

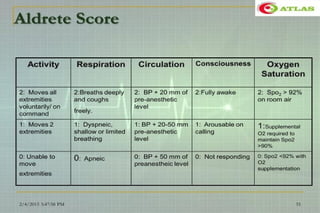
![Scientific Evidence – NON OPIOID ANALGESICS
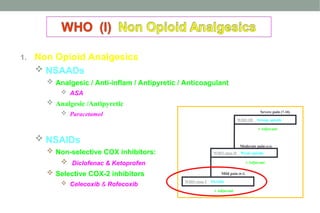
1. Paracetamol:
1. is an effective analgesic for acute pain; the incidence of adverse effects
comparable to placebo (Level I [Cochrane Review]).
2. Paracetamol / NSAIDs given in addition to PCA Opioids Opioid
consumption (Level I).
2. NSAIDs:
1. are effective in the treatment of acute postoperative (Level I ).
2. With careful patient selection and monitoring, the incidence of renal
impairment is low (Level I [Cochrane Review]).
3. NSAIDs + Paracetamol improve analgesia compared with paracetamol
alone (Level I).
Acute Pain Management - Scientific Evidence - AAGBI Guidelines 2010](https://image.slidesharecdn.com/2-250126175633-efcf1fb1/85/2-Postoperative-assessment-and-management-ppt-62-320.jpg)
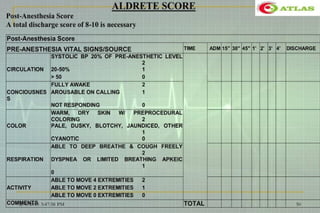
![Scientific Evidence – WEAK
OPIOIDS
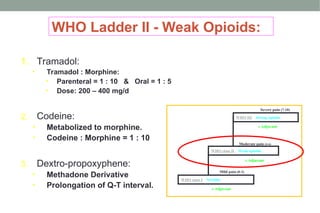
1. Tramadol:
has a lower risk of respiratory depression & impairs GIT motor
function < other opioids
(Level II).
is an effective treatment for neuropathic pain
(Level I [Cochrane Review]).
2. Dextropropoxyphene:
has low analgesic efficacy
(Level I [Cochrane Review]).
Acute Pain Management - Scientific Evidence - AAGBI Guidelines 2010](https://image.slidesharecdn.com/2-250126175633-efcf1fb1/85/2-Postoperative-assessment-and-management-ppt-64-320.jpg)
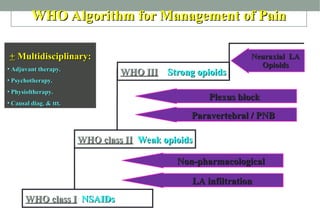
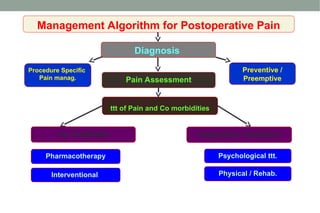

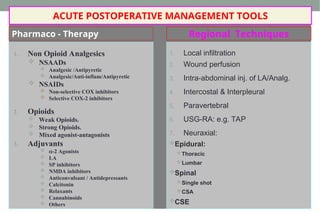
The document outlines postoperative assessment and care, focusing on emergency medical problems, respiratory and hemodynamic issues, and pain management strategies. It details the admission process to the PACU, monitoring parameters, common postoperative complications, and treatments for conditions such as hypotension, hypoventilation, and postoperative nausea and vomiting (PONV). The importance of effective pain management through various methods, including pharmacologic and non-pharmacologic approaches, is also highlighted.














































![The Post anesthesia care unit [PACU] ppt](https://cdn.slidesharecdn.com/ss_thumbnails/postanaesthesiacareunit-240424172213-667289dc-thumbnail.jpg?width=640&height=640&fit=bounds)




















