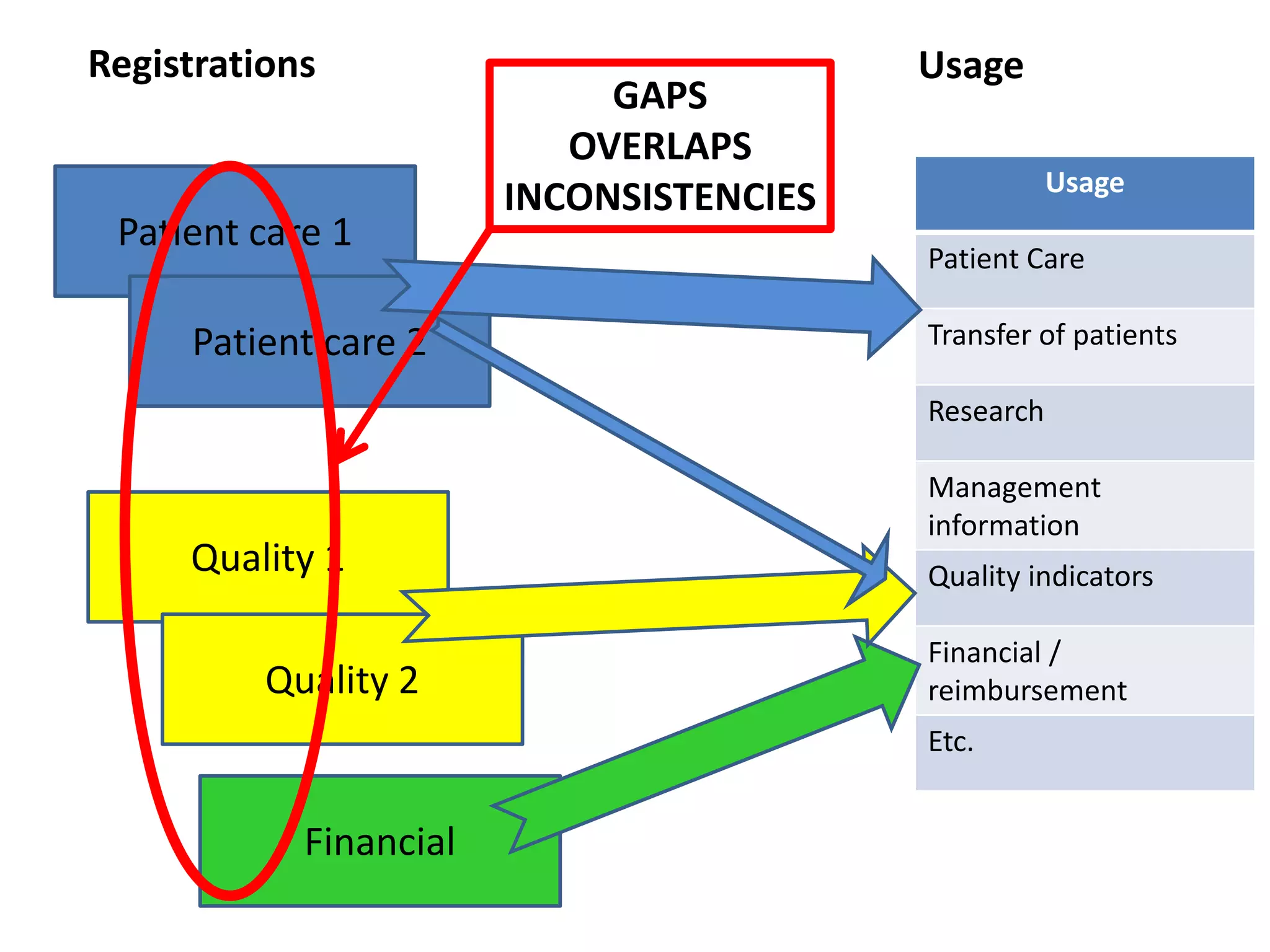
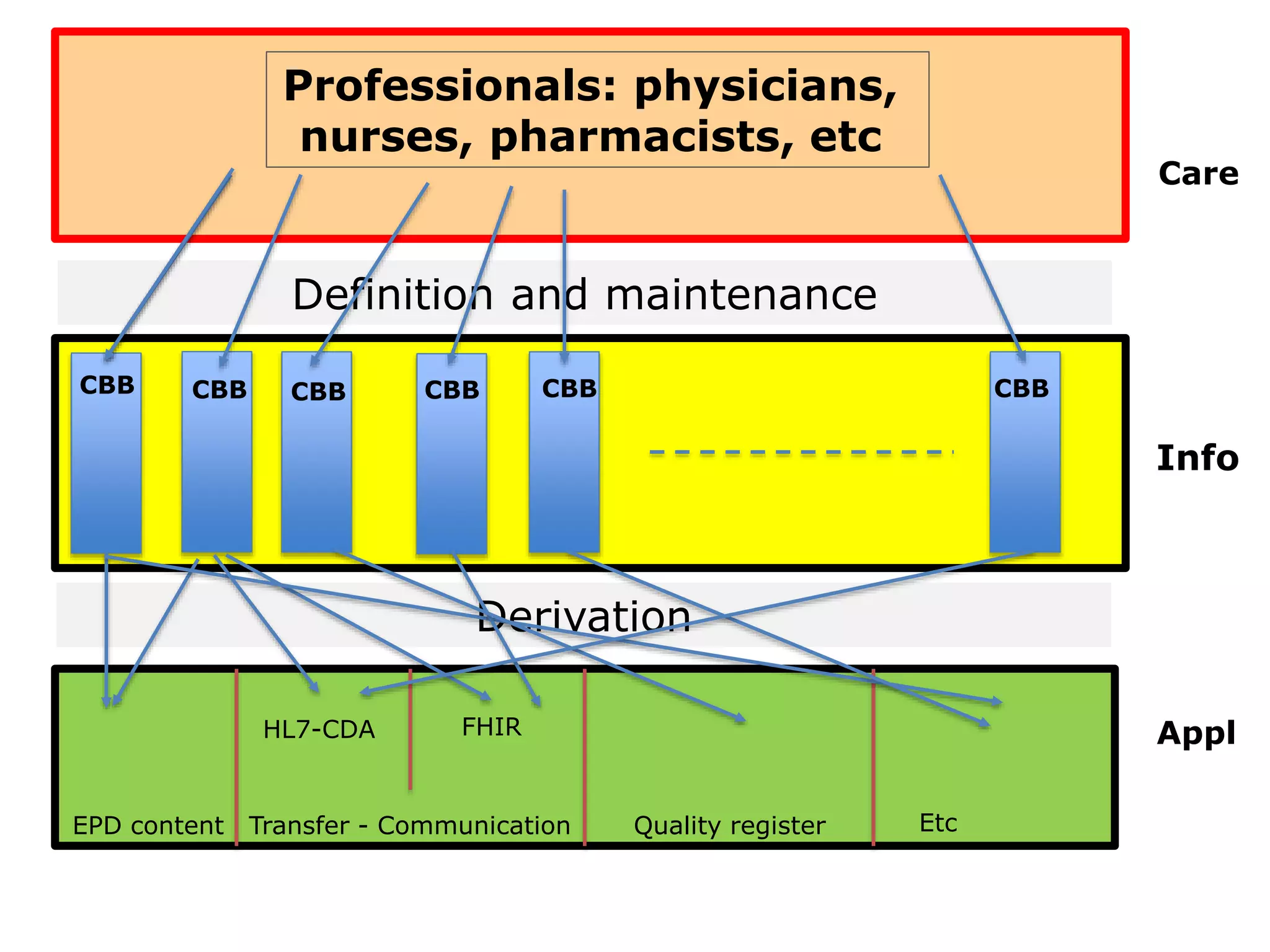
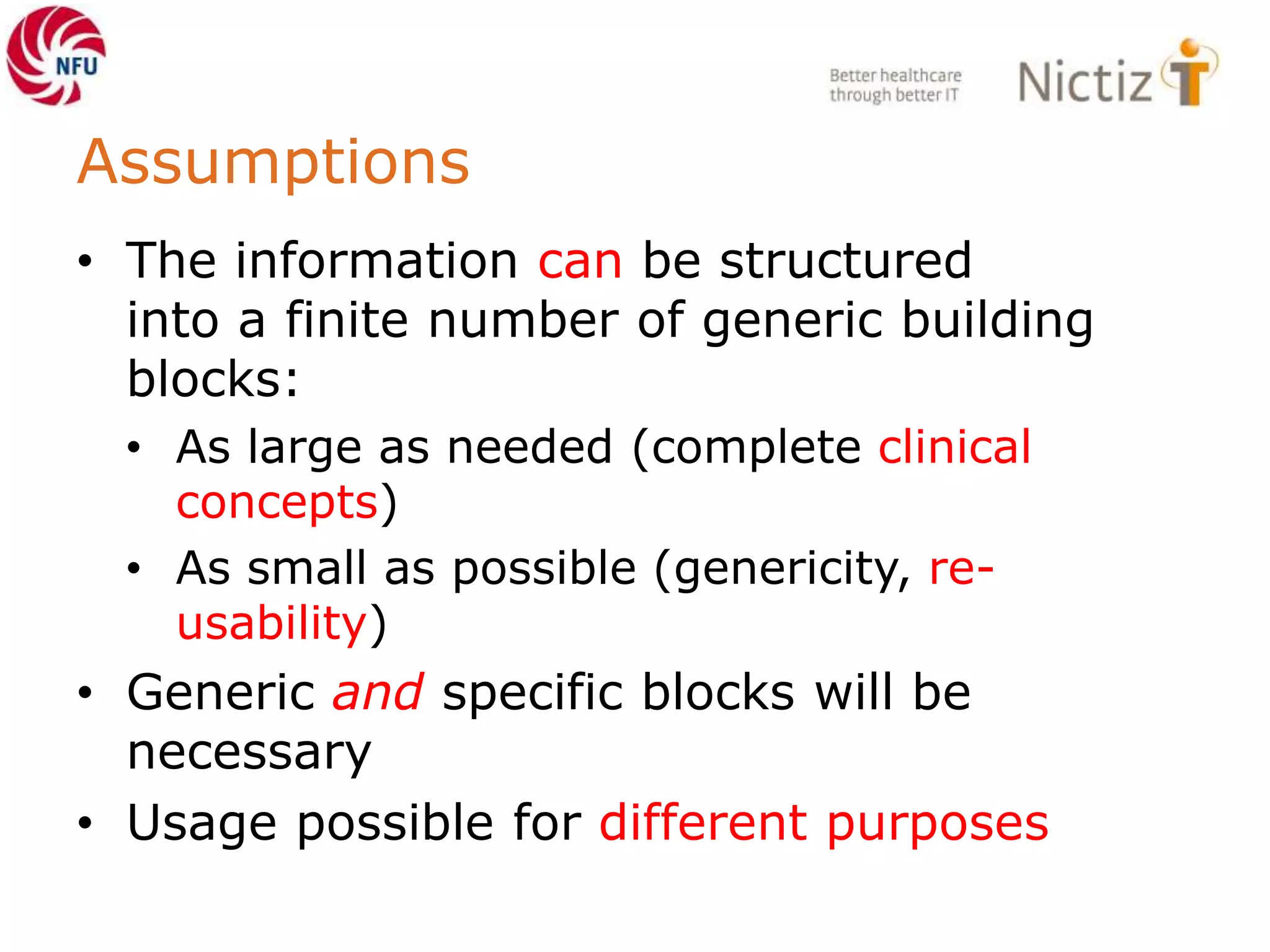
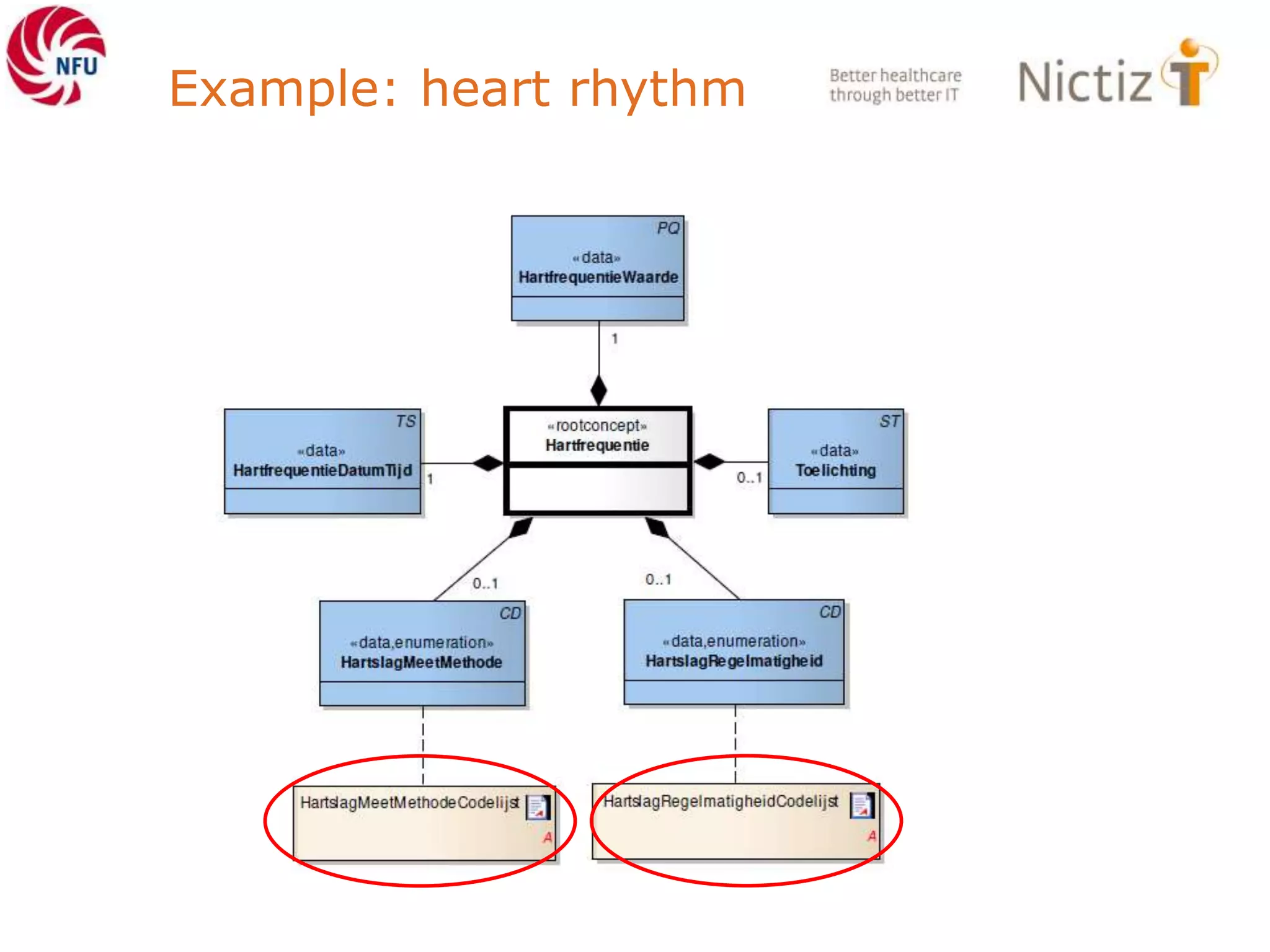

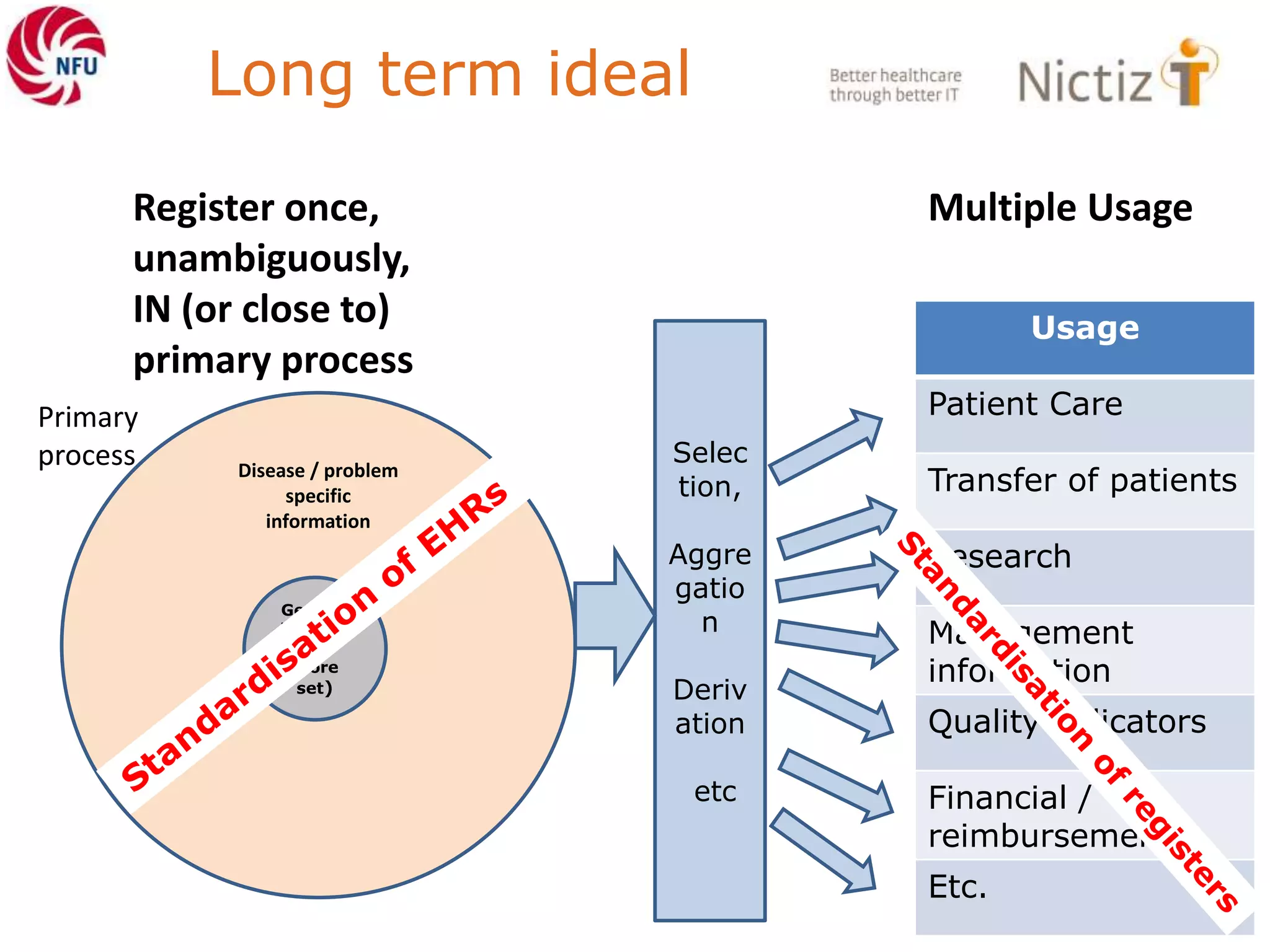



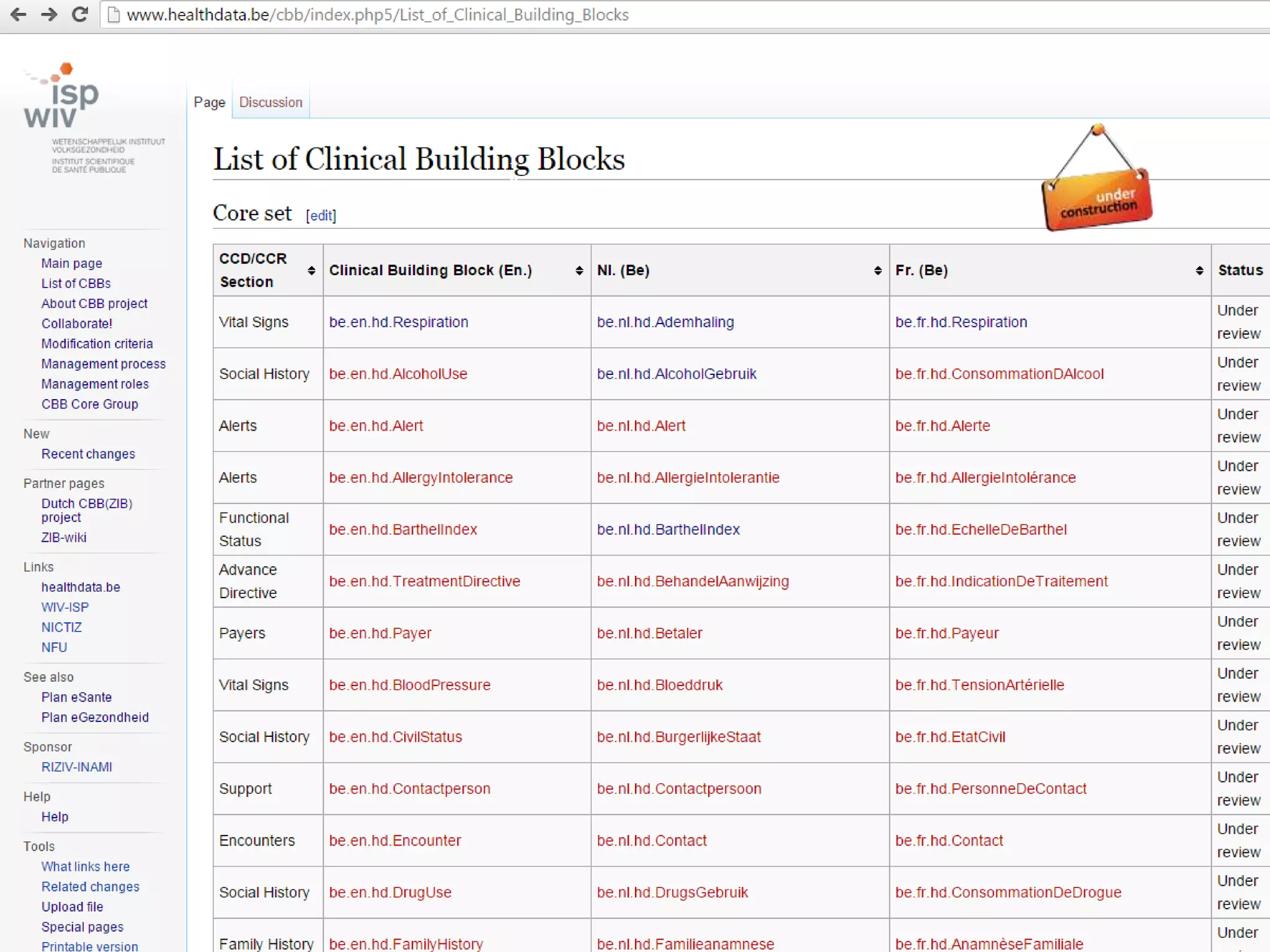




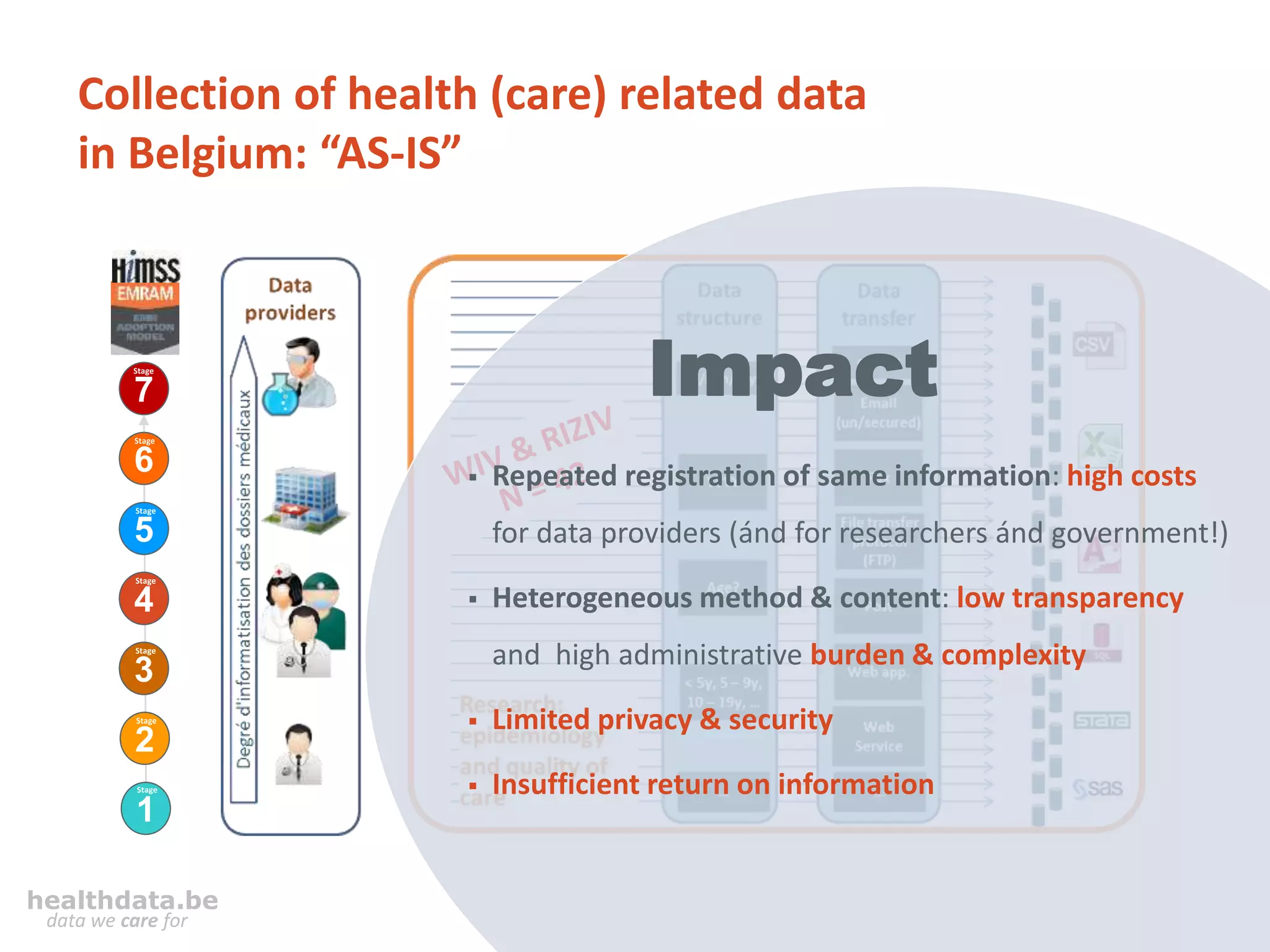
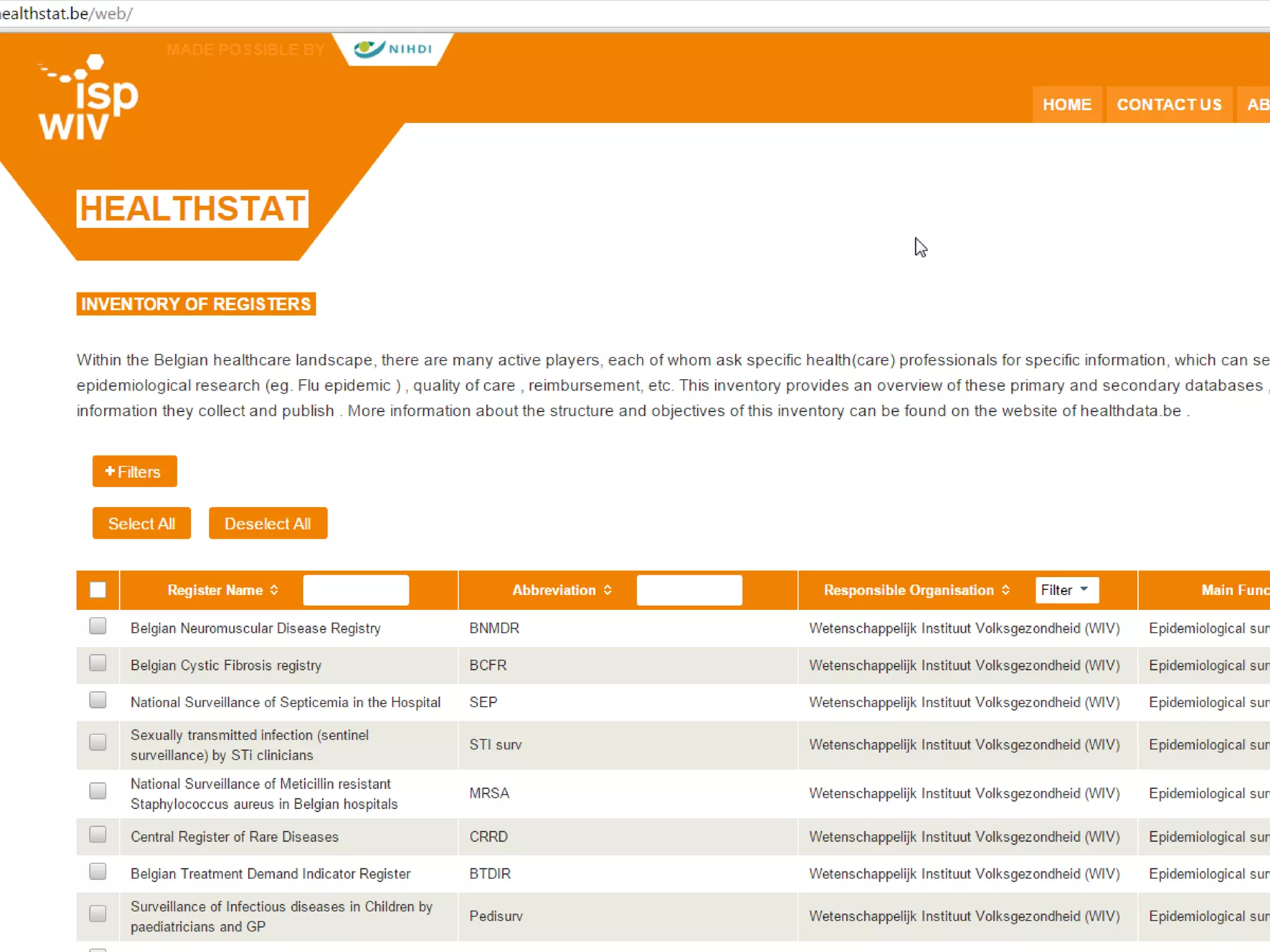
The healthdata.be project aims to improve the collection and management of healthcare data in Belgium by addressing issues such as repeated data registration, low transparency, and privacy concerns. It advocates for a standardization of data using clinical building blocks, which are structured data specifications intended for use across various health domains. The initiative is supported by legal frameworks and collaborative efforts between federal health authorities, healthcare institutions, and IT organizations, with a focus on enhancing public health knowledge and reducing administrative burdens.







































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)














