
Recommended
Recommended
More Related Content
Similar to Understanding ARFID: Avoidant Restrictive Food Intake Disorder
Similar to Understanding ARFID: Avoidant Restrictive Food Intake Disorder (20)
More from pooleavelina
More from pooleavelina (20)
Recently uploaded
Recently uploaded (20)
Understanding ARFID: Avoidant Restrictive Food Intake Disorder
- 1. https://www.nationaleatingdisorders.org/learn/by-eating- disorder/arfid AVOIDANT RESTRICTIVE FOOD INTAKE DISORDER (ARFID) Avoidant Restrictive Food Intake Disorder (ARFID) is a new diagnosis in the DSM-5, and was previously referred to as “Selective Eating Disorder.” ARFID is similar to anorexia in that both disorders involve limitations in the amount and/or types of food consumed, but unlike anorexia, ARFID does not involve any distress about body shape or size, or fears of fatness. Although many children go through phases of picky or selective eating, a person with ARFID does not consume enough calories to grow and develop properly and, in adults, to maintain basic body function. In children, this results in stalled weight gain and vertical growth; in adults, this results in weight loss. ARFID can also result in problems at school or work, due to difficulties eating with others and extended times needed to eat. DIAGNOSTIC CRITERIA According to the DSM-5, ARFID is diagnosed when: · An eating or feeding disturbance (e.g., apparent lack of interest in eating or food; avoidance based on the sensory characteristics of food; concern about aversive consequences of eating) as manifested by persistent failure to meet appropriate nutritional and/or energy needs associated with one (or more) of the following: · Significant weight loss (or failure to achieve expected weight gain or faltering growth in children). · Significant nutritional deficiency. · Dependence on enteral feeding or oral nutritional supplements. · Marked interference with psychosocial functioning. · The disturbance is not better explained by lack of available food or by an associated culturally sanctioned practice. · The eating disturbance does not occur exclusively during the
- 2. course of anorexia nervosa or bulimia nervosa, and there is no evidence of a disturbance in the way in which one’s body weight or shape is experienced. · The eating disturbance is not attributable to a concurrent medical condition or not better explained by another mental disorder. When the eating disturbance occurs in the context of another condition or disorder, the severity of the eating disturbance exceeds that routinely associated with the condition or disorder and warrants additional clinical attention. RISK FACTORS As with all eating disorders, the risk factors for ARFID involve a range of biological, psychological, and sociocultural issues. These factors may interact differently in different people, which means two people with the same eating disorder can have very diverse perspectives, experiences, and symptoms. Researchers know much less about what puts someone at risk of developing ARFID, but here’s what they do know: · People with autism spectrum conditions are much more likely to develop ARFID, as are those with ADHD and intellectual disabilities. · Children who don’t outgrow normal picky eating, or in whom picky eating is severe, appear to be more likely to develop ARFID. · Many children with ARFID also have a co-occurring anxiety disorder, and they are also at high risk for other psychiatric disorders. WARNING SIGNS & SYMPTOMS OF ARFID Behavioral and psychological · Dramatic weight loss · Dresses in layers to hide weight loss or stay warm · Reports constipation, abdominal pain, cold intolerance, lethargy, and/or excess energy · Reports consistent, vague gastrointestinal issues (“upset stomach”, feels full, etc.) around mealtimes that have no known cause · Dramatic restriction in types or amount of food eaten
- 3. · Will only eat certain textures of food · Fears of choking or vomiting · Lack of appetite or interest in food · Limited range of preferred foods that becomes narrower over time (i.e., picky eating that progressively worsens). · No body image disturbance or fear of weight gain Physical Because both anorexia and ARFID involve an inability to meet nutritional needs, both disorders have similar physical signs and medical consequences. · Stomach cramps, other non-specific gastrointestinal complaints (constipation, acid reflux, etc.) · Menstrual irregularities—missing periods or only having a period while on hormonal contraceptives (this is not considered a “true” period) · Difficulties concentrating · Abnormal laboratory findings (anemia, low thyroid and hormone levels, low potassium, low blood cell counts, slow heart rate) · Postpuberty female loses menstrual period · Dizziness · Fainting/syncope · Feeling cold all the time · Sleep problems · Dry skin · Dry and brittle nails · Fine hair on body (lanugo) · Thinning of hair on head, dry and brittle hair · Muscle weakness · Cold, mottled hands and feet or swelling of feet · Poor wound healing · Impaired immune functioning HEALTH CONSEQUENCES OF ARFID In ARFID, the body is denied the essential nutrients it needs to function normally. Thus, the body is forced to slow down all of its processes to conserve energy, resulting in serious medical
- 4. consequences. The body is generally resilient at coping with the stress of eating disordered behaviors, and laboratory tests can generally appear perfect even as someone is at high risk of death. Electrolyte imbalances can kill without warning; so can cardiac arrest. Therefore, it’s incredibly important to understand the many ways that eating disorders affect the body. Cognitive-Behavioral Treatment of Avoidant/Restrictive Food Intake Disorder Jennifer J. Thomas, Ph.D.1,2, Olivia Wons, B.S.3, and Kamryn Eddy, Ph.D.1,2 1Eating Disorders Clinical and Research Program, Massachusetts General Hospital 2Department of Psychiatry, Harvard Medical School 3Neuroendocrine Unit, Massachusetts General Hospital Abstract Purpose of review: Avoidant/restrictive food intake disorder (ARFID) was added to the psychiatric nomenclature in 2013, but little is known about its optimal treatment. The purpose of this paper is to review the recent literature on ARFID treatment and highlight a novel cognitive- behavioral approach presently under study. Recent findings: The current evidence base for ARFID
- 5. treatment relies primarily on case reports, case series, and retrospective chart reviews, with only a handful of randomized controlled trials in young children. Studies in adults are lacking. ARFID treatments recently described in the literature include family-based treatment and parent training; cognitive-behavioral approaches; hospital-based re-feeding including tube feeding; and adjunctive pharmacotherapy. A novel form of outpatient cognitive-behavioral therapy for ARFID (CBT- AR) is one treatment currently under study. CBT-AR is appropriate for children, adolescents, and adults ages 10 and up; proceeds through four stages across 20–30 sessions; and is available in both individual and family- supported versions. Summary: There is no evidence-based psychological treatment suitable for all forms of ARFID at this time. Several groups are currently evaluating the efficacy of new psychological treatments for ARFID—particularly family-based and cognitive-behavioral approaches—but results have not yet been published. Keywords
- 6. Avoidant/restrictive food intake disorder; ARFID; family-based treatment; cognitive-behavioral therapy; tube feeding Correspondence to: Jennifer J. Thomas, Ph.D., Eating Disorders Clinical and Research Program, Massachusetts General Hospital, 2 Longfellow Place, Suite 200, Boston, MA 02114. [email protected] Phone: (617) 643-6306. Conflicts of interest. Drs. Thomas and Eddy will receive royalties from Cambridge University Press for the sale of their book Cognitive-Behavioral Therapy for Avoidant/Restrictive Food Intake Disorder: Children, Adolescents, and Adults, scheduled to be published in late 2018. HHS Public Access Author manuscript Curr Opin Psychiatry. Author manuscript; available in PMC 2019 November 01. Published in final edited form as: Curr Opin Psychiatry. 2018 November ; 31(6): 425–430. doi:10.1097/YCO.0000000000000454. A u th o r M a n
- 8. o r M a n u scrip t Introduction Avoidant/restrictive food intake disorder (ARFID) made its diagnostic debut in 2013 with the publication on DSM-5 [1]. ARFID is a reformulation and expansion of the former DSM- IV diagnosis of feeding disorder of infancy and early childhood, and can occur across the lifespan. The hallmark feature of ARIFD is food avoidance or restriction, motivated by sensitivity to the sensory characteristics of food, fear of aversive consequences of eating, or lack of interest in eating or food. To meet criteria for ARFID, the food restriction or avoidance must lead to one or more consequences such as weight loss or faltering growth, nutritional deficiency, dependence on oral nutritional supplements or tube feeding, or
- 9. psychosocial impairment. DSM-5 describes three example presentations of ARFID. In the first, individuals eat a very limited range of foods due to an inability to tolerate certain tastes and textures. In the second, individuals avoid specific foods or categories of food, or may stop eating altogether, for fear of aversive consequences of eating, such as choking, vomiting, anaphylaxis, or gastrointestinal distress. In the third, individuals exhibit a lack of interest in food or eating. It is important to note that these three presentations are not mutually exclusive and can co-occur within the same individual [2]. In addition to the heterogeneity of clinical presentation, ARFID is also quite diverse in terms of age, demographics, and comorbidities, highlighting the difficulty in identifying a universally applicable treatment approach. For example, ARFID has been reported in very young children [3 **], adolescents [4 *], and adults [5], and several studies have highlighted that both males and females present with the disorder [6,7]. Other investigations have
- 10. underscored numerous potential psychiatric and medical comorbidities, including autism spectrum disorder [8] and gastrointestinal disorders [6], which may further individualize treatment needs. Available data on the treatment of ARFID Because ARFID is so new, there is currently no evidence-based treatment suitable for all forms of the disorder. A robust literature that pre-dates DSM-5 supports the efficacy of behavioral interventions for young children with pediatric feeding disorders [9,10]. However, the generalizability of these approaches to individuals with ARFID—especially adolescents and adults—remains unclear. Below we summarize studies published since the 2013 advent of DSM-5 that describe the treatment of ARFID specifically. ARFID treatments recently described in the literature include family-based treatment and parent training; cognitive-behavioral approaches; hospital-based re-feeding including tube feeding; and adjunctive pharmacotherapy. Family-based treatment and parent training
- 11. Several recently published case reports have described the use of family-based treatment (FBT) for children and adolescents with ARFID [11,12,13]. Such approaches are similar to FBT for anorexia nervosa (AN) in that parents are charged with the task of feeding, but differ from FBT for AN in that parents are asked to support their children in increasing not only dietary volume, but also dietary variety through repeated exposure to novel foods. At least two clinical trials of FBT for ARFID are currently underway [14,15]. Another case Thomas et al. Page 2 Curr Opin Psychiatry. Author manuscript; available in PMC 2019 November 01. A u th o r M a n u scrip t
- 13. a n u scrip t report described the use of a behavioral parent-training intervention comprising differential reinforcement, gradual exposure to novel foods, and contingency management, resulting in the acceptance of 30 novel foods in a six-year-old with limited dietary variety [16]. Cognitive-behavioral approaches Multiple published case reports and case series have described the use of various forms of cognitive-behavioral therapy (CBT) for children [13,17,18] and adults [19,5] with ARFID. Common elements across CBT interventions for ARFID include regular eating [5,13], self- monitoring of food intake [5], exposure and response prevention [13,16], relaxation training [17,16, and behavioral experiments [5]. In one case study, a 16- year-old boy was able to significantly increase his consumption of proteins, fruits, and
- 14. vegetables, and significantly decrease his eating-related distress after 11 sessions of CBT supplemented with in-home meal interventions in which his mother reinforced the consumption of novel foods [16]. Hospital-based re-feeding including tube feeding Several hospital-based re-feeding programs have reported positive outcomes on eating and weight for children and adolescents with low-weight ARFID. One randomized controlled study prospectively evaluated the efficacy, among 20 boys and girls (ages 13–72 months) with ARFID, of a five-day manualized behavioral treatment comprising structured mealtimes, escape extinction, and reinforcement procedures in a day hospital setting. Patients randomized to the study treatment exhibited significantly greater bite acceptance, grams of food consumed at mealtime, and fewer mealtime disruptions post-treatment compared to those in the wait list control condition 3 **]. Another study described treatment response among 32 children and adolescents with ARFID treated in an eating disorders
- 15. partial hospitalization program, reporting significant increases in weight and significant decreases in eating pathology and anxiety from pre- to post- treatment after an average of seven weeks [4 *]. Treatment gains were maintained for at least 12 months in the subset of 20 patients who completed a follow-up assessment [20]. Several case studies have described the use of tube feeding to support inpatient nutritional rehabilitation among low-weight children and adolescents (ages 5–17 years old) with ARFID [21,22,23]. Of note, at least two studies have reported that patients with ARFID were significantly more likely than those with other eating disorders to require tube feeding during inpatient hospitalization [24,25 *]. Although tube feeding can be a life-saving measure in some cases of acute food refusal, a recent review described potentially iatrogenic effects of tube feeding, including long-term tube dependence and decreased oral intake [26], highlighting the urgent need for future research on effective tube weaning protocols for
- 16. individuals who require tube feeding. Adjunctive pharmacotherapy Three groups have recently published studies on pharmacotherapy as an adjunct to hospital- based treatment to facilitate meal consumption and/or weight gain in low-weight children and adolescents with ARFID. In one retrospective chart review, 14 children and adolescents demonstrated a significantly faster rate of weight gain after (versus before) being prescribed mirtazapine [27 *]. In another retrospective chart review, nine youth who took olanzapine Thomas et al. Page 3 Curr Opin Psychiatry. Author manuscript; available in PMC 2019 November 01. A u th o r M a n u scrip
- 18. a n u scrip t showed significant increases in weight from pre- to post- treatment [28 *]. The only double- blind randomized placebo-controlled trial of medication for ARFID evaluated the efficacy of D-cycloserine (DCS) augmentation of a five-day behavioral intervention for chronic and severe food refusal in 15 children (ages 20–58 months). Those randomized to the DCS condition showed a significantly greater percentage of bites rapidly swallowed, and significantly fewer mealtime disruptions, compared to those receiving placebo [29 **]. Summary of available data Available data on the treatment of ARFID are sparse, and limited to child and adolescent populations. Studies are limited to case reports, case series, and retrospective chart reviews,
- 19. with a handful of randomized controlled trials in very young children treated in day hospital settings. Findings in adults are limited to case reports, with no larger-scale studies on patients over the age of 18. Several groups are currently evaluating the efficacy of new psychological treatments for ARFID [14,15,30], but results have not yet been published. Case reports and case series have highlighted the promise of family-based treatment, cognitive-behavioral therapy, and hospital-based re-feeding, with pharmacotherapy as an adjunctive rather than a stand-alone treatment. Prospective randomized controlled trials are needed, particularly for adolescents and adults. The cognitive-behavioral formulation of ARFID To fill the need for manualized treatments suitable for testing in randomized controlled trials, our team at Massachusetts General Hospital has developed a novel form of cognitive- behavioral therapy for ARFID that is currently being tested in an open trial in which 20 participants ages 10–22 are receiving either individual of family-based versions of the
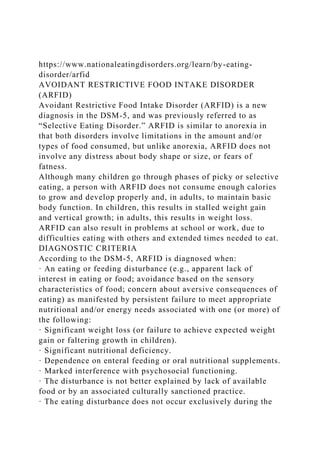
- 20. treatment [30,31 **]. The goal of CBT-AR is to help patients achieve a healthy weight, resolve nutrition deficiencies, increase variety to include multiple foods from each of the five basic food groups, eliminate dependence on nutritional supplements, and reduce psychosocial impairment. CBT-AR is based on our cognitive- behavioral conceptualization of the disorder (Figure 1), which posits that some individuals have a biological predisposition to sensory sensitivity, fear of aversive consequences, and/or lack of interest in food or eating [2]. Specifically, those with sensory sensitivity may have heightened response to unfamiliar tastes and smells, those with fear of aversive consequences may have high trait anxiety, and those with lack of interest in eating or food may have lower homeostatic or hedonic appetites. The CBT model posits that individuals with such predispositions will be vulnerable to developing negative feelings and predictions about eating. For example, the patient with
- 21. sensory sensitivity might feel disgust about novel foods and predict, “Every time I have tasted a vegetable, I have gagged, so I will probably hate any other vegetable.” These negative feelings and predictions would logically lead the patient to begin restricting food intake. Unfortunately, this food avoidance has both physiological and psychological consequences that reinforce negative feelings and predictions. Physiologically, the patient may experience nutritional compromise, such as weight loss or nutrition deficiencies. Under these auspices the patient may experience the predictable consequences of starvation such as Thomas et al. Page 4 Curr Opin Psychiatry. Author manuscript; available in PMC 2019 November 01. A u th o r M a n u
- 23. o r M a n u scrip t becoming satisfied on smaller portions of food, and experiencing altered taste perception from nutrition deficiencies, thus reinforcing the cycle of restricting volume. Psychologically, the more the patient relies on the same foods again and again, the greater the just noticeable difference will become between the patient’s preferred foods and novel foods, thus reinforcing the cycle of restricting variety. Cognitive-behavioral therapy for ARFID (CBT-AR) Based on our cognitive-behavioral model of ARFID, CBT-AR is designed reduce nutritional compromise and increase opportunities for exposure to novel foods to reduce negative feelings and predictions about eating. CBT-AR is appropriate for the outpatient treatment of
- 24. children, adolescents, and adults with ARFID (ages 10 and up). CBT-AR is a flexible, modular treatment designed to last approximately 20 (for patients who are not underweight) to 30 (for patients who have significant weight to gain) sessions over six to 12 months. CBT- AR is appropriate for individuals with ARFID who are medically stable, currently accepting at least some food by mouth, and not receiving tube feeding. Patients who are under the age of 16 and/or older adolescents and young adult patients who have significant weight to gain can be offered a family-supported version of CBT-AR, whereas patients ages 16 years and up without significant weight to gain can be treated with an individual version. CBT-AR proceeds through four broad stages (Table 1) [31 **]. In Stage 1, the therapist provides psychoeducation about ARFID and CBT-AR. In addition, the therapist encourages the patient to establish a pattern of regular eating and self- monitoring by relying primarily on preferred foods, but also encourages early change by asking the patient who is not
- 25. underweight to begin introducing minor variations in the presentation of preferred foods and/or reintroducing previously dropped foods. In contrast, the therapist encourages early change for patients who are underweight by asking them (often with family support) to increase their intake by at least 500 calories per day to support a weight gain of approximately 1–2 lbs per week. In Stage 2, the therapist provides psychoeducation about nutrition deficiencies and supports the patient in selecting novel fruits, vegetables, proteins, dairy, and grains to learn about in Stage 3 that will support resolution of these deficiencies, encourage further weight gain, and/or ameliorate psychosocial impairment. In Stage 3—the heart of the treatment—the therapist selects the module(s) most appropriate to the patient’s ARFID maintaining mechanisms(s) including sensory sensitivity, fear of aversive consequences, and/or lack of interest in food or eating. For patients with multiple maintaining mechanisms, the therapist starts with the module
- 26. addressing the primary or most impairing mechanism. Although Stage 3 interventions differ based on the specific module, the common element across all modules is exposure. For patients with sensory sensitivity, the therapist invites the patient (or family) to bring five novel foods to each session and asks the patient to non-judgmentally describe each food’s appearance, feel, smell, taste, and texture. The patient then selects foods to practice tasting throughout the week to facilitate habituation, and later works to incorporate larger portions of these novel foods into his or her day-to-day diet. For patients with fear of aversive consequences, the therapist works with Thomas et al. Page 5 Curr Opin Psychiatry. Author manuscript; available in PMC 2019 November 01. A u th o r M a
- 28. th o r M a n u scrip t the patient (or family) to create a fear and avoidance hierarchy of foods and eating-related situations that the patient fears will lead to negative outcomes. The therapist then conducts in-session exposures to these foods and situations, and asks the patient to repeat these exposures for homework, to test the patient’s predictions that the feared outcome will actually occur. Lastly, for patients with lack of interest in eating, the therapist introduces a series of interoceptive exposures (e.g., pushing one’s belly out, gulping water, and spinning in a chair) to help the patient habituate to sensations associated with eating and fullness. The therapist also helps the patient remember what he or she enjoys
- 29. about his or her preferred foods by describing their appearance, feel, smell, taste, and texture. Lastly, in Stage 4, the therapist supports the patient in evaluating progress, co-creating a relapse prevention plan, and setting goals for the future. Conclusion and future directions The addition of ARFID to DSM-5 has drawn attention to the urgent need for research into its optimal treatment. Available data are limited to case reports, case series, and randomized controlled trials in specialized populations of children and adolescents; treatment studies in adults are lacking. New psychological therapies are currently being tested. One such approach is a novel form of cognitive-behavioral therapy for children, adolescents, and adults that can be offered over 20–30 sessions in an individual or family-supported format. Given the heterogeneity of ARFID, it is likely that different presentations will require different interventions, and that once clinical trials have been completed, patients can be matched to the treatment that is the best fit for their unique
- 30. clinical needs. Acknowledgments Disclosure of funding. The authors would like to gratefully acknowledge funding for the work described in this paper from the National Institute of Mental Health (1R01MH108595), Hilda and Preston Davis Foundation, and American Psychological Foundation. References and Recommended Reading Papers of particular interest, published within the annual period of review, have been highlighted as: * of special interest ** of outstanding interest 1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-5). American Psychiatric Pub; 2013. 2. Thomas JJ, Lawson EA, Micali N et al. Avoidant/restrictive food intake disorder: a three- dimensional model of neurobiology with implications for etiology and treatment. Current psychiatry reports. 2017; 19:54. [PubMed: 28714048] 3 **. Sharp WG, Stubbs KH, Adams H et al. Intensive, manual- based intervention for pediatric feeding disorders: results from a randomized pilot trial. Journal of pediatric gastroenterology and nutrition. 2016; 62:658–63.
- 31. This randomized wait list controlled trial describes an intensive five-day manualized behavioral intervention for young children with ARFID. Thomas et al. Page 6 Curr Opin Psychiatry. Author manuscript; available in PMC 2019 November 01. A u th o r M a n u scrip t A u th o r M a n u scrip
- 32. t A u th o r M a n u scrip t A u th o r M a n u scrip t [PubMed: 26628445] 4 *. Ornstein RM, Essayli JH, Nicely TA et al. Treatment of avoidant/restrictive food intake disorder in
- 33. a cohort of young patients in a partial hospitalization program for eating disorders. International Journal of Eating Disorders. 2017; 50:1067–74. This retrospective chart review describes outcomes for children and adolescents with ARFID treated in a partial hospitalization program for eating disorders, which utilizes techniques from family- based treatment and cognitive-behavioral therapy. [PubMed: 28644568] 5. Steen E, Wade TD. Treatment of co‐occurring food avoidance and alcohol use disorder in an adult: possible avoidant restrictive food intake disorder?. International Journal of Eating Disorders. 2018; 51:373–377. [PubMed: 29394459] 6. Eddy KT, Thomas JJ, Hastings E et al. Prevalence of DSM‐5 avoidant/restrictive food intake disorder in a pediatric gastroenterology healthcare network. International Journal of Eating Disorders. 2015; 48:464–70. [PubMed: 25142784] 7. Forman SF, McKenzie N, Hehn R et al. Predictors of outcome at 1 year in adolescents with DSM-5 restrictive eating disorders: report of the national eating disorders quality improvement collaborative. Journal of Adolescent Health. 2014; 55:750–6. [PubMed: 25200345] 8. Lucarelli J, Pappas D, Welchons L, Augustyn M. Autism spectrum disorder and avoidant/restrictive food intake disorder. Journal of Developmental & Behavioral
- 34. Pediatrics. 2017; 38:79–80. [PubMed: 27824638] 9. Lukens CT, Silverman AH. Systematic review of psychological interventions for pediatric feeding problems. Journal of pediatric psychology. 2014 6 13;39(8):903–17. [PubMed: 24934248] 10. Sharp WG, Volkert VM, Scahill L et al. A systematic review and meta-analysis of intensive multidisciplinary intervention for pediatric feeding disorders: how standard is the standard of care?. The Journal of pediatrics. 2017; 181:116–24. [PubMed: 27843007] 11. Fitzpatrick KK, Forsberg SE, Colborn. Family-based therapy for avoidant restrictive food intake disorder: Families Facing Food Neophobias In: Family Therapy for Adolescent Eating and Weight Disorders. 1 Loeb K. (Ed.), Le Grange D. (Ed.), Lock J. (Ed.). New York: Routledge; 2015 pp. 276–296 12. Norris ML, Spettigue WJ, Katzman DK. Update on eating disorders: current perspectives on avoidant/restrictive food intake disorder in children and youth. Neuropsychiatric disease and treatment. 2016; 12:213–218. [PubMed: 26855577] 13. Thomas JJ, Brigham KS, Sally ST et al. Case 18–2017—an 11-year-old girl with difficulty eating after a choking incident. New England journal of medicine. 2017; 376:2377–86. [PubMed: 28614676] 14. Lesser J, Eckhardt S, Ehrenreich-May J, et al. Integrating
- 35. family based treatment with the unified protocol for the transdiagnostic treatment of emotional 351 disorders: a novel treatment for avoidant restrictive food intake disorder. Clinical Teaching Day presentation at the International Conference on Eating Disorders; 2017; Prague, Czech Republic. 15. Sadeh-Sharvit S, Robinson A, Lock J. FBT-ARFID for younger patients: lessons from a randomized controlled trial. Workshop presented at the International Conference on Eating Disorders; 2018; Chicago, Illinois. 16. Murphy J, Zlomke KR. A behavioral parent-training intervention for a child with avoidant/ restrictive food intake disorder. Clinical Practice in Pediatric Psychology. 2016; 4:23–34. 17. Fischer AJ, Luiselli JK, Dove MB. Effects of clinic and in- home treatment on consumption and feeding-associated anxiety in an adolescent with avoidant/restrictive food intake disorder. Clinical Practice in Pediatric Psychology. 2015; 3:154–166. 18. Bryant Waugh R Avoidant restrictive food intake disorder: an illustrative case example. International Journal of Eating Disorders. 2013; 46:420–3. [PubMed: 23658083] 19. King LA, Urbach JR, Stewart KE. Illness anxiety and avoidant/restrictive food intake disorder: cognitive-behavioral conceptualization and treatment. Eating behaviors. 2015; 19:106–9. [PubMed: 26276708] Thomas et al. Page 7
- 36. Curr Opin Psychiatry. Author manuscript; available in PMC 2019 November 01. A u th o r M a n u scrip t A u th o r M a n u scrip t A u th
- 37. o r M a n u scrip t A u th o r M a n u scrip t 20. Bryson AE, Scipioni AM, Essayli JH et al. Outcomes of low‐weight patients with avoidant/ restrictive food intake disorder and anorexia nervosa at long‐term follow‐up after treatment in a partial hospitalization program for eating disorders. International Journal of Eating Disorders. 2018; 51:470–474. [PubMed: 29493804] 21. Guvenek-Cokol PE, Gallagher K, Samsel C. Medical traumatic stress: a multidisciplinary approach
- 38. for iatrogenic acute food refusal in the inpatient setting. Hospital pediatrics. 2016; 6:693–8. [PubMed: 27803075] 22. Pitt PD, Middleman AB. A focus on behavior management of avoidant/restrictive food intake disorder (ARFID): a case series. Clinical pediatrics. 2018; 57:478–80. [PubMed: 28719985] 23. Schermbrucker J, Kimber M, Johnson N et al. Avoidant/restrictive food intake disorder in an 11- year old south American boy: medical and cultural challenges. Journal of the Canadian Academy of Child and Adolescent Psychiatry. 2017; 26:110–113. [PubMed: 28747934] 24. Strandjord SE, Sieke EH, Richmond M, Rome ES. Avoidant/restrictive food intake disorder: illness and hospital course in patients hospitalized for nutritional insufficiency. Journal of Adolescent Health. 2015; 57:673–8. [PubMed: 26422290] 25 *. Peebles R, Lesser A, Park CC et al. Outcomes of an inpatient medical nutritional rehabilitation protocol in children and adolescents with eating disorders. Journal of eating disorders. 2017; 5:1– 14. This paper describes the Children’s Hospital of Philadelphia (CHOP) Malnutrition Protocol for the inpatient re-feeding of children and adolescents with restrictive eating disorders, including ARFID.
- 39. [PubMed: 28053702] 26. Dovey TM, Wilken M, Martin CI, Meyer C. Definitions and clinical guidance on the enteral dependence component of the avoidant/restrictive food intake disorder diagnostic criteria in children. Journal of Parenteral and Enteral Nutrition. 2018; 42:499–507. 27 *. Gray E, Chen T, Menzel J et al. Mirtazapine and weight gain in avoidant and restrictive food intake disorder. Journal of the American Academy of Child & Adolescent Psychiatry. 2018; 57:288–9. This retrospective chart review describes adjuctive pharmacotherapy with mirtazipine for children and adolescents with ARFID. [PubMed: 29588055] 28 *. Brewerton TD, D’Agostino M. Adjunctive use of olanzapine in the treatment of avoidant restrictive food intake disorder in children and adolescents in an eating disorders program. Journal of child and adolescent psychopharmacology. 2017; 27:920–2. This retrospective chart review describes adjunctive pharmacotherapy with olanazapine for children and adolescents with ARFID. [PubMed: 29068721]
- 40. 29 **. Sharp WG, Allen AG, Stubbs KH et al. Successful pharmacotherapy for the treatment of severe feeding aversion with mechanistic insights from cross-species neuronal remodeling. Translational psychiatry. 2017; 7:1–9. This double blind randomized placebo controlled trial describes adjunctive pharmacotherapy with D- cycloserine for young children with chronic and severe food refusal. 30. Thomas JJ, Becker KR, Wons O et al. Cognitive behavioral therapy for avoidant/restrictive food intake disorder (CBT-AR): A pilot study demonstrating feasibility, efficacy, and acceptability. Submitted to the XXIVth Annual Meeting of the Eating Disorders Research Society 2018. 31 **. Thomas JJ, Eddy KT. Cognitive-behavioral therapy for avoidant/restrictive food intake disorder: children, adolescents, and adults. Cambridge, UK: Cambridge University Press; in press. This book describes a novel cognitive-behavioral model of the maintenance of ARFID and is the first treatment manual to describe the implementation of cognitive- behavioral therapy for the disorder. Thomas et al. Page 8 Curr Opin Psychiatry. Author manuscript; available in PMC 2019 November 01. A
- 42. u scrip t A u th o r M a n u scrip t Key points • There are no evidence-based psychological treatments suitable for all forms of avoidant/restrictive food intake disorder at this time. • The current evidence base for ARFID treatment relies primarily on case reports, case series, retrospective chart reviews, and a handful of randomized controlled trials in very young children. Treatment studies in adults are lacking.
- 43. • ARFID interventions recently described in the literature include family-based treatment and parent training; cognitive-behavioral approaches; hospital- based re-feeding including tube feeding; and adjunctive pharmacotherapy. • New psychological treatments are currently being tested, including a novel form of cognitive-behavioral therapy for children, adolescents, and adults that can be offered over 20–30 sessions in an individual or family- supported format. Thomas et al. Page 9 Curr Opin Psychiatry. Author manuscript; available in PMC 2019 November 01. A u th o r M a n u scrip
- 45. a n u scrip t Figure 1. Cognitive-behavioral model of avoidant/restrictive food intake disorder Thomas et al. Page 10 Curr Opin Psychiatry. Author manuscript; available in PMC 2019 November 01. A u th o r M a n u scrip t A u th
- 46. o r M a n u scrip t A u th o r M a n u scrip t A u th o r M a n u scrip
- 48. o r M a n u scrip t A u th o r M a n u scrip t Thomas et al. Page 11 Table 1. Four stages of cognitive-behavioral therapy for avoidant/restrictive food intake disorder (CBT-AR) Stage Primary interventions 1. Psychoeducation and early change
- 49. (2–4 sessions) • Psychoeducation on ARFID and its treatment • Self- or parent-monitoring of food intake • Establishing a pattern of regular eating to normalize hunger cues • Increasing volume of preferred foods (for patients who are underweight) and variety (for all patients) • Individualized formulation of mechanisms that maintain avoidant/restrictive eating (i.e., sensory sensitivity, fear of aversive consequences, lack of interest in eating or food) 2. Treatment planning (2 sessions) • Continue increasing volume and/or variety • Reviewing intake from Primary Food Group Building Blocks and selecting foods to learn about in Stage 3 3. Maintaining mechanisms in order of priority (14–22 sessions) • Sensory sensitivity: Systematic desensitization to novel foods by repeated in-session exploration of sight, smell, texture, taste, chew; specific, detailed plans for out-of- session practice with tasting and incorporation • Fear of aversive consequences: Psychoeducation about how avoidance maintains anxiety, development of fear/avoidance hierarchy, graded exposure to feared foods and situations in which choking, vomiting, or other feared consequence may occur • Apparent lack of interest in eating or food: Interoceptive exposure to bloating, fullness, and/or nausea; in- session exposure to highly-preferred foods
- 50. 4. Relapse prevention(2 sessions) • Evaluating whether treatment goals have been met, identifying treatment strategies to continue at home, and developing a plan for maintaining weight gain (if needed) continuing to learn about novel foods Curr Opin Psychiatry. Author manuscript; available in PMC 2019 November 01. AbstractIntroductionAvailable data on the treatment of ARFIDFamily-based treatment and parent trainingCognitive- behavioral approachesHospital-based re-feeding including tube feedingAdjunctive pharmacotherapySummary of available dataThe cognitive-behavioral formulation of ARFIDCognitive- behavioral therapy for ARFID (CBT-AR)Conclusion and future directionsReferencesFigure 1.Table 1. Eating Disorder Core Symptoms and Symptom Pathways Across Developmental Stages: A Network Analysis Caroline Christian University of Louisville Victoria L. Perko University of Kansas Irina A. Vanzhula University of Louisville Jenna P. Tregarthen Recovery Record, Inc., San Francisco, California Kelsie T. Forbush
- 51. University of Kansas Cheri A. Levinson University of Louisville Eating disorders (EDs) often develop during adolescence and early adulthood but may persist, arise, or reemerge across the life span. Research and treatment efforts primarily focus on adolescent and young adult populations, leaving large knowledge gaps regarding ED symptoms across the entire developmental spectrum. The current study uses network analysis to compare central symptoms (i.e., symptoms that are highly connected to other symptoms) and symptom pathways (i.e., relations among symptoms) across five developmental stages (early adolescence, late adolescence, young adulthood, early-middle adult- hood, middle-late adulthood) in a large sample of individuals with EDs (N � 29,902; N � 32,219) in two network models. Several symptoms related to overeating, food avoidance, feeling full, and overvaluation of weight and shape emerged as central in most or all developmental stages, suggesting that some core symptoms remain central across development. Despite similarities in central symptoms, significant differences in network structure (i.e., how symptom pathways are connected) emerged across age groups. These differences suggest that symptom interconnectivity (but not symptom severity) might increase across development. Future research should continue to investigate developmental symptom differences in order to inform treatment for individuals with EDs of all ages. General Scientific Summary Connections between eating disorder symptoms vary across
- 52. stages of development. Consistent with Habit Formation Theory, symptoms were more tightly connected in older individuals, who have on average a longer duration of illness. In contrast, eating disorder central symptoms (symptoms related to overeating, food avoidance, fullness, and overvaluation of weight and shape) were relatively consistent across age groups. Keywords: eating disorder symptoms, development, age, network analysis, eating disorders Supplemental materials: http://dx.doi.org/10.1037/abn0000477.supp This article was published Online First November 11, 2019. X Caroline Christian, Department of Psychological and Brain Sciences, University of Louisville; Victoria L. Perko, Department of Psychology, University of Kansas; Irina A. Vanzhula, Department of Psychological and Brain Sciences, University of Louisville; Jenna P. Tregarthen, Recovery Record, Inc., San Francisco, California; Kelsie T. Forbush, Department of Psychology, University of Kansas; Cheri A. Levinson, Department of Psychological and Brain Sciences, University of Louisville. The present study is a new analysis of previously analyzed data. This study is the investigation of developmental differences in eating disorder symptoms using network analysis using this dataset. No other
- 53. papers have addressed similar questions as those addressed in this article. All study procedures were approved by the University of Kansas Institutional Re- view Board (Study IRB STUDY00003260). Authors complied with APA ethical standards in the treatment of their participants. The manuscript has not been and is not posted on a website. Jenna P. Tregarthen is a co-founder and shareholder of Recovery Record, Inc. Jenna P. Tregarthen made a substantial contribution as part of data collection and curation and ap- proved the final manuscript, but she did not participate in the analysis, interpretation, or drafting of the manuscript. Kelsie T. Forbush received an industry-sponsored grant from Recovery Record, Inc. No other authors have conflicts of interest to disclose. Correspondence concerning this article should be addressed to Cheri A. Levinson, Department of Psychological and Brain Sciences, University of Louisville, Life Sciences Building 317, Louisville, KY 40292. E-mail: [email protected] T hi s do
- 58. oa dl y. Journal of Abnormal Psychology © 2019 American Psychological Association 2020, Vol. 129, No. 2, 177–190 ISSN: 0021-843X http://dx.doi.org/10.1037/abn0000477 177 https://orcid.org/0000-0001-7741-1498 mailto:[email protected] http://dx.doi.org/10.1037/abn0000477 Eating disorders (EDs) are serious mental illnesses associated with negative health consequences, significant impairment, and high mortality (Crow et al., 2009; Rome & Ammerman, 2003; Stice, Marti, & Rohde, 2013). Peak age of ED onset is during adolescence, between 16 and 20 years of age (Stice et al., 2013). Although EDs most commonly develop during this period, evi- dence suggests that eating pathology may persist, return, or de- velop throughout an individual’s life (Fulton, 2016; Patrick & Stahl, 2009). Indeed, studies indicate that ED symptoms occur across all developmental stages, with approximately 11% of adults aged 42–55 and 4% of adults aged 60 –70 engaging in ED behav- iors, such as binge eating, laxative/diuretic misuse, or self- induced vomiting (Mangweth-Matzek et al., 2006; Marcus, Bromberger, Wei, Brown, & Kravitz, 2007). The presence of disordered
- 59. eating among middle and older adults suggests that it is important to examine EDs across the full developmental spectrum; however, to date, research has primarily focused on EDs in adolescence and early adulthood. Past research suggests that ED symptoms may change across development. However, the nature of these differences remains unclear. In terms of diagnoses, older individuals are more likely to be diagnosed with binge eating disorder, as compared to younger individuals with EDs (Jenkins & Price, 2018). Additionally, diag- nostic migration is extremely common in EDs, which suggests that symptomatology may shift as the person and illness develop (Cas- tellini et al., 2011; Fichter & Quadflieg, 2007). In terms of sever- ity, some research suggests that disordered eating behaviors, body dissatisfaction, and distorted cognitions surrounding food decline with age (Gadalla, 2008; Forman & Davis, 2005; Tiggemann & McCourt, 2013). Reduction of ED cognitions may be related to the changing social environment over the life span. In one study, the association between negative commentary about one’s weight and shape and bulimic symptoms diminished with older age (Tzoneva, Forney, & Keel, 2015).
- 60. However, other studies indicated body dissatisfaction and diet- ing behaviors remain prevalent and may strengthen with age (e.g., Fulton, 2016). Indeed, research supports that overvaluation of weight and shape is pervasive among middle age and older adults (Forman & Davis, 2005; Patrick & Stahl, 2009; Mangweth- Matzek et al., 2006). The Habit Formation Theory of EDs suggests that maladaptive eating behaviors may begin as goal-driven (e.g., di- eting to lose weight), but with repetition, these behaviors (e.g., restriction), coupled with the reward (e.g., praise from others on losing weight), develop into a deeply engrained habit (Walsh, 2013). Similarly, binge eating and purging behaviors may begin impulsively to cope with negative emotions but can develop into compulsive rituals with repetition (Pearson, Wonderlich, & Smith, 2015). Thus, Habit Formation Theory posits that maladaptive eating behaviors and cognitions will become more deeply en- grained and habitual in later developmental stages. Indeed, studies indicate that older age of onset and longer duration-of-illness are associated with poor treatment outcomes (Noordenbos, Olden- have, Muschter, & Terpstra, 2002; Norring & Sohlberg, 1993), highlighting the clinical importance of researching eating pathol- ogy across development. Overall, the current state of eating disorder research provides an incomplete picture of cognitions and behaviors across the life span. Thus, additional research examining the differences in eating dis- order symptoms across developmental stages is urgently needed.
- 61. Specifically, it is unknown how specific symptoms and symptom relationships might change across developmental periods to main- tain ED psychopathology. One novel way to conceptualize EDs is network theory. Net- work analysis (NA) is a statistical methodology based on network theory, which conceptualizes psychopathology as a web of inter- connecting nodes (symptoms) and edges (associations between symptoms) that are theorized to maintain a specific illness state (Borsboom, 2017). NA allows researchers to identify specific relationships among many symptoms at once and provides oppor- tunities to visualize illness pathways (relationships among individ- ual symptoms) and identify central symptoms (symptoms that are highly connected with other symptoms in the network). NA can also identify if two networks are significantly different from each other in structure (i.e., if two symptoms are similarly associated in both networks) and global strength (how strongly symptoms are associated with each other; van Borkulo et al., 2015). This tech- nique allows researchers to investigate if (and how) two popula- tions or subgroups of a population differ in symptom connected- ness. Several studies have used NA to understand ED psychopathol- ogy. These studies found body checking (Forbush, Siew, & Vite- vitch, 2016), fear of weight gain (Elliott, Jones, & Schmidt, 2018;
- 62. Forrest, Jones, Ortiz, & Smith, 2018; Levinson et al., 2017), and other symptoms related to overvaluation of weight and shape (DuBois, Rodgers, Franko, Eddy, & Thomas, 2017; Elliott et al., 2018; Forrest et al., 2018; Goldschmidt et al., 2018; Wang, Jones, Dreier, Elliott, & Grilo, 2018) to be central, maintaining symp- toms, consistent with the cognitive– behavioral theory of EDs (Cooper & Shafran, 2008; Fairburn, 2008). A few additional studies have identified additional important symptoms, such as dietary restraint (Goldschmidt et al., 2018; Solmi et al., 2018), interoceptive awareness, (Olatunji, Levinson, & Calebs, 2018; Solmi et al., 2018), and ineffectiveness (Olatunji et al., 2018; Solmi et al., 2018; Solmi, Collantoni, Meneguzzo, Tenconi, & Favaro, 2019), and the relationships among depression, anxiety, and ED symptoms (Solmi et al., 2018, 2019). Although NA has been applied to increase the broad understand- ing of eating pathology, no research has examined differences in network models of ED symptoms across developmental stages. Past research suggests that there may be unique differences in ED presentations across the life span, including diagnostic differences, physical changes, and differences in treatment outcomes (Cas- tellini et al., 2011; Forman & Davis, 2005; Hudson & Pope, 2018; Jenkins & Price, 2018; Peat, Peyerl, & Muehlenkamp, 2008). Thus, it seems likely that ED symptom relationships may also differ across developmental stages. Better understanding of the differences in central ED symptoms across developmental stages could help determine if alternative treatments would be more beneficial for different age groups.
- 63. The current study utilizes NA to examine ED symptoms in five distinct developmental stages: early adolescence (11–14), late ad- olescence (15–18), young adulthood (19 –25), early-middle adult- hood (26 – 45), and middle-late adulthood (46�). These age ranges represent unique developmental stages in several aspects, includ- ing social environment, physiological and neurological develop- ment, maturity, and autonomy (Blonigen, Carlson, Hicks, Krueger, & Iacono, 2008; Steinberg, 2005; Williams & Currie, 2000). We examine symptom relationships across two widely used ED mea- T hi s do cu m en t is co py ri gh te
- 67. an d is no t to be di ss em in at ed br oa dl y. 178 CHRISTIAN ET AL. sures: the Eating Pathology Symptoms Inventory (EPSI; Forbush et al., 2013) and Eating Disorder Examination Questionnaire (EDE-Q; Fairburn & Beglin, 1994). Both questionnaires are con-
- 68. sidered “gold-standard” measures of ED symptoms and are fre- quently used for network investigations (DuBois et al., 2017; Forbush et al., 2016; Forrest et al., 2018), yet they assess slightly different aspects of ED symptoms, such that the EDE-Q is based on the cognitive– behavioral model of EDs and the EPSI is de- signed to be a multidimensional assessment of ED symptoms. Thus, we include both measures to allow for a more comprehen- sive overview of ED symptoms and to gain insight into the replicability of networks. We hypothesized that symptoms that were central in past studies using NA (e.g., overvaluation of weight and shape; Levinson, Vanzhula, Brosof, & Forbush, 2018) would remain central regard- less of age, as suggested by the literature (Forman & Davis, 2005; Patrick & Stahl, 2009; Mangweth-Matzek et al., 2006). Further, we hypothesized that there would be a significant difference in net- work structure across networks. Despite some common threads across EDs, specific connections between symptoms are likely to differ across developmental stages, given what the literature has described in terms of differences in symptom severity and treat- ment effectiveness (Hudson & Pope, 2018; Jenkins & Price, 2018; Peat et al., 2008; Forman & Davis, 2005). For example, although fear of weight gain may remain central across diverse ED presen- tations, the connection between fear of weight gain and binge eating may become stronger over time, consistent with the Habit Formation Theory (Walsh, 2013). This change would result in differences in network structure, which has implications for im- plementing effective treatments across age groups.
- 69. Additionally, we predict that the global strength would increase for networks with older participants compared to younger participants, reflec- tive of Habit Formation Theory, indicating increased severity across developmental stages. Method Participants Participants were Recovery Record users (N � 29,902; N � 32,219), a smartphone application that is based on cognitive– behavioral treatment for EDs (Tregarthen, Lock, & Darcy, 2015). Participants provided consent for data to be used for research purposes when they agreed to the “Terms and Conditions” in the initial application setup. Participants who completed the EPSI (n � 29,902) were 11 to 85 years old (M � 26.23, SD � 10.46), and 94.0% identified as female. These participants reported their av- erage length of ED was 9.71 years (SD � 9.72, range � 0 – 65 years). Recovery Record allows users to connect their account with a clinician in order to share information and inform treatment planning. In our sample, 34.5% of participants had accounts con- nected with a treatment provider and had an official diagnosis of an ED based on clinician-report. Participants who completed the EDE-Q (n � 32,219) were 11 to 79 years old (M � 23.43, SD � 8.89), and 96.5% identified as female. Average length of ED was 7.60 years (SD � 8.23, range �
- 70. 0 – 60 years). In the present sample, 8.8% of participants had accounts connected with a treatment provider and had an official diagnosis of an ED based on clinician-report. See Table 1 for Table 1 Demographic Breakdown Demographic characteristic Early adolescence n (%) Late adolescence n (%) Young adult n (%) Early-middle adult n (%) Middle-late adult n (%) EDE-Q 1523 (100) 9838 (100) 11709 (100) 7955 (100) 1194 (100) Gender Female 1468 (96.4) 9498 (96.5) 11310 (96.6) 7671 (96.4) 1131 (94.7) Male 42 (2.8) 248 (2.5) 288 (2.9) 228 (2.9) 56 (4.7) Missing 13 (.9) 92 (.9) 111 (.7) 56 (.7) 7 (.6) Diagnosis
- 71. AN 13 (.9) 85 (.9) 159 (1.4) 133 (1.7) 19 (1.6) BN 2 (.1) 37 (.4) 99 (.8) 104 (1.3) 12 (1.0) BED 4 (.3) 12 (.1) 49 (.4) 104 (1.3) 55 (4.6) Other 3 (.2) 42 (.4) 93 (.8) 102 (1.3) 18 (1.5) Missing 1501 (98.6) 9662 (98.2) 11309 (96.6) 7522 (94.6) 1090 (91.3) Duration of illness (M[SD]) 1.71 (1.71) 2.92 (2.27) 5.82 (3.96) 13.86 (8.37) 29.00 (14.60) EPSI 1028 (100) 6171 (100) 10701 (100) 9929 (100) 2073 (100) Gender Female 959 (93.3) 5786 (93.8) 10108 (94.5) 9412 (94.8) 1857 (89.6) Male 46 (4.5) 228 (3.7) 381 (3.6) 438 (4.4) 201 (9.7) Missing 23 (2.2) 157 (2.5) 212 (2.0) 79 (.8) 15 (.7) Diagnosis AN 152 (14.8) 796 (12.9) 1456 (13.6) 995 (10.0) 172 (8.3) BN 30 (2.9) 307 (5.0) 870 (8.1) 825 (8.3) 81 (3.9) BED 31 (3.0) 165 (2.7) 514 (4.8) 1144 (11.5) 527 (25.4) Other 62 (6.0) 354 (5.7) 795 (7.4) 830 (8.4) 222 (10.7) Missing 753 (73.2) 4549 (73.7) 7066 (66.0) 6134 (61.8) 1071 (51.7) Duration of illness (M[SD]) 2.06 (2.11) 3.19 (2.44) 6.05 (4.12) 14.54 (8.58) 29.12 (15.20) Note. EDE-Q � Eating Disorder Examination Questionnaire; EPSI � Eating Pathology Symptoms Inventory; AN � anorexia nervosa; BN � bulimia nervosa; BED � binge eating disorder. T hi
- 76. ed br oa dl y. 179EATING DISORDER AGE NETWORKS participants’ gender, ED diagnoses, and duration of illness across developmental categories. Measures EPSI. The EPSI is a 45-item multidimensional measure de- signed to assess ED symptoms. The EPSI has eight scales corre- sponding to unique facets of eating pathology: Body Dissatisfac- tion (i.e., satisfaction with body shape and body parts; e.g., hips, thighs), Binge Eating (i.e., tendency to overeat or eat mindlessly), Cognitive Restraint (i.e., attempting to restrict eating, whether successful or not), Excessive Exercise (i.e., intense or compulsive exercise), Restricting (i.e., efforts to avoid or reduce eating), Purging (i.e., self-induced vomiting and laxative/diuretic use), Muscle Building (i.e., cognitions and behaviors [supplement use] related to increasing muscularity), and Negative Attitudes Toward Obesity (i.e., negative judgment of individuals who are over-
- 77. weight/obese). Between 32.6% and 73.6% of our sample scored above EPSI subscale means in an ED treatment sample (Forbush et al., 2013). Two scales of the EPSI, Negative Attitudes Toward Obesity and Muscle Building, were not included in the Recovery Record app; thus, these items were not included in the network. The EPSI has excellent convergent and discriminant validity, as well as excellent test-retest reliability (Forbush et al., 2013). The internal consistency of all items included in the EPSI network was adequate for the current sample (� � .73). EDE-Q. The EDE-Q version 6.0 is a 28-item self-report ques- tionnaire designed to assess ED behaviors and thoughts. This version of the EDE-Q has four scales: Eating Concern (i.e., inter- fering thoughts about food, eating, or calories), Shape Concern (i.e., interfering thoughts about shape), Weight Concern (i.e., in- terfering thoughts about weight), and Restraint (i.e., attempts to reduce food intake; e.g., skipping meals, food rules). The mean EDEQ global score in our sample is 4.17 (SD � 1.10), and 63.3% (n � 20,390) of our sample scored above the recommended clinical cutoff (a score of 4.0 or higher) for EDs (Fairburn, Wilson, & Schleimer, 1993). One EDE-Q item (15) was excluded because it measures the same symptom (binge eating) as the previous question. Networks should not include two questions targeting the same symptom because it may artificially inflate centrality, poten- tially leading to false interpretation of that symptom as central
- 78. (Fried & Cramer, 2017). The EDE-Q has demonstrated excellent test-retest reliability and internal consistency (Luce & Crowther, 1999) and good criterion and concurrent validity (Mond, Hay, Rodgers, Owen, & Beumont, 2004). The internal consistency of all items included in the EDE-Q network was good for the current sample (� � .86). Procedure Participants used the Recovery Record application to self- monitor ED cognitions and behaviors. The application encourages monthly completion of the EDE-Q and the EPSI. The present study used data from the initial completion of EDE-Q and EPSI by participants using the mobile application. Participant data were categorized into five developmental stag- es: early adolescence (11–14), late adolescence (15–18), young adulthood (19 –25), early-middle adulthood (26 – 45), and middle- late adulthood (46�). Our ranges may not fully distinguish be- tween all stages of development because we had few participants above the age of 45 (n � 1,194 for EPSI, n � 2,073 for EDE-Q) relative to the entire sample, so we used 45 as a cutoff for middle-late adulthood in order to ensure a large sample size for the networks. Using younger age ranges is not uncommon for clinical studies on EDs due to difficulty recruiting older adults with EDs (Forman & Davis, 2005; Jenkins & Price, 2018).
- 79. Glasso networks using the EDE-Q and EPSI were estimated at each developmental stage using the “estimateNetwork” function in the bootnet package in R (Epskamp, Maris, Waldorp, & Bors- boom, 2018). The Glasso function estimates partial correlations between nodes, meaning each correlation is unique, accounting for all other symptoms in the network while minimizing spurious relationships. We first created networks using the default setting (cor_auto), which uses polychoric correlations. However, because some networks did not have adequate stability, we estimated the networks again using Spearman correlations to obtain stable net- works, as suggested by Epskamp and Fried (2018). Stability esti- mates were calculated using the bootnet package in R (Epskamp et al., 2018). Three indices of centrality were calculated using the “centrali- typlot” function in the qgraph package in R: strength (i.e., the sum of the absolute value of all of a node’s edges), closeness (i.e., degree of direct connections to other nodes), and betweenness (i.e., degree to which a node falls on the path between other nodes; Epskamp, Cramer, Waldorp, Schmittmann, & Borsboom, 2012). We interpret only strength centrality because it was the most stable, as has been done in prior NA investigations (e.g., DuBois et al., 2017; Epskamp et al., 2012). Centrality difference tests were conducted using the bootnet package in R (Epskamp et al.,
- 80. 2018) to determine if central symptoms were significantly more central than other symptoms. We included three to six central symptoms for each network based on the network centrality difference test. The number of symptoms included per network is based on sharp observable decreases in centrality differences among top symp- toms that were used as cutoffs for inclusion. We did not use a standard cutoff value across networks due to internetwork vari- ability. Differences between networks across developmental stages were identified using the NetworkComparisonTest package in R (van Borkulo et al., 2015). Three metrics were utilized to analyze network differences: network invariance test (M; i.e., significant differences in the maximum edge strength in the networks), edge invariance test (E; i.e., significant differences between specific edges in the networks), and global strength invariance test (GSI; i.e., significant differences in the sum of the edge strengths; van Borkulo et al., 2015). Edge invariance was calculated for networks with significant network invariance in order to quantify the nature of these structural differences. Global strength is a particularly useful measure, as it may be related to symptom severity (van Borkulo et al., 2015). A one-way ANOVA was conducted across developmental stages for both the EDE-Q and EPSI to investigate whether sig- nificant differences in symptom severity across groups were re-
- 81. lated to global strength across networks, as has been theorized (van Borkulo et al., 2015). We conducted these analyses using the EDE-Q global score, as factor validity is strongest for the global index rather than the four subscales (Aardoom, Dingemans, Sloft Op’t Landt, & Van Furth, 2012) and six EPSI subscales, as the T hi s do cu m en t is co py ri gh te d by th e
- 85. t to be di ss em in at ed br oa dl y. 180 CHRISTIAN ET AL. EPSI was designed as a multidimensional measure of eating pa- thology, rather than a global subscale of severity (Forbush et al., 2013). A post hoc Bonferroni correction was used for multiple comparisons. The cutoff value after this correction is p � .007. Results Networks and Stability See Figure 1 for EPSI networks and Figure 2 for EDE-Q networks. Table 2 includes descriptions of each of the EPSI and
- 86. EDE-Q items. Stability for strength was excellent (strength � .75) for all the EPSI and EDE-Q networks (Epskamp, Borsboom, & Fried, 2018). Central Symptoms EPSI. See Figure 3 for the strength centrality of all symptoms in the EPSI networks. All central symptoms were significantly more central than other symptoms in the network at p � .05. Overeating and feeling full after eating a small amount of food emerged as central symptoms across every developmental stage. Avoiding high calorie foods and planning days around exercise are central symptoms in late adolescence, young adulthood, early- middle adulthood, and middle-late adulthood. Fasting is a central symptom in early adolescence, late adolescence, young adulthood, and early-middle adulthood. Stuffing oneself to the point of feeling sick is a central symptom in young adulthood, early-middle adult- hood, and middle-late adulthood. The most central symptoms in the EPSI networks are described in Table 3. EDE-Q. See Figure 4 for the strength centrality of all symp- toms in the EDE-Q networks. All central symptoms were signif- icantly more central than other symptoms in the network at p � .05. Desire for an empty stomach emerged as a central symptom across every developmental stage. Concentration prob- lems due to weight and shape is a central symptom in early adolescence, late adolescence, young adulthood, and early- middle
- 87. A. Early Adolescence B. Late Adolescence C. Young Adulthood D. Early-middle Adulthood E. Middle-late Adulthood clothesfit unhealthyfood nothungry eatlittle exercisedaily supriseeat exercisehard snacking fulleasy thinkdiuretics outfits thinklaxatives dietteas dietpills dislikebody full countcals
- 96. hips eatmore resist stuffed avoidhighcal exerciseexhaust diureticsuse fast autopilot overeat Figure 1. EPSI networks for (A) early adolescence (11–14), (B) late adolescence (15–18), (C) young adulthood (19 –25), (D) early-middle adulthood (26 – 45), and (E) middle- late adulthood (46�). Blue (solid) edges represent positive partial correlations. Red (dashed) lines represent negative partial correlations. Line thickness represents the strength of the partial correlation. See Table 2 for EPSI items corresponding to each node. See the online article for the color version of this figure. T hi s do cu
- 101. dl y. 181EATING DISORDER AGE NETWORKS adulthood. Feeling dissatisfied about one’s weight is a central symptom in early adolescence, young adulthood, early-middle adult- hood, and middle-late adulthood. Overeating is a central symptom in late adolescence, young adulthood, early-middle adulthood, and middle-late adulthood. Desire to lose weight is a central symptom in early and late adolescence. Judgment of self due to shape is a central symptom in early adolescence. Binge eating is a central symptom in young adulthood. Dissatisfaction about one’s shape is a central symp- tom in middle-late adulthood. The most central symptoms in the EDE-Q networks are described in Table 4. EPSI networks. The network invariance test indicated that the early adolescence network was significantly different than late ado- lescence (M � 0.12, p � .05), young adulthood (M � 0.52, p � .05), early-middle adulthood (M � 0.23, p � .001), and middle-late adult- hood (M � 0.29, p � .001). The late adolescence network was significantly different from early-middle adulthood (M � 0.17, p � .001) and middle-late adulthood (M � 0.24, p � .001), but not
- 102. young adulthood (p � .05). The young adulthood network was not signifi- cantly different from early-middle adulthood or middle-late adulthood (p � .05). The early-middle adulthood network was significantly different than middle-late adulthood (M � 0.10, p � .02). The edge invariance test indicated that two edges were significantly different (p � .05) between early adolescence and late adolescence, one edge significantly differed between early adolescence and young adulthood, 16 edges significantly differed between early adolescence and early-middle adulthood, 13 edges significantly differed between early adolescence and middle-late adulthood, 20 edges significantly differed between late adolescence and early-middle adulthood, 19 edges significantly differed between late adolescence and middle-late adulthood, and two edges significantly differed between early- middle adulthood and middle-late adulthood. See online supplemental mate- rials for all significantly different edges and corresponding E- values. The Global Strength Invariance test indicated that there were no significant differences in global strength among the EPSI networks of different developmental stages (p � .05).
- 103. EDE-Q. The structure of the early adolescence network was significantly different than young adulthood (M � 0.15, p � .001), early-middle adulthood (M � 0.17, p � .001), and middle-late adult- A. Early Adolescence B. Late Adolescence C. Young Adulthood D. Early-middle Adulthood E. Middle-late Adult Adulthood restrict fast excludefood foodrules emptystomach flatstomach foodconc wsconc losecontrolfeargain feelfat desirelose overeat binge
- 110. shapejudge weighself weighdiss shapediss seeself otherseebody Figure 2. EDE-Q networks for (A) early adolescence (11–14), (B) late adolescence (15–18), (C) young adulthood (19 –25), (D) early-middle adulthood (26 – 45), and (E) middle-late adulthood (46�). Blue (solid) edges represent positive partial correlations. Red (dashed) lines represent negative partial correlations. Line thickness represents the strength of the partial correlation. See Table 2 for EDE-Q items corresponding to each node. See the online article for the color version of this figure. T hi s do cu m en t is co
- 114. du al us er an d is no t to be di ss em in at ed br oa dl y. 182 CHRISTIAN ET AL. http://dx.doi.org/10.1037/abn0000477.supp
- 115. http://dx.doi.org/10.1037/abn0000477.supp Table 2 Network Node (i.e., Symptom) Abbreviations EPSI clothesfit Dislike how clothes fit unhealthyfoods Attempt to exclude “unhealthy” foods nothungry Ate when not hungry eatlittle Told that I do not eat much exercisedaily Felt the need to exercise nearly daily supriseeat People would be surprised by how little I ate exercisehard Push myself hard when exercising snacking Snacked without realizing fulleasy Got full easily thinkdiuretics Considered taking diuretics outfits Tried on different outfits because of how I looked thinklaxatives Thought laxatives are good to lose weight dietteas Used diet teas or cleansing teas dietpills Used diet pills dislikebody Dislike how my body looked full Ate until uncomfortably full countcals Counted calories planexercise Planned days around exercising butt Thought butt was too big thighs Dislike size of thighs shapediff Wished shape of body was different vomit Vomited to lose weight noticeate Did not notice how much I ate until after strenexercise Engaged in strenuous exercise at least 5 days per week fullsmall Got full after eating a small amount of food hips Dissatisfied with the size of hips eatmore Others encouraged to eat more
- 116. resist Felt I could not resist eating food offered stuffed Stuffed myself with food avoidhighcal Tried to avoid foods with high calories exerciseexhaust Exercised to exhaustion diureticsuse Used diuretics to lose weight fast Skipped two meals in a row autopilot Ate on autopilot overeat Ate a large amount of food in a short period of time EDE-Q restrict Tried to limit the amount of food eaten for shape or weight concerns fast Gone for long periods of time without eating for shape or weight concerns excludefood Tried to exclude foods that you like for shape or weight concerns foodrules Tried to follow food rules for shape or weight concerns emptystomac Definite desire to have an empty stomach flatstomach Definite desire to have a flat stomach foodconc Thinking about food, eating, or calories made it difficult to concentrate wsconc Thinking about shape or weight made it difficult to concentrate losecontrol Definite fear of losing control overeating feargain Fear that you might gain weight feelfat Felt fat desirelose Strong desire to lose weight overeat Ate an unusually large amount of food binge Had a sense of losing control over your eating and ate an unusually large amount of food vomit Made yourself sick (vomit) for shape or weight concerns laxatives Taken laxatives for shape or weight concerns compex Exercised in a “driven” or “compulsive” way for shape or weight concerns
- 117. eatsecret Ate in secret guilty Felt guilty for eating due to shape or weight concerns otherseeeat Concerned about other people seeing you eat weightjudge Weight influenced self-judgment shapejudge Shape influenced self-judgment weighself Upset if had to weigh once a week weightdiss Dissatisfied with weight shapediss Dissatisfied with shape seeself Discomfort seeing your own body otherseebody Discomfort with others seeing your body T hi s do cu m en t is co py ri gh te d by th
- 121. no t to be di ss em in at ed br oa dl y. 183EATING DISORDER AGE NETWORKS hood (M � 0.17, p � .01), but not late adolescence. The late adolescence network was significantly different from young adult- hood (M � 0.07, p � .05), early-middle adulthood (M � 0.10, p � .001), and middle-late adulthood (M � 0.16, p � .001). The young adulthood network was significantly different than middle-late adult- hood (M � 0.14, p � .05), but not early-middle adulthood. The
- 122. early-middle adulthood network was not significantly different than middle-late adulthood. Eight edges were significantly different (p � .05) between early adolescence and young adulthood, 20 edges significantly differed between early adolescence and early-middle adulthood, 23 edges significantly differed between early adolescence and middle- late adulthood, 12 edges significantly differed between late adoles- cence and young adulthood, 13 edges significantly differed be- tween late adolescence and early-middle adulthood, 19 edges significantly differed between late adolescence and middle-late adulthood, and seven edges significantly differed between young adulthood and middle-late adulthood. See online supplemental materials for all significantly different edges and corresponding E-values. Figure 3. Centrality of EPSI symptoms for the (A) early adolescence, (B) late adolescence, (C) young adulthood, (D) early-middle adulthood, and (E) middle-late adulthood networks. Red (large) dots denote most central symptoms. See Table 2 for EPSI items corresponding to each node abbreviation. See the online article for the color version of this figure. Table 3 EPSI Central Symptoms Early adolescence Late adolescence Young adulthood Early- middle adulthood Middle-late adulthood
- 123. Overeat (1.88) Overeat (1.68) Overeat (1.72) Overeat (1.58) Overeat (1.98) Fullsmall (2.35) Fullsmall (1.45) Fullsmall (1.88) Fullsmall (1.92) Fullsmall (1.82) Avoidhighcal (1.54) Avoidhighcal (1.44) Avoidhighcal (1.72) Avoidhighcal (1.47) Planexercise (1.29) Planexercise (1.57) Planexercise (1.69) Planexercise (1.30) Fast (1.75) Fast (2.53) Fast (2.19) Fast (1.27) Stuffed (1.44) Stuffed (1.89) Stuffed (1.87) Note. Standardized strength centrality coefficients included in parentheses. All symptoms in the table were significantly more central than over 75% of other symptoms in the network. See Table 2 for EPSI items corresponding to each node abbreviation. T hi s do cu m en t is co py ri
- 127. us er an d is no t to be di ss em in at ed br oa dl y. 184 CHRISTIAN ET AL. http://dx.doi.org/10.1037/abn0000477.supp http://dx.doi.org/10.1037/abn0000477.supp
- 128. The early adolescence network (global strength � 11.82) had significantly lower global strength than middle-late adulthood (global strength � 12.56; GSI � 0.74, p � .05). Late adolescence (global strength � 12.73) had significantly lower strength than young adult- hood (global strength � 13.48; GSI � 0.75, p � .01) and early- middle adulthood (global strength � 13.61; GSI � 0.89, p � .05). There were no other significant differences in global strength among the EDE-Q networks (p � .05). See Table 5 for an overview of network differences across developmental stages. ANOVA Across Developmental Stages The results of the one-way ANOVAs indicated a significant main effect of group for body dissatisfaction, F(4, 29,897) � Figure 4. Centrality of EDE-Q symptoms for the (A) early adolescence, (B) late adolescence, (C) young adulthood, (D) early-middle adulthood, and (E) middle-late adulthood networks. Red (large) dots denote most central symptoms. See Table 2 for EDE-Q items corresponding to each abbreviation. See the online article for the color version of this figure. Table 4 EDE-Q Central Symptoms Early adolescence Late adolescence Young adulthood Early- middle adulthood Middle-late adulthood Emptystomach� (.98) Emptystomach�� (1.11)
- 129. Emptystomach�� (1.30) Emptystomach�� (1.72) Emptystomach�� (1.73) Wsconc�� (1.48) Wsconc�� (1.13) Wsconc� (1.07) Wsconc�� (1.13) Overeat� (1.32) Overeat�� (1.43) Overeat�� (1.56) Overeat� (1.11) Weightdiss� (.98) Weightdiss�� (1.13) Weightdiss�� (1.41) Weightdiss� (1.09) Desirelose� (.95) Desirelose� (1.05) Shapejudge� (1.30) Binge� (.99) Shapediss� (1.11) Note. Standardized strength centrality coefficients included in parentheses. � Symptom is significantly more central than over 50% of other symptoms in the network. �� Symptom is significantly more central than over 75% of other symptoms in the network. See Table 2 for EDE-Q items corresponding to each node abbreviation. T hi s do cu m en t is
- 133. vi du al us er an d is no t to be di ss em in at ed br oa dl y. 185EATING DISORDER AGE NETWORKS
- 134. 10.03, cognitive restraint, F(4, 29,897) � 183.28, binge eating, F(4, 29,897) � 183.28, purging, F(4, 29,897) � 189.43, restric- tion, F(4, 29,897) � 700.49, excessive exercise, F(4, 29,897) � 215.31, and global ED symptoms, F(4, 32,214) � 107.64, p � .001. Post hoc pairwise comparisons indicated that body dissatis- faction was highest in late adolescence, young adulthood, and early-middle adulthood. Purging was highest in late adolescence and young adulthood. Restriction, excessive exercise, cognitive restraint, and global ED symptoms were highest in early adoles- cence and significantly declined across development. Binge eating was lowest in early adolescence and significantly increased across development. See Table 6 for means and standard deviations for these measures across each developmental stage. Discussion This study utilizes NA to explore ED symptoms across funda- mental developmental stages of adolescence and adulthood in a large sample of Recovery Record users. We hypothesized that central symptoms would be consistent across developmental stages but that the individual connections or pathways (edges) between symptoms may differ in strength. In support of our hypothesis, several symptoms emerged as central across all or most develop- mental stages. In partial support of our second hypothesis, there were significant differences in the network structure for all ED networks across both measures, but only significant differences in global strength among some of the EDE-Q networks. However, the
- 135. results of the ANOVA contradicted these findings, as for most ED symptoms, excluding binge eating, symptom severity was highest for adolescence and young adulthood and declined later in adult- hood, suggesting that the strength of the connections (but not the severity of symptoms) may increase across development. Overall, these network comparison results suggest that although many of the central symptoms remain consistent across developmental stages, the connections among symptoms significantly differ. Central Symptoms Several symptoms, including overeating and cognitions related to fullness, were central symptoms at every developmental stage. Several additional symptoms were central in four of the five networks, including symptoms related to food avoidance, overeat- ing, and overvaluation of weight and shape. The high proportion of symptoms that were central across most or all developmental stages suggests that these ED symptoms may be central regardless of developmental stage. Thus, these symptoms may represent important targets for intervention for individuals with EDs across all developmental stages. Some symptoms were unique to one or two developmental stages, including additional symptoms related to overvaluation of weight and shape (e.g., dissatisfaction about one’s shape; desire to lose weight). These symptoms may
- 136. represent unique targets of intervention for the treatment of EDs in specific age populations. Additionally, many of the central symptoms represent symp- toms related to overvaluation of weight and shape, including concentration problems due to weight and shape, dissatisfaction Table 5 Network Comparison Tests Early adolescence Late adolescence Young adulthood Early-middle adulthood Middle-late adulthood Developmental stage M GSI M GSI M GSI M GSI M GSI Early adolescence — — .11 .92 .15� 1.67 .17� 1.80 .18� .75� Late adolescence .12� .81 — — .07� .75� .10� .88� .17� .17 Young adulthood .52� 2.88 .52 2.07 — — .06 .13 .14� .92 Early-middle adulthood .23� 1.60 .17� .78 .49 1.29 — — .12 1.05 Middle-late adulthood .29� .33 .24� .48 .51 2.55 .10� 1.26 — — Note. Bottom left (not bold) values represent network comparisons among EPSI networks. Upper right (bold) values represent network comparisons among EDE-Q networks. M � network invariance test statistic;
- 137. GSI � global strength invariance test statistic. � p � .05. Table 6 Means and Standard Deviations of Study Measures Across Developmental Stages Outcome Early adolescence Late adolescence Young adulthood Early-middle adulthood Middle-late adulthood EDE-Q global 4.32 (1.07) 4.29 (1.07) 4.18 (1.11) 4.05 (1.10) 3.73 (1.14) EPSI body dissatisfaction 20.70 (6.29) 21.36 (5.67) 21.19 (5.88) 21.36 (6.05) 20.59 (6.40) EPSI cognitive restraint 8.26 (3.30) 8.11 (3.14) 7.84 (3.09) 7.20 (3.12) 6.44 (2.90) EPSI binge eating 12.39 (9.04) 15.62 (9.37) 16.71 (9.37) 17.95 (9.02) 17.58 (8.16) EPSI purging 5.63 (5.94) 6.58 (5.92) 6.10 (5.88) 5.08 (5.49) 3.08 (4.34) EPSI restriction 13.98 (6.25) 12.62 (6.37) 10.75 (6.49) 8.22 (6.49) 6.91 (5.69) EPSI excessive exercise 9.71 (5.81) 9.08 (5.65) 8.63 (5.82) 7.44
- 138. (5.67) 5.71 (4.82) Note. Values reported as M (SD). Italicized values were not significantly different (p � .007) than at least one other developmental stage. Bolded values denote stages significantly different than three or more other developmental stages. T hi s do cu m en t is co py ri gh te d by th e A
- 142. to be di ss em in at ed br oa dl y. 186 CHRISTIAN ET AL. about one’s weight, dissatisfaction about one’s shape, judgment about one’s shape, and desire to lose weight. This finding is consistent with past conceptualizations of eating pathology using NA (DuBois et al., 2017; Forrest et al., 2018; Levinson et al., 2017; Wang et al., 2018) and supports the theory that overvalu- ation of weight and shape are core ED symptoms (Fairburn, 2008). A few symptoms that were highly central, including overeating and food avoidance, had not previously emerged as central in past studies. Thus, more research should test if these results replicate in
- 143. other samples. Differences Across Development Despite the number of central symptoms that remained similar across developmental stages, the network comparison tests re- vealed significant differences in how symptoms were related across networks. The adolescent networks for both the EDE-Q and EPSI were significantly different from all the adulthood networks, suggesting that symptom relationships during adolescence signif- icantly vary from adulthood. Additionally, the networks represent- ing stages of adulthood were significantly different from each other for both measures, indicating that symptom relationships also are highly variable across the developmental stages of adulthood. The edge invariance tests supported these findings, as there were many significantly different edges across networks. All signifi- cantly different edges are included in online supplemental mate- rials, as these edges represent pathways that may be differently important across developmental stages and provide insight into the clinical significance of network structure differences. Overall, these findings suggest that important illness pathways may change across development, indicating that clinicians should expect fluctuations in the relationships among ED symptoms that occur with time and life experiences and that these changes may alter intervention targets. For example, fear of weight gain may
- 144. be a common driving symptom across stages of development, but it may manifest differently over time (e.g., restriction may be more prevalent early on, but later shifts to judgment fears and isolation). Therefore, interventions may need to be tailored to address such changes. In terms of global strength, only the EDE-Q networks exhibited significant differences, with trends indicating global strength in- creases for networks with older participants compared to younger participants. Higher global strength is theorized to be representa- tive of greater severity (Pe et al., 2015; van Borkulo et al., 2015). However, comparisons in EDE-Q global scores and EPSI subscale scores across stages of development indicated that symptoms (based on total symptom scores) were more severe (i.e., higher) in the adolescent and young adult groups for all symptoms except binge eating. Bos et al. (2018) also found increased network connectivity corresponding with decreased severity, contrary to findings by van Borkulo et al. and Pe et al. As such, global strength may not necessarily correspond to greater overall severity of symptoms, but instead tighter connections between symptoms. The high interconnectivity of symptoms in the later developmental stages may be attributed to the longer average duration of illness of older individuals with EDs in our sample, which would likely indicate stronger, more reinforced pathways among symptoms,
- 145. as suggested by Habit Formation Theory (Walsh, 2013). Contrary to this finding, no significant differences in the global strength emerged across EPSI networks. This result was surpris- ing, as the network comparison test detects even small differences. However, group comparisons indicated that some symptoms (e.g., binge eating) were stronger for older ages and other symptoms (e.g., restriction) were stronger in younger ages, so these opposing trends potentially “cancelled” each other out in the summation of strength across networks. It is also possible that this is an artifact of different measurement techniques that should be investigated in future research. Given the conflicting findings in the literature, future research should investigate how symptom interconnectivity (vs. symptom severity) may contribute to course of illness and outcomes. Limitations This study examines ED symptoms across developmental stages in the largest clinical ED sample used for NA to date, providing important insight into how ED symptomology may change across development. However, this study has limitations. One limitation is the missing diagnostic information in the data sets, which prevented us from using diagnosis-matched samples for each de- velopmental stage. Recovery record only provides participant di-
- 146. agnostic information when the application is connected with a clinician, which was only applicable for 27.0 –48.7% of the EPSI participants and 1.4 –9.7% of the EDE-Q participants. Among the participants that did have ED diagnoses, there were significant differences in diagnoses across developmental stages. For exam- ple, in the EPSI network, the early adolescence group was primar- ily comprised of anorexia nervosa (55.3% of individuals with a clinician-provided diagnosis), and the middle-late adulthood group was primarily comprised of binge eating disorder (52.6% of indi- viduals with a clinician-provided diagnosis). Due to these differ- ences, it is possible that some of the network differences we found may be attributed to diagnostic differences as opposed to devel- opmental stage. Future research should use diagnosis-matched samples to test if our findings replicate. However, despite differ- ences in diagnoses across networks, many symptoms remained central across all networks. This finding supports the idea that despite differential diagnoses, EDs are transdiagnostic phenomena (Cooper & Dalle Grave, 2017; Lampard, Tasca, Balfour, & Bis- sada, 2013). Additionally, the ubiquity of core symptoms across diagnoses could contribute to the high diagnostic crossover in EDs (Castellini et al., 2011; Fichter & Quadflieg, 2007). Further, because of the low prevalence of individuals above 46 that used the Recovery Record application, the middle-late adults network spans several decades (46 –79 years of age). Thus, this
- 147. study is unable to contribute to parsing out ED symptom differ- ences across this large developmental category. Additional re- search should be conducted in middle and older adults, focused on identifying developmental differences in ED symptoms. Further, given that this is the first investigation of EDs across development from early adolescence to late adulthood, there are no established guidelines for distinct developmental periods in this population. Our categories are based on non-ED-specific developmental the- ories. Future research may refine these periods to ensure they reflect distinct stages of development for this population. Addi- tionally, data were self-reported from the Recovery Record app and limited by self-awareness and self-report biases. Two sub- T hi s do cu m en t is co py ri gh te
- 151. an d is no t to be di ss em in at ed br oa dl y. 187EATING DISORDER AGE NETWORKS http://dx.doi.org/10.1037/abn0000477.supp http://dx.doi.org/10.1037/abn0000477.supp scales of the EPSI, Muscle Building and Negative Attitudes To- ward Obesity, were not measured in the Recovery Record app, so
- 152. it is unknown how these constructs might vary across develop- mental stages. One primary concern with NA is that there is currently no empirical method for selecting items for inclusion. As depicted by differences in central symptoms and connections across the EPSI and EDE-Q, item inclusion can critically impact interpretation of the network. For example, the EPSI, comprised of more behavioral ED symptoms, had more behavioral symptoms emerge as central, as compared to the EDE-Q. Future research should develop and validate empirical methods of selecting items for a network and developing measures designed to perform well in NA. Researchers have also expressed concerns with sole reliance on centrality indices to determine central symptoms (see Bringmann & Eronen, 2018; Hallquist, Wright, & Molenaar, 2019). However, in general, many researchers have suggested that central symptoms may serve as useful targets for future interventions (McNally, 2016; Rode- baugh et al., 2018), and growing empirical data shows that central symptoms predict important outcomes, specifically in EDs (Elliott et al., 2018; Olatunji et al., 2018). Finally, these networks were conducted at the group level, so findings indicate trends across developmental stages and may not be representative of symptom relationships for an individual over time. Implications and Future Research
- 153. This study examines ED symptoms across developmental stages in a large clinical ED sample, which has broad implications for future research and treatment development for individuals with EDs. Significant network differences across stages suggest that ED research should be inclusive of individuals from all ages, espe- cially older populations, who are typically left out of studies on treatment development (Forman & Davis, 2005). Additionally, differences across stages of development may impact treatment needs for subpopulations of EDs. For example, as symptom con- nections change in older populations, treatments may need to be adapted to focus on the strongest connections in order to disrupt the most salient illness pathways. Treatments for older individuals with EDs must also take into consideration the increased connec- tivity of symptoms, which may be contributing to the worse treatment outcomes for this population (Noordenbos et al., 2002; Norring & Sohlberg, 1993). In addition, symptoms that are central to eating pathology across developmental stages, including items related to overeating, feel- ings of fullness, food avoidance, and overvaluation of weight and shape, are hypothesized to be good targets for intervention for individuals of all ages with EDs. Interventions that target these symptoms, including cognitive– behavioral and dialectical– behavior therapy interventions, such as thought challenging, ex- posure therapy, distress tolerance, and behavior chaining, are widely used and are among the most effective and empirically supported treatments for EDs (Fairburn, 2008; Linehan & Chen, 2005). Feelings of fullness can also be addressed using