Download as PDF, PPTX

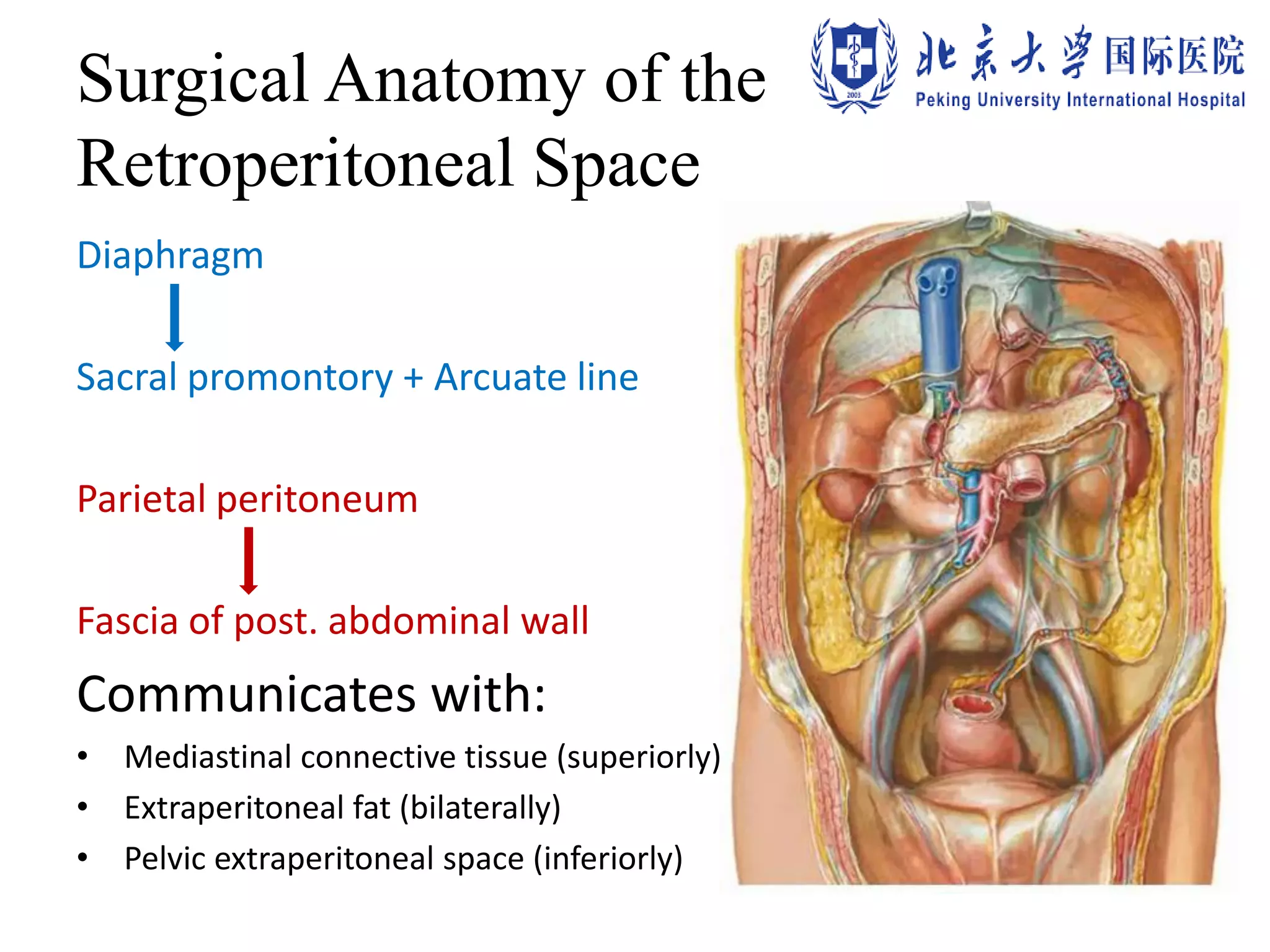

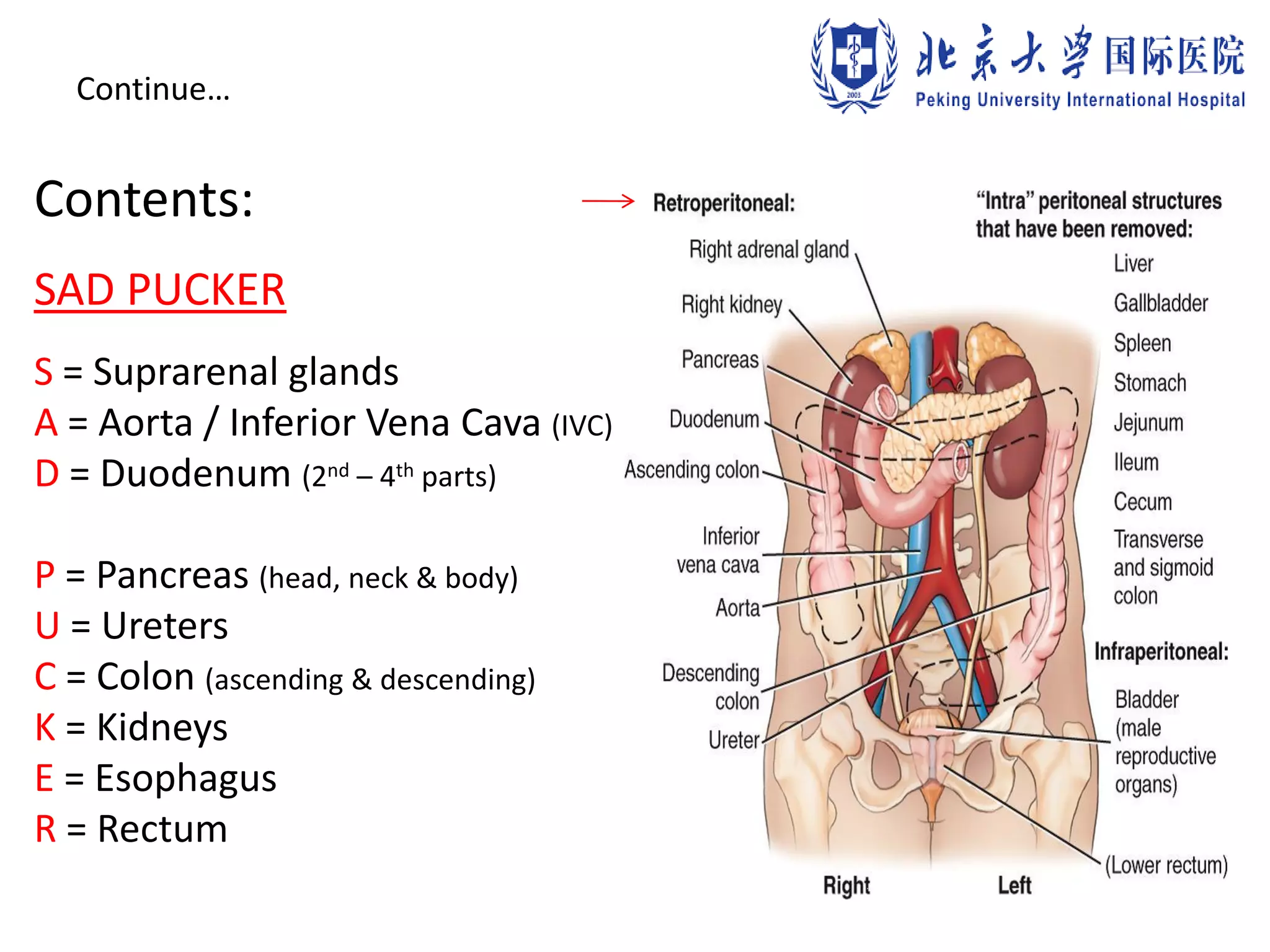





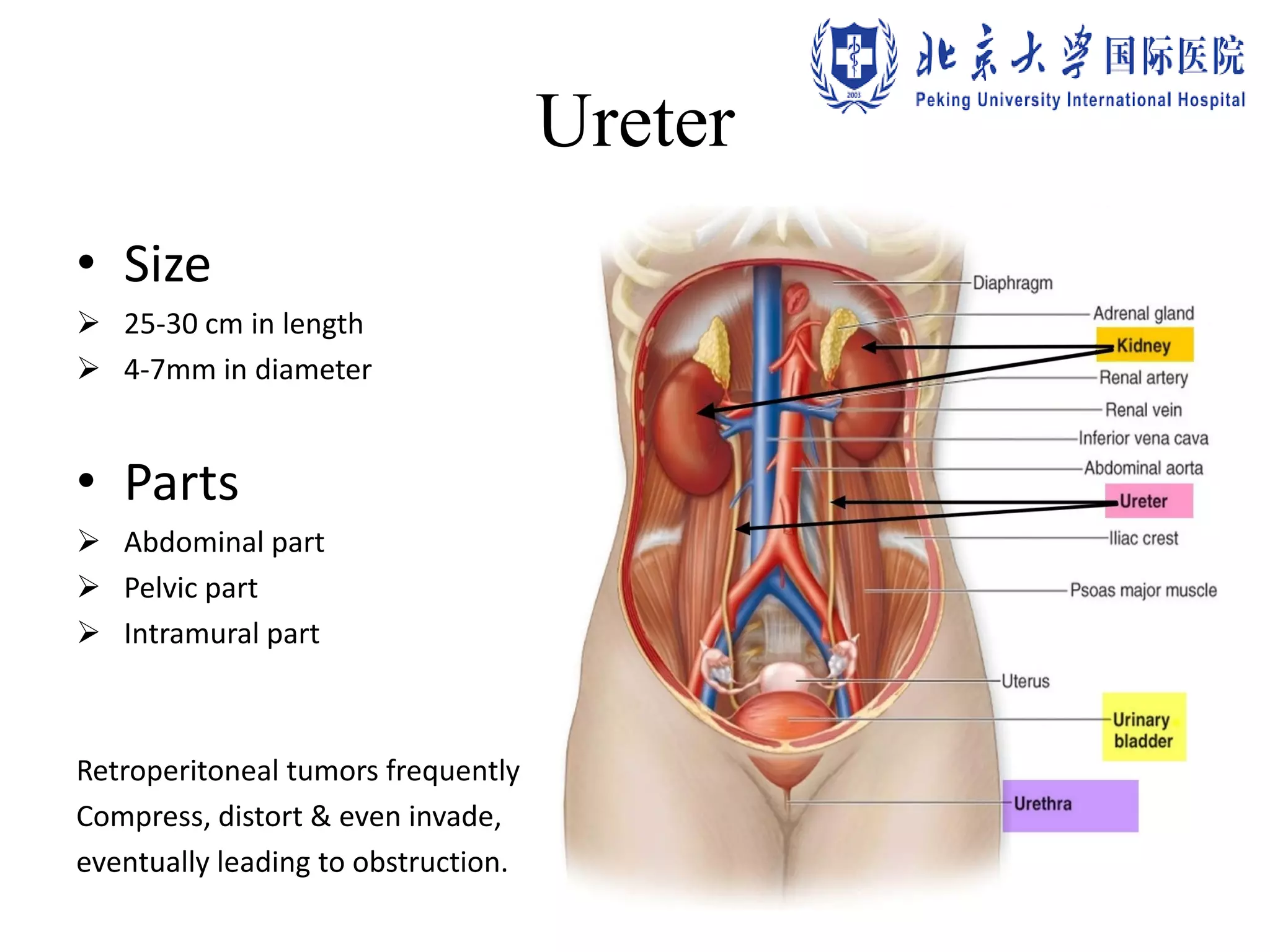
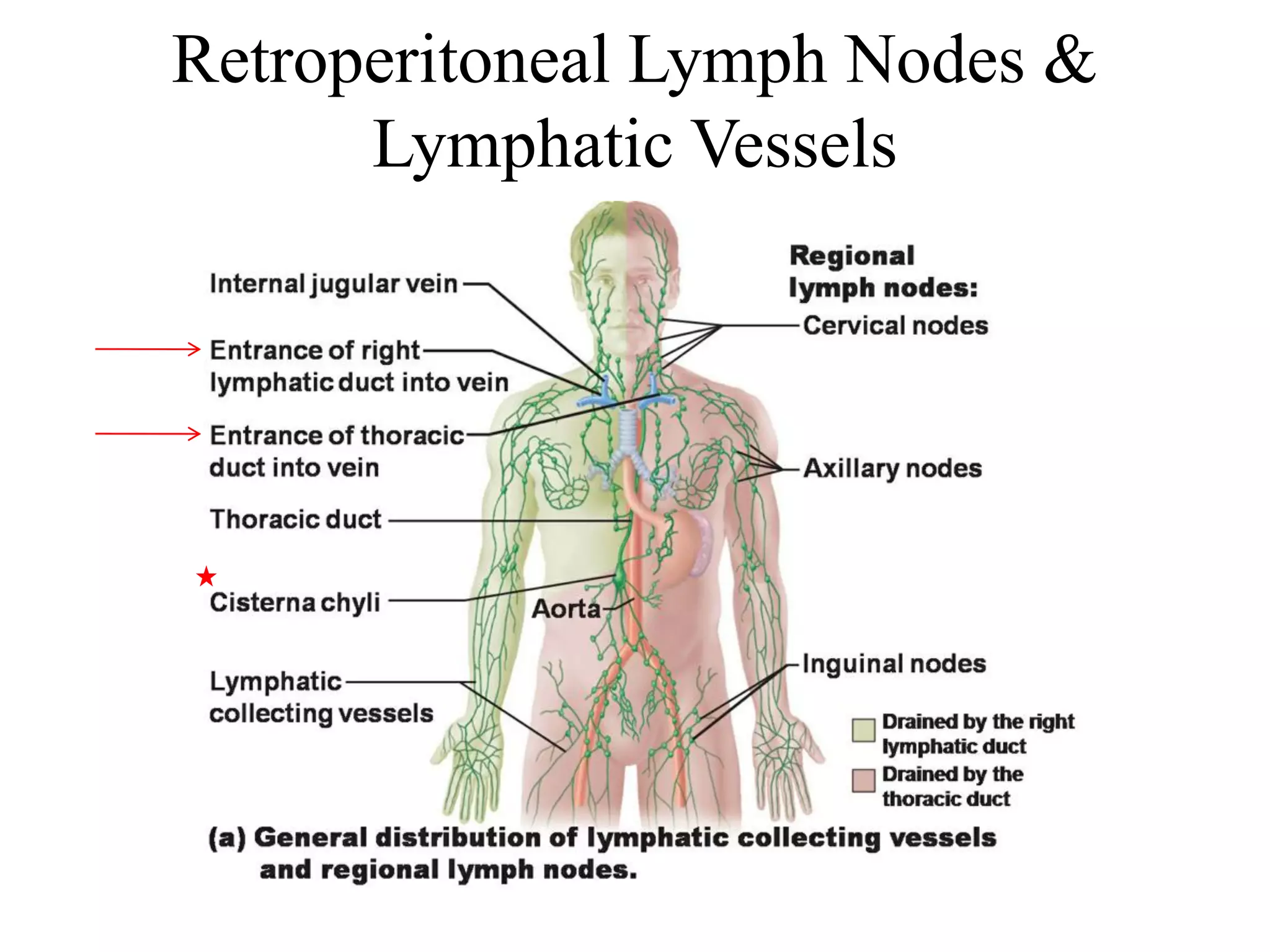
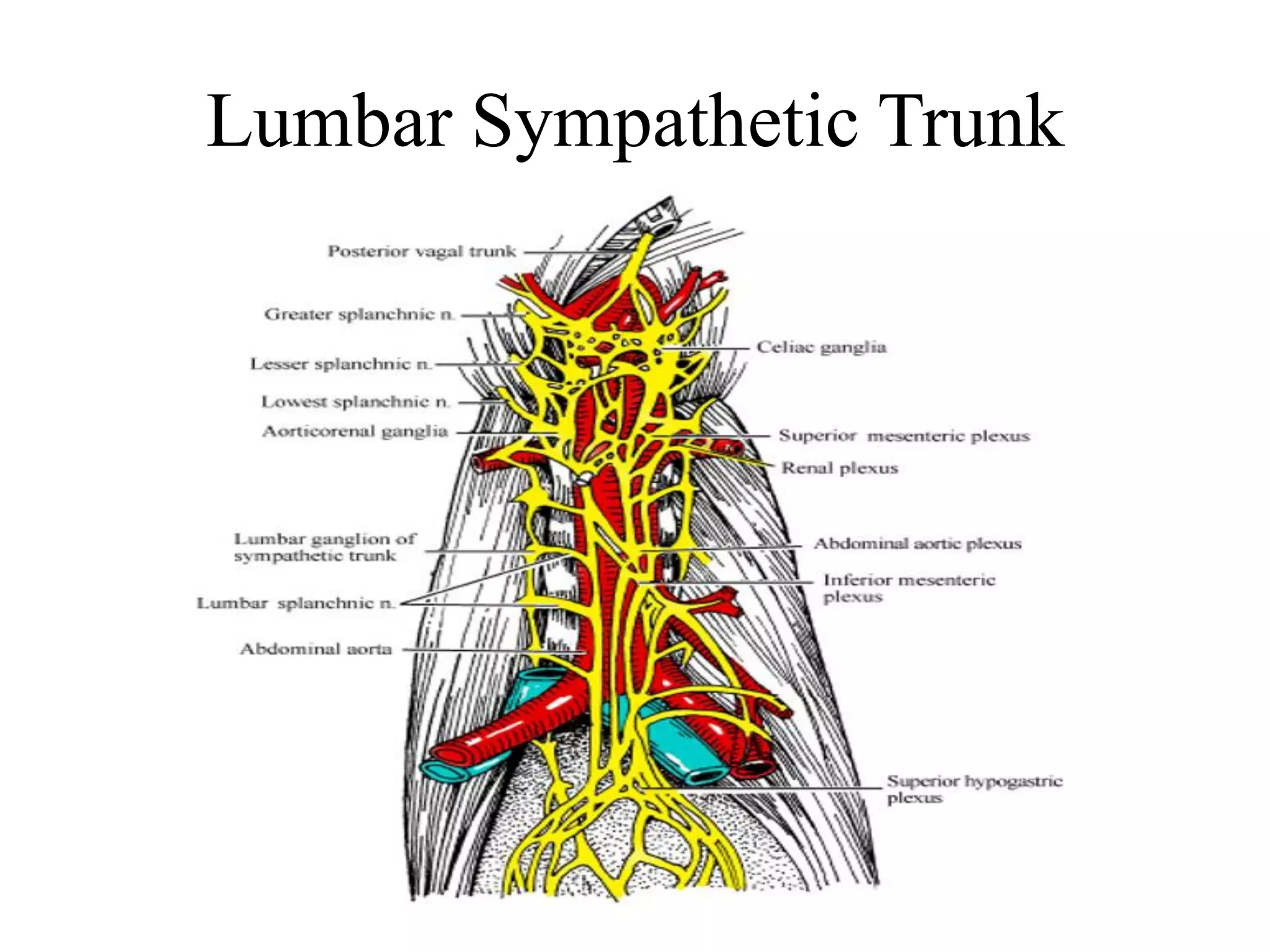
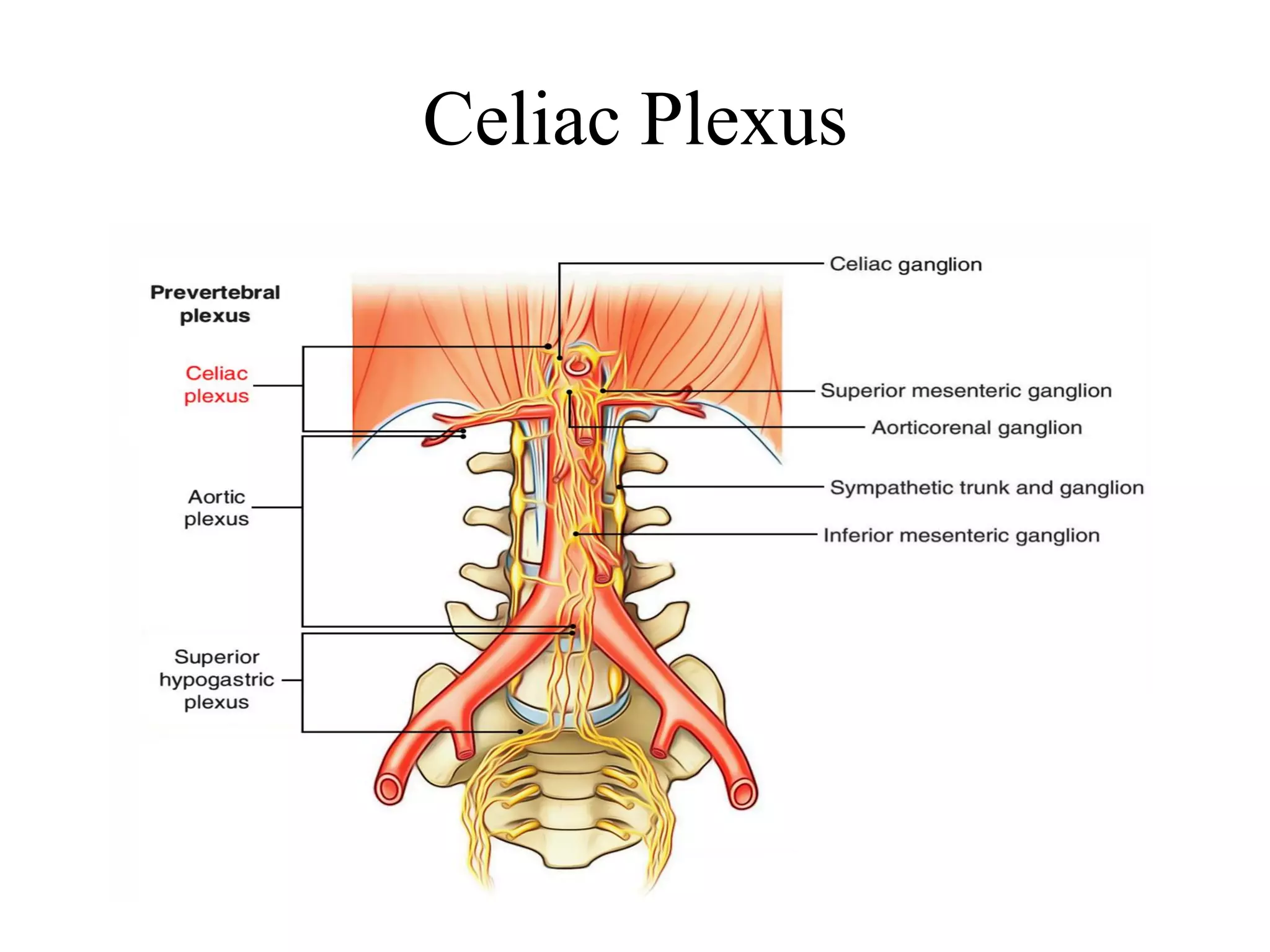
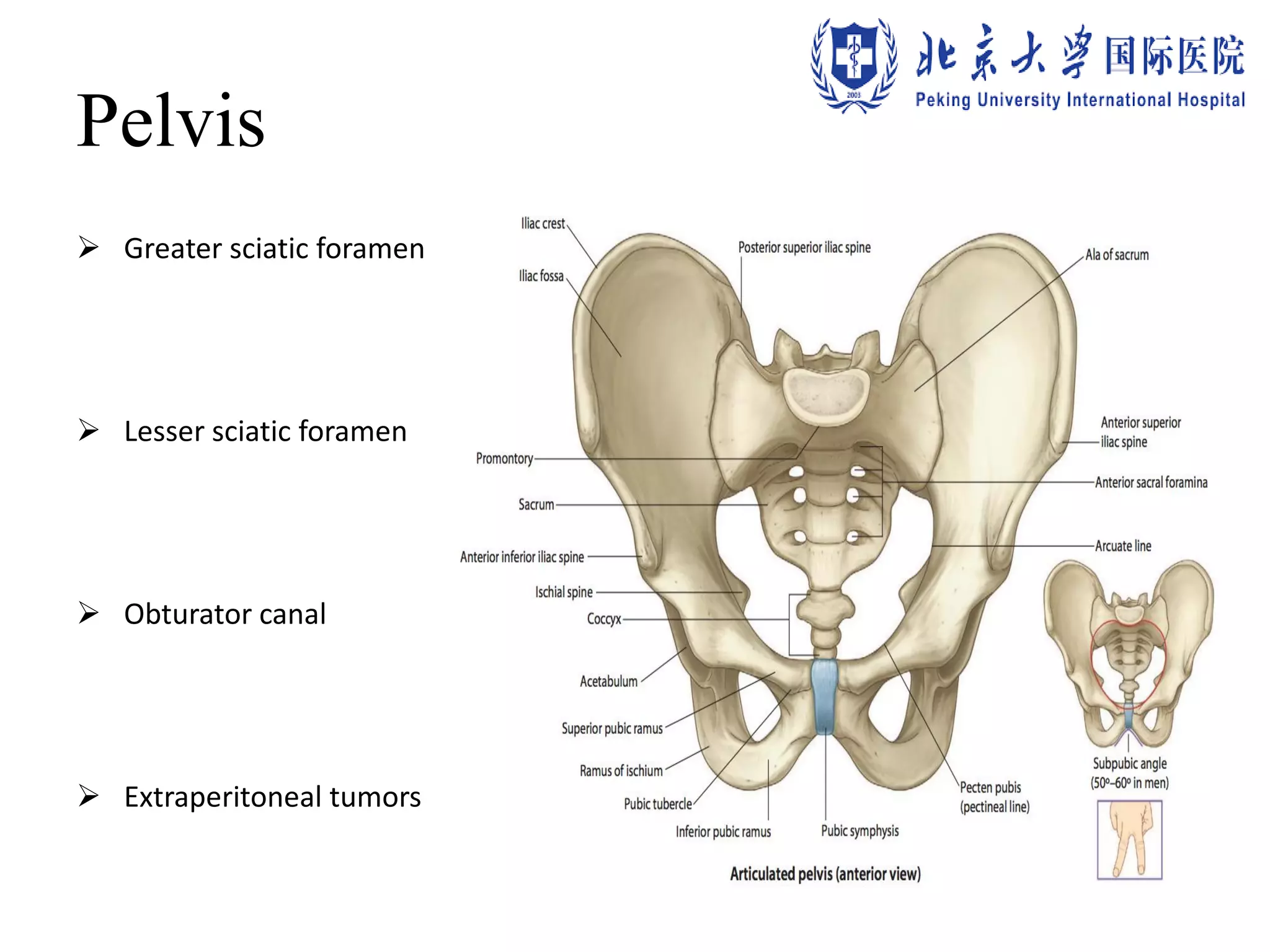









The document provides an overview of the surgical anatomy of the retroperitoneal and pelvic extraperitoneal space, detailing its divisions, contents, and associated structures such as the kidneys, aorta, and suprarenal glands. It highlights the anatomy relevant to potential surgical procedures, including notable features like lymphatic vessels and the impacts of retroperitoneal tumors. Contact information for further inquiry and references for additional information are also included.









































































