3. Introduction
Histoplasmosis sometimes called Darling’s
disease, in honor of the pathologist who first
recognized it in a patient in Panama.
It is present in histiocytes, that is, connective tissue
macrophages, in the RE system, where darling
described a capsule in the stained tissue section.
The apparent capsule has been proven to be an
artifact, caused by the protoplasm of Histoplasma
shrinking away from the cell wall during the
staining process, leaving an unstained area.
4. Histoplasmosis is a systemic
intracellular mycotic disease, mostly of
the reticulo-endothelial system,
manifesting itself in the bone marrow,
lungs, liver, and the spleen caused by
the inhalation of the fungus.
In fact, hepatosplenomegaly is the
primary sign in children, while in
adults, histoplasmosis more
commonly appears as pulmonary
disease.
5. Histoplasmosis also known as:
"Cave disease,"
"Darling's disease,"
"Ohio valley disease,”
"reticuloendotheliosis,"
"spelunker’s lung" and
"caver's disease" is a disease caused by the
fungus Histoplasma capsulatum.
Symptoms of this infection vary greatly, but the
disease affects primarily the lungs.
Occasionally, other organs are affected; this is
called disseminated histoplasmosis, and it can be
fatal if left untreated.
6. Histoplasmosis is common among
AIDS patients because of their
suppressed immunity and
approximately 30% of HIV/AIDS
patients diagnosed with
histoplasmosis die from it.
In immunocompetent individuals, past
infection results in partial protection
against ill effects if reinfected.
7. Types:
Histoplasmosis may be divided into
the following types:
Primary pulmonary histoplasmosis
Progressive disseminated
histoplasmosis
Primary cutaneous histoplasmosis
African histoplasmosis
8. Sources of Histoplasmosis
This is one of the most common fungal infections.
The ecological niche of H. capsulatum is in
blackbird roosts, chicken houses and bat
guano and especially from soil with a high nitrogen
content resulting from deposits of excreta from
chicken, starlings and bats.
Histoplasmosis is a significant occupational
disease in bat caves in Mexico when workers
harvest the guano for fertilizer.
Disruption of soil from excavation or construction
can release infectious elements that are inhaled
and settle into the lung.
9. In the endemic area the majority of patients
who develop histoplasmosis (95%) are
asymptomatic.
5 percent of the cases have chronic
progressive lung disease, chronic
cutaneous or systemic disease or an acute
fulminating fatal systemic disease.
All stages of this disease may mimic
tuberculosis.
The diagnosis is made from their history,
serologic testing or skin test.
10. Epidemiology
Histoplasmosis capsulatum is found
throughout the world.
It is endemic in certain areas of the
United States, particularly in states
bordering the Ohio River valley, the
lower Mississippi River & Missouri
river.
The humidity and acidity patterns of
soil are associated with endemicity.
11. Incidence of histoplasmosis in adults
aged 65 years and older in the U.S. to
be 3.4 cases per 100,000 population.
Rates were highest in the Midwest,
with an estimated 6.1 cases per
100,000 population.
12. Bird and bat droppings in soil promote
growth of Histoplasma.
Contact with such soil aerosolizes the
microconidia, which can infect
humans.
It is also common in caves in southern
and East Africa.
13. Positive histoplasmin skin tests occur
in as many as 90% of the people living
in areas where H. capsulatum is
common, such as the eastern and
central United States.
In Canada, the St. Lawrence River
Valley is the site of the most frequent
infections, with 20-30 percent of the
population testing positive.
14. In the United States, an estimated
60% to 90% of people who live in
areas surrounding the Ohio and
Mississippi River valleys (where
Histoplasma is common in the
environment) have been exposed to
the fungus at some point during their
lifetime.
15. India is another Asian country where
H. capsulatum is known to be
endemic, although the true prevalence
of this mycosis is still
underappreciated.
The first case was reported as early
as 1954, and since then several cases
have been published.
16. In India the majority of histoplasmosis
cases were reported from the eastern
and north-eastern part of the country,
especially from Calcutta (West
Bengal) and Assam.
Interestingly, as observed for the
highly endemic areas in North
America, both states are crossed by
long rivers: the Ganges and the
Brahamaputra, respectively.
17. The Gangetic West Bengal is the site
of most frequent infections, with 9.4
percent of the population testing
positive.
Histoplasma capsulatum was isolated
from the local soil proving endemicity
of histoplasmosis in West Bengal.
18. Systemic Mycoses
Five fungi are included in this group:
Histoplasma capsulatum
Blastomyces dermatitidis
Paracoccidioides barasiliensis
Coccidioides immitis
Cryptococcus neoformans
Four of these pathogens [H. capsulatum, B
dermatitidis, P. barasiliensis and C. immitis] are
dimorphic.
They grow as filamentous molds as saprobes
and in culture at 25 ゚C;
when they infect humans or are cultured at 37 ゚C
, they transform to a unicellular morphology.
19.
20.
21. Life cycle of Histoplasma
Histoplasma spores circulate in the air
after contaminated soil is disturbed.
The spores are too small to see without
a microscope.
When people breathe in the spores, they
are at risk for developing histoplasmosis.
After the spores enter the lungs, the
person’s body temperature allows the
spores to transform into yeast.
The yeast can then travel to lymph
nodes and can spread to other parts of
the body through the bloodstream.
22. Histoplasmosis is not contagious, but is
contracted by inhalation of the spores
from disturbed soil or guano.
The inoculum is represented principally
by microconidia. These are inhaled and
reach the alveoli.
In the alveoli, macrophages ingest these
microconidia.
They survive inside the phagosome.
As the fungus is thermally dimorphic,
these microconidia are transformed into
yeast.
23. They grow and multiply inside the
phagosome. The macrophages travel
in lymphatic circulation and spread the
disease to different organs.
Within the phagosome the fungus has
an absolute requirement for thiamine.
Cell-mediated immunity for
histoplasmosis develops within 2
weeks.
24. If the patient has strong cellular immunity,
macrophages, epithelial cells and
lymphocytes surround the organisms and
contain them, and eventually calcify.
Fibrosis around the cavities in the lung
creates dense , round , flattened areas that
are described as “coin lesions”.
In immunocompromised individuals, the
organisms disseminate to different organs
such as bone, spleen, liver, adrenal glands
and mucocutaneous membranes, resulting in
progressive disseminated histoplasmosis.
Chronic lung disease can manifest.
25.
26.
27. Clinical Features:
Sign & Symptoms:
In the patients who are clinically ill,
histoplasmosis generally occurs in one of
three forms:
acute pulmonary,
chronic pulmonary or
disseminated.
There is generally complete recovery from
the acute pulmonary form (another "flu-like"
illness).
However, if untreated, the disseminated form
of disease is usually fatal.
Patients will first notice shortness of breath
and a cough which becomes productive.
28. If symptoms of histoplasmosis infection
occur, they will start within 3 to 17 days after
exposure; the average is 12–14 days.
Most affected individuals have clinically silent
manifestations and show no apparent ill
effects.
The acute phase of histoplasmosis is
characterized by non-specific respiratory
symptoms, often cough or flu-like.
Chest X-ray findings are normal in 40–70% of
cases.
Chronic histoplasmosis cases can resemble
tuberculosis.
29. The sputum may be purulent or
bloody.
Patients will become anorexic and
lose weight.
Compalin of Fever & chills
Night sweats
Fatigue (extreme tiredness)
Headache & Body aches
Chest pain
30. This again sounds like
tuberculosis, and the lung X-
ray also looks like
tuberculosis, but today
radiologists can distinguish
between these diseases on
the chest film (histoplasmosis
usually appears as bilateral
interstitial infiltrates.)The
skin test is NOT used for
diagnostic purposes,
because it interferes with
serological tests.
31. While histoplasmosis is the most
common cause of mediastinitis, this
remains a relatively rare disease.
Severe infections can cause
hepatosplenomegaly,
lymphadenopathy, and adrenal
enlargement.
Lesions have a tendency to calcify as
they heal.
32. Presumed ocular histoplasmosis
syndrome (POHS) causes
chorioretinitis, where the choroid and
retina of the eyes are scarred,
resulting in a loss of vision not unlike
macular degeneration.
Despite its name, the relationship to
Histoplasma is controversial.
Distinct from POHS, acute ocular
histoplasmosis may rarely occur in
immunodeficiency.
33. Skin lesion on the upper lip due to Histoplasma
capsulatum infection.
34.
35. Laboratory Diagnosis:
To diagnose histoplasmosis :
medical and travel history,
Sign & symptoms,
physical examinations, and
laboratory tests
36. Specimens:
Clinical specimens sent to the lab
depend on the presentation of the
disease:
Sputum or Bronchial alveolar lavage,
if it is pulmonary disease, or
Skin scrappings from the edges of
ulcer.
Biopsy material from the diseased
organ.
Aspirated Pus from lymphnodes &
subcutaneous abscess
Bone marrow is an excellent source
of the fungus, which tends to grow in
37. Peripheral blood is also a source of
visualizing the organism histologically.
The yeast is usually found in monocytes or
in PMN's.
In peripheral blood, H. capsulatum appears
as a small yeast about 5-6 µ in diameter.
(Blastomyces is 12 to 15 µ).
Gastric washings are also a source of H.
capsulatum as people with pulmonary
disease produce sputum and frequently
swallow their sputum.
Cerebrospinal Fluid and Urine for culture.
38. Direct Examination:
H.capsulatum is most likely to be found within
cells instead of free in fluid.
Staining by :
Wright’s method ,
The Giemsa stain, or
Calcofluor white
Special stains: Papanicolaou stain or H & E stain
for tissue specimen.
Mucus and other thick substances should be
treated with N-acetyl-L-cysteine before the wet
mount is prepared.
KOH wet mount prepared from clinical samples
shows tiny yeast cells.
39. Mycology
Culture Media:
Blood agar or Modified SDA with antimicrobials and
actidione
BHIA containing 6% Blood are strongly
recommended for specimens from sites that are
ordinarly sterile
Yeast extract phosphate agar with ammonium
hydroxide : can be inoculated from the specimen to
encourage conidiation and inhibit Candida
species.
Potato dextrose agar : to encourage conidia
production
All cultures should be examined daily for 1 week,
40. When it is grown on Modified
Sabouraud dextrose agar with
antimicrobials at 25ºC, it appears as a
white, cottony mycelium after 2 to 3
weeks.
Later they become woolly , as aerial
hyphae develop.
The mold phase of H. capsulatum is
characterized by thin, branching,
septate hyphae, 1-2 µm, that produce
microconidia(2-5µm).
41. Macroconidia develop directly on the
hyphae or on short, slender conidiophores
that develop at right angles to vegetative
hyphae.
The macroconidia are hyaline, unicellular,
and relatively large 8-14 µm, spherical to
pyriform shape.
As the macroconidia age, they become
tuberculate macroconidium, they form
finger like extensions of the thick wall of
conidium.
Mature macroconidia sometimes described
42.
43. Grown at 37ºC the budding yeast form
appears after 10-15 days . It is a white to tan
and mucoid colony, with rough membranous
texture.
The yeast cell is 5-6 µ in diameter and slightly
oval in shape and found exclusively within
macrophages.
To confirm the diagnosis, one must convert
the organism from mycelium to yeastor or
use the DNA probe.
Primary cultures for H.capsulatum should be
held for 10-12 weeks before being dscarded
as No Growth.
44.
45. 325
325. Culture of Histoplasma capsulatum on Sabouraud's dextrose
agar showing a white suede-like colony with a pale yellow-brown
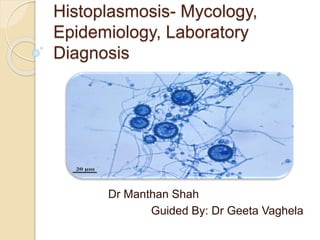
46. 327
Microscopic morphology of the saprophytic or mycelial form
of Histoplasma capsulatum showing characteristic large,
rounded, single-celled, tuberculate macroconidia formed on
short, hyaline, undifferentiated conidiophores.
50. Serological Test
Serology for histoplasmosis is a little
more complicated than for other
mycoses, but it provides more
information than blastomycosis serology.
There are 4 tests:
• Latex agglutination
• Complement Fixation
• Immunodiffusion
• EIA
51. Each of these serological tests has
different characteristics that make them
useful.
The latex agglutination test is a very
simple test involving agglutination in a
test tube by using latex particles coated
with Histoplasmin as an antigen.
This screening test should always be
confirmed by another methods.
Disadvantage: many false positive tests
have been reported.
52. Antibody Detection for
H.capsulatum
Detection of antibodies to Histoplasma
provides additional laboratory
evidence of disease when used
alongside other laboratory findings
and clinical presentation.
53. Immunodiffusion Assay:
The Histoplasma immunodiffusion assay
utilizes 2 different antigens, the H and
the M proteins, and we can therefore
detect up to 2 different precipitating
bands in the agar plate.
Antibodies to the M antigen, appear
shortly following exposure and can
remain detectable by immunodiffusion
for up to 3 years following disease
resolution.
Therefore, presence of the M band
alone cannot be used to discriminate
between acute or remote infection.
54. On the other hand, the presence of an H
band either alone or in combination with the
M band is indicative of active or recent
histoplasmosis because H band of the
immunodiffusion test is usually present for
only 4 to 6 weeks after exposure
Importantly, a negative immunodiffusion
result should not be used to exclude
histoplasmosis as the specimen may have
been collected early following exposure and
prior to the development of detectable
precipitating antibodies.
Specificity >95% & variable Sensitivity 80-
100 %
55.
56.
57. Complement Fixation Test:
Alongside immunodiffusion, there is
also Histoplasma complement fixation
testing.
Briefly, complement fixation assays
are based on the ability of antibody-
antigen complexes, formed between
antibodies present in the patient
sample and added fungal antigens, to
fix and inactivate exogenously added
complement.
58. Sensitized RBCs are added to this mix and
since the complement pathway is inactivated,
the red blood cells will remain intact and
settle to the bottom of the well as a compact
pellet, indicative of a positive reaction and the
presence of specific antibodies.
In the absence of patient antibodies however,
the added complement will remain active and
lead to lysis of the sensitized red blood cells.
Therefore, the presence of lysis is indicative
of a negative reaction and the absence of
specific antibodies.
59.
60. The Histoplasma complement fixation
assay is performed using 2 different
Histoplasma antigens, one purified from
the yeast phase and the second purified
from the mycelial phase of growth.
Serial dilution of patient samples, allows
us to determine an endpoint titer which
can be used to guide diagnosis.
For either antigen, serially increasing
titers or an endpoint titer greater than or
equal to 1:32 is associated with the
presence of active histoplasmosis.
61. A titer of 1:8 or 1:16 is considered positive,
but only presumptive evidence of infection
and additional clinical correlation is
necessary.
Titers less than 1:8 are not considered to be
significant and therefore are not reported.
Importantly, low-level titers may be detected
in individuals who reside in endemic areas
and are otherwise healthy.
Finally, declining complement fixation titers
over months to years have been associated
with disease resolution, but should not be
used to monitor response to therapy.
62. The complement fixation assay has a
higher sensitivity for histoplasmosis as
compared to immunodiffusion assays,
particularly during early disease,
however their specificity is lower and for
this reason complement fixation and
immunodiffusion are performed
concurrently.
Also these assays are fairly labor
intensive with long incubation times
which leads to an average turnaround
63. One disadvantage is that complement
fixing antibody develops late in the
disease, about 2 to 3 weeks after onset.
A second disadvantage is that it cross
reacts with other mycotic infections like
blastomycosis, paracoccidioidomycosis .
An advantage of the C-F test is that it is
quantitative, so the physician can follow
the course of the disease by observing
the titer of several samples.
64. PCR Assays
A real-time PCR assay that correctly
identified H. capsulatum from among a
variety of fungi grown in the laboratory
appears promising.
Using this assay, positive identification of H.
capsulatum was shown in tissue biopsies and
bronchoalveolar lavage fluid from patients
who had documented histoplasmosis .
Two different seminested PCR assays have
also shown promise when applied to blood
and tissue scrapings obtained from patients
with histoplasmosis and mice experimentally
infected with H. capsulatum .
65. Radioimmunoassay:
Recently, a Radioimmunoassay can
be used to measure H. capsulatum
polysaccharide antigen (HPA) levels in
samples of a patient's urine, serum,
and other body fluids.
The test appears to meet the
important need for a rapid and
accurate method for early diagnosis of
disseminated histoplasmosis,
especially in patients with AIDS.
66. HPA is detected in body fluid samples
of most patients with disseminated
infection.
The antigen cross reacts with
Coccidioides immitis & Blastomyces
dermatidis.
High Sensitivity & Low specificity , so
should be confirmed by another
method.
67. 332
332. Immy exoantigen immunodiffusion test kit for the
identification of Histoplasma capsulatum, Coccidioides
immitis and Blastomyces dermatitidis.
68. 333
333. Exoantigen immunodiffusion plate showing positive
identification of Histoplasma capsulatum. Note H and M bands
of identification; EX = culture filtrate; H = Histoplasma antibody
and antigen, C = Coccidioides antibody and antigen; B =
69. These days, H.capsulatum
AccuProbe (GEN-PROBE, Inc. San
Diego, California ), a probe that
recognizes specific rDNA target
sequence, is commonly used for more
rapid & accurate results.
The Lysis centrifugation technique
is most effective method of
recognizing H.capsulatum from blood
specimen.
70. Histoplasmin skin test
A person can learn from a
histoplasmin skin test whether he or
she has been previously infected by
H. capsulatum.
This test, similar to a tuberculin skin
test like delayed type hypersensitivity.
Skin test with intradermal injection of
0.1ml of Histoplasmin antigen , a
culture filtrate of the mycelial phase of
growth, in forearm.
It is useful as epidemiological tool.
71. A histoplasmin skin test becomes
positive 2 to 4 weeks after a person is
infected by H. capsulatum.
The test is positive after 48 hours with
an induration of 5mm.
a positive skin test does not mean that a
person is completely protected against ill
effects, it indicates either present or past
exposure to H.capsulatum.
A previous infection by H. capsulatum
can provide partial protection against ill
effects if a person is reinfected.
72. Animal Pathogenicity:
Dogs, guinea pigs, hamsters, rabbits,
mouse.
Mouse is an ideal laboratory animal
for isolation of H.capsulatum.
Mycelial & yeast forms can be
inoculated to establish systemic
infection .
Due to discovery of newer methods
,its frequency of usage has
decreased.
73. Treatment
For some people, the symptoms of
histoplasmosis will go away without
treatment.
However, prescription antifungal medication
is needed to treat severe histoplasmosis in
the lungs, chronic histoplasmosis, and
infections that have spread from the lungs to
other parts of the body (disseminated
histoplasmosis).
The drug of choice (DOC) is amphotericin B,
with all its side effects.
Itraconazole and Voriconazole is now also
being used.
74. Liposomal preparations of
amphotericin B are more effective
than deoxycholate preparations.
The liposomal preparation is preferred
in patients that might be at risk of
nephrotoxicity, although all
preparations of amphotericin B have
risk of nephrotoxcity.
Individuals taking amphotericin B are
monitored for renal function.
75. Treatment with itraconazole 400mg
daily will need to continue for at least
a year in severe cases, while in acute
pulmonary histoplasmosis, 6 to 12
weeks treatment is sufficient.
Alternatives to itraconazole are
posaconazole, voriconazole, and
fluconazole.
Individuals taking itraconazole are
monitored for hepatic function.
76. Differential Diagnosis:
Tuberculosis
Localized pneumonitis is mistaken for:
Mycoplasma pneumoniae
Legionella
Coxiella burnetii
Chlamydia pneumoniae
The uninucleate yeasts should be distinguished
from other intracellular organisms like :
Leishmania donovani ( contain kinetoplast) ,
Toxoplasma gondii (tachyzoites being protozoa
are not stained with GMS stain) ,
Penicillium marneffei (dividing transverse fission
cells),
Cryptococcus neoformans (capsulated) .
Candida glabrata (never found intracellularly)
77. How can we prevent
histoplasmosis?
It can be difficult to avoid breathing in Histoplasma
in areas where it’s common in the environment.
In areas where Histoplasma is known to live,
people who have weakened immune systems (for
example, by HIV/AIDS, an organ transplant, or
medications such as corticosteroids or TNF-
inhibitors) should avoid doing activities that are
known to be associated with getting
histoplasmosis, including:
Disturbing material (for example, digging in soil or
chopping wood) where there are bird or bat
droppings
Cleaning chicken coops
Exploring caves
78. Is histoplasmosis
contagious?
No. Histoplasmosis can’t spread from
the lungs between people or between
people and animals. However, in
extremely rare cases, the infection
can be passed through an organ
transplant with an infected organ.
79. If someone had already had
histoplasmosis, could they get it again?
It’s possible for someone who’s
already had histoplasmosis to get it
again, but the body’s immune system
usually provides some partial
protection so that the infection is less
severe the second time.
In people who have weakened
immune systems, histoplasmosis can
remain hidden in the body for months
or years and then cause symptoms
later (also called a relapse of infection)
80. Any types of queries regarding
diagnostic problems can be sent to
Histoplasmosis Reference
Laboratory (HRL) , Indianapolis,
USA.
81. 322
322. Histoplasmosis of the lower gum showing ulcer around
base of tooth. Tissue section stained with haematoxylin and
eosin (H&E) from a biopsy of the mouth lesion shown in slide.
82. 323
323. Note macrophages containing numerous yeast cells of
Histoplasma capsulatum. The basophilic cytoplasm of the
fungal cells is retracted from the poorly stained cell wall,
giving the false impression of a capsule. (Courtesy Dr G.
83. 324
324. Tissue section stained by Grocott's methenamine silver
(GMS) from a lung biopsy showing numerous yeast cells of
Histoplasma capsulatum inside macrophages.
84. 329
329. Microscopic morphology of the parasitic or yeast form of
Histoplasma capsulatum cultured on brain heart infusion agar
containing blood incubated at 37oC. Note the small round to
oval budding yeast-like cells.
85. 330
330. Tissue section stained by Periodic Acid-Schiff (PAS)
showing numerous yeast cells of Histoplasma capsulatum var.
duboisii. This African variant differs by having larger (7-15um)
budding yeast cells in vivo.
86. 331
331. Tissue section stained by Grocott’s methenamine silver
(GMS) showing numerous yeast cells of Histoplasma
capsulatum var. duboisii. This African variant differs by having
larger (7-15um) budding yeast cells in vivo.
87. References:
Fundamentals of Diagnostic Mycology: Fran Fisher
& Norma B. Cook - Chapter 8 Systemic fungi –
Histoplasmosis Page no. 247-250
Textbook of Medical Mycology- 3rd Edition –Jagdish
Chander : Chapter 16- Histoplasmosis pg no. 210-
220.
A Guide to Serologic Testing for Select Fungi -
Mayo Medical Laboratories
(http://www.mayomedicallaboratories.com/articles/
hot-topic/2014/05-15-serologic-testing-
fungi/index.html )
Detection of Histoplasma capsulatum DNA in
human samples by real-time polymerase chain
reaction. - PubMed – NCBI
88. Histoplasmosis: a Clinical and Laboratory Update
(http://cmr.asm.org/content/20/1/115.full )
Histoplasmosis | Types of Diseases | Fungal
Diseases | CDC
(http://www.cdc.gov/fungal/diseases/histoplasmosis
/ )
Histoplasmosis: Read About Diagnosis, Treatment
and Symptoms
(http://www.medicinenet.com/histoplasmosis_facts/
article.htm )
Textbook of Microbiology Ananthanarayan &
Paniker -9th Edition Chapter 64 – Systemic &
Opportunistic Mycoses :Histoplasmosis pg no.
607-608