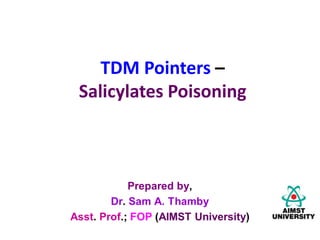
![ Salicylate poisoning is mainly due to ingestion of…
• Aspirin [10-20 g (adults); 3g (children)], or
• LMS (1 ml of 25% LMS = 300 mg salicylate)
Pathophysiology:
SALICYLATES
Stimulate resp.
centre
Hyperpnoea
(hyperventilation)
Hypocarbia
(Hypocapnoea)
↓ed CO2;
↑ed HCO3
-
↑ed pH
Respiratory
Alkalosis
Body compensates:
Excretes HCO3
-, Na+,
Ca2+; BUT…
Retains Cl-
Hypokalemia and
dehydration](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Recommended
More Related Content
What's hot
What's hot (20)
Similar to TDM Pointers - Salicylates & Paracetamol Poisoning.pdf
Similar to TDM Pointers - Salicylates & Paracetamol Poisoning.pdf (20)
More from samthamby79
More from samthamby79 (20)
Recently uploaded
Recently uploaded (20)
TDM Pointers - Salicylates & Paracetamol Poisoning.pdf
- 1. TDM Pointers – Salicylates Poisoning
- 2. Salicylate poisoning is mainly due to ingestion of… • Aspirin [10-20 g (adults); 3g (children)], or • LMS (1 ml of 25% LMS = 300 mg salicylate) Pathophysiology: SALICYLATES Stimulate resp. centre Hyperpnoea (hyperventilation) Hypocarbia (Hypocapnoea) ↓ed CO2; ↑ed HCO3 - ↑ed pH Respiratory Alkalosis Body compensates: Excretes HCO3 -, Na+, Ca2+; BUT… Retains Cl- Hypokalemia and dehydration
- 3. Hypokalemia (mild toxicity); Hyperkalemia (severe toxicity); Stimulate metabolism (generally) causing Hyperthermia. Damage hepatocytes Renal dysfunction; ↑ed plasma enzyme activity; ↑ed PT time; ↓ed platelet aggregation; Interferes w/ Carbohydrates metabolism ↑ed conc. of lactic acid, ketones and inorganic acids HAGMA: Due to ↑ed conc. of acid in the body Anion Gap; High Anion Gap; Delta Ratio; AG formula
- 4. Clinical Features Mild Poisoning: • Tachycardia; Hyperpnoea; Respiratory Alkalosis • Tinnitus • Alkaline Urine ( pH > 6) Severe Poisoning: • Convulsions; Coma; • Respiratory and Cardiac Failure; Cerebral and pulmonary oedema • AKI; Acidosis;
- 5. Salicylates are weak acids that cross cell membranes relatively easily (they are more toxic when blood pH is low). Dehydration, hyperthermia, and chronic ingestion increase salicylate toxicity because they result in greater distribution of salicylates to tissues. Excretion of salicylates increases when urine pH increases.
- 6. Suspect Salicylate poisoning if patients present with any of the following H/o a single acute overdose Repeated ingestions of therapeutic doses Unexplained metabolic acidosis Unexplained confusion and fever (in elderly patients) Other findings compatible with sepsis (fever, hypoxia, non-cardiogenic pulmonary oedema, dehydration, hypotension)
- 7. The symptoms of acute salicylate poisoning may be minimal initially with severe toxicity not evident until 6-12 hours. There is a poor correlation between salicylate concentration and toxicity (Organs and systems deterioration may still occur with falling serum concentrations due to rising CNS concentration). In moderate to severe salicylate poisoning, consider decontamination (activated charcoal) and the early enhancement of elimination (urinary alkalization with or without haemodialysis).
- 8. SALICYLATE DOSAGE CLINICAL EFFECTS <150mg/kg Minimal symptoms 150-300mg/kg Mild-moderate symptoms: Tinnitus, vomiting, hyperventilation >300mg/kg Severe symptoms: Acidosis, seizures, hyperthermia
- 9. Ix: Positive Ferric Chloride test (blood or urine sample) Blood salicylate levels: • 50-110 mg/dl 6-hrs post-ingestion (mild-moderate intoxication); • >110 mg/dl 6-hrs post-ingestion (severe intoxication; often fatal); Elevated Hct, WBC count, platelet count; Hypo- and Hyper- natremia; kalemia; Hypoglycemia Respiratory alkalosis; Metabolic acidosis; Respiratory alkalosis + Metabolic acidosis; Prolonged PT time ABGs
- 10. Significant salicylate toxicity: Serum levels > therapeutic range (10 - 20 mg/dL), particularly 6 hrs. post-ingestion (when absorption is usually almost complete), Acidemia plus ABG results compatible with salicylate poisoning. • Serum levels are helpful in confirming the diagnosis and may help guide therapy, but levels may be misleading and should be clinically correlated.
- 11. ABGs result (usually): Primary respiratory alkalosis (during the first few hours after ingestion); Later, they show compensated metabolic acidosis or mixed metabolic acidosis/respiratory alkalosis. As salicylate levels decrease, poorly compensated or uncompensated metabolic acidosis is the primary finding. If respiratory failure occurs, ABGs suggest combined metabolic and respiratory acidosis, and CXR shows diffuse pulmonary infiltrates. Plasma glucose levels may be normal, low, or high. Increased serum CK and urine myoglobin levels suggest rhabdomyolysis.
- 12. Management: Gastric lavage performed for upto 12 – 24 hrs. Activated charcoal: • Initial dose 1g/kg • Subsequent doses 25 g Q2H for 3 doses, or 50 g Q4H for 2 doses; For dehydration: 0.9% NS and Potassium as indicated; Correct electrolyte imbalance; Oxygen and glucose may be required. For severe acidosis, treat with bicarbonate (pH < 7.15);
- 13. Forced Alkaline Diuresis: Is indicated if/ in case of.. • Salicylate level > 50 mg/dl; • Very symptomatic patient; • Patient w/ increasing salicylate levels; Forced diuresis can be safely initiated if the urine flow rate is at least 4 ml/min. If not, give IV Frusemide 20 – 40 mg. Even after this, if urine flow rate is still < 4 ml/min., abandon the procedure as renal insufficiency is present.
- 14. Regime of IV infusion: • 500 ml D5% + 50 ml of 8.4% NaHCO3 • 500 ml D5% + 1 g KCl (if no hyperkalemia) • 500 ml NS + 40 mg frusemide • Given at a rate of 500 ml/hr.
- 15. The above cycle can be repeated for 2-3 times for 24- 48 hrs. Monitor the following: • Urine output (target > 4ml/min.); • I/O chart • Urine pH 7-8 • Potassium levels
- 16. Monitor for fluid overload in pulmonary and cerebral oedema cases (mostly among geriatric patients); Forced diuresis should be stopped in oliguric patients. Serum salicylate levels should be checked regularly until a consistent downward trend is observed in 2 successive readings.
- 17. FYI: Alkaline diuresis is indicated for patients with any symptoms of poisoning and should not be delayed until salicylate levels are determined. This intervention is usually safe and exponentially increases salicylate excretion. As hypokalemia may interfere with alkaline diuresis, patients are given a solution consisting of 1 L of 5% D/W, three 50-mEq ampules of NaHCO3, and 40 mEq of KCl at 1.5 to 2 times the maintenance IV fluid rate. Serum K is monitored. As fluid overload can result in pulmonary edema, patients are monitored for respiratory findings.
- 18. TDM Pointers - Paracetamol Poisoning
- 19. Paracetamol N-acetyl-p-benzoquinoneimine (toxic) Inactivated This interaction is concentration-dependent. Large overdose: • Glutathione is depleted. • N-acetyl-p-benzoquinoneimine binds to hepatic cell membranes, causing necrosis. Glutathione Conjugation Cyt.P-450
- 20. Clinical Features: 1st 24 hrs.: Vomiting; diaphoresis; pts. are usually fully conscious; After 24 hrs.: Hepatic enzymes’ conc. ↑es; peaks at 72-96 hrs.; Rt. Upper quadrant pain, coagulopathy, jaundice, somnolence, coma; Normally, recovery commences on 4th day post-ingestion, if hepatic failure does not occur.
- 21. Ix: • If patient presents within 1-4 hrs. post-ingestion, plasma paracetamol conc. should be estimated within 4 hrs. post- ingestion. • If it is ER product, one additional estimation should be done 4- 6 hrs. after the first estimation. • AST, ALT, Sr. bilirubin, BU, PT time, and Sr. Creatinine levels should be estimated daily for 3 days. • Suspected fulminant liver failure cases: Additionally estimate the Sr. glucose and ABG levels.
- 22. Management: For Pts. presenting within 1 hr.: • Gastric lavage; • Activated charcoal (one stat dose of 1 g/kg within 4 hrs. of ingestion); Acetylcysteine (IV or oral) – if paracetamol concs. are above toxic levels; Patients on enzyme-inducing drugs (CBZ, phenobarbitone, phenytoin, rifampicin, etc.) can develop toxicity at lower plasma paracetamol concs. They should be administered acetylcysteine if plasma paracetamol concs. are > 50% of the std. ref. values. For max. hepatoprotective effect, initiate Tx within 8-10 hrs. post-ingestion.
- 23. Tx should be stopped if the conc. falls below the treatment line. Acetylcysteine IV: Continuous Infusion in D5% 1) 150 mg/kg in 200 ml over 15 mins., followed by 2) 50 mg/kg in 500 ml over 4 hrs., then followed by 3) 100 mg/kg in 1000 ml over 16 hrs. Acetylcysteine oral: 140 mg/kg stat, followed by 70 mg/kg Q4H for 17 additional doses; Pts. w/ hepatic failure may require longer duration of admn. ( > 72 hrs.); Oral preparation may be more useful; End points are clinical improvement and INR < 2.0
- 24. Acetylcysteine should be used with caution in asthmatic patients as it can induce bronchospasm. Indications for acetylcysteine: Pt. ingested > 150 mg/kg paracetamol; Pt. has Hx of excessive ingestion of paracetamol. Sr. paracetamol cannot be done or is not available within 8 hrs. Pt. w/ unknown ingestion time, and Sr. paracetamol level > 10 mcg/ml; Lab evidence of hepatotoxicity (AST or ALT > 1000 IU/L);
- 25. Side effects: If flushing: Can continue acetylcysteine infusion; If urticaria: Stop the infusion; Treat w/ IV antihistamine; Restart infusion once symptoms resolve; Hypotension or respiratory symptoms: Switch from IV form to oral acetylcysteine;
- 26. Nomogram for paracetamol intoxication
- 27. THE END