Download as PDF, PPTX

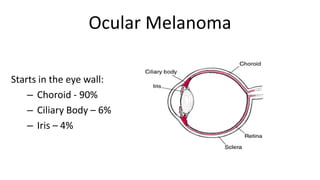

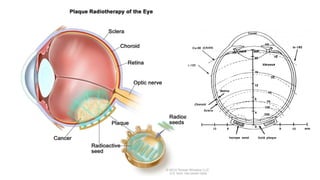
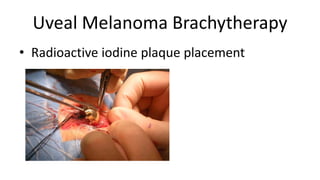








Dr. Peter G. Hovland discusses ocular melanoma, a rare eye cancer that affects around 2,000 people in the U.S. each year, primarily in Caucasians with lighter eye colors. Treatment options include radiation, laser therapy, and enucleation, with ongoing research into new therapies such as clinical trials for alternative treatments. The presentation emphasizes the importance of personalized patient care and a supportive healthcare team throughout the patient's journey.