

Recommended
More Related Content
What's hot
What's hot (20)
Similar to 4.intestine3
Similar to 4.intestine3 (20)
More from PNK SINGH
More from PNK SINGH (20)
Recently uploaded
Recently uploaded (20)
4.intestine3
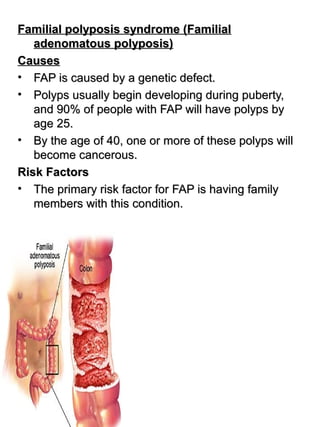
- 1. Familial polyposis syndrome (FamilialFamilial polyposis syndrome (Familial adenomatous polyposis)adenomatous polyposis) CausesCauses • FAP is caused by a genetic defect.FAP is caused by a genetic defect. • Polyps usually begin developing during puberty,Polyps usually begin developing during puberty, and 90% of people with FAP will have polyps byand 90% of people with FAP will have polyps by age 25.age 25. • By the age of 40, one or more of these polyps willBy the age of 40, one or more of these polyps will become cancerous.become cancerous. Risk FactorsRisk Factors • The primary risk factor for FAP is having familyThe primary risk factor for FAP is having family members with this condition.members with this condition.
- 2. Morphologic and molecular changes in the adenoma-carcinoma sequence- note the Knudson’s two hit hypothesis
- 3. Familial polyposis syndrome (FamilialFamilial polyposis syndrome (Familial adenomatous polyposis)adenomatous polyposis) 1. Familial Polyposis Coli (Large Bowel)1. Familial Polyposis Coli (Large Bowel) • Large no of neoplastic polyps in the colonLarge no of neoplastic polyps in the colon • risk of colonic cancer is virtually 100% by midlife,risk of colonic cancer is virtually 100% by midlife, unless a prophylactic colectomy is performedunless a prophylactic colectomy is performed Familial colonic polyposis with adenocarcinoma
- 4. 2. Gardner syndrome2. Gardner syndrome Adenomatous polyps of large bowel associated withAdenomatous polyps of large bowel associated with one or more of:one or more of: • multiple osteomas of skull and mandiblemultiple osteomas of skull and mandible • epidermal cysts of skinepidermal cysts of skin • soft tissue neoplasms, usually intra-abdominalsoft tissue neoplasms, usually intra-abdominal 3. Turcot syndrome (rare) –3. Turcot syndrome (rare) – • Colorectal adenomatous polyps associated withColorectal adenomatous polyps associated with brain tumorsbrain tumors
- 5. Familial adenomatous polyposis. The surface is carpeted by innumerable polypoid adenomas
- 6. Colorectal cancerColorectal cancer Most ca originate in rectum, rectosigmoid & sigmoidMost ca originate in rectum, rectosigmoid & sigmoid coloncolon Risk factorsRisk factors Diet plays an important roleDiet plays an important role • Low vegetable fiber content leads to decreasedLow vegetable fiber content leads to decreased stool bulk & increased faecal transient timestool bulk & increased faecal transient time • High fat intake leads to increased systhesis ofHigh fat intake leads to increased systhesis of cholesterol & bile acids by the liver which may becholesterol & bile acids by the liver which may be converted into carcinogens by intestinal bacteriaconverted into carcinogens by intestinal bacteria • High content of refined carbohydrates from whichHigh content of refined carbohydrates from which toxic products are produced which are risk factorstoxic products are produced which are risk factors
- 7. MorphologyMorphology Left sided carcinomaLeft sided carcinoma • Tumors in the proximal colon tend to grow asTumors in the proximal colon tend to grow as polypoid, exophytic masses without obstructivepolypoid, exophytic masses without obstructive symptomssymptoms Righted sided carcinomaRighted sided carcinoma • Distal colon cancer tend to be annular, encirclingDistal colon cancer tend to be annular, encircling lesions that produce so-called “napkin-ring”lesions that produce so-called “napkin-ring” constrictions of the bowel and narrowing of theconstrictions of the bowel and narrowing of the lumenlumen • There may be ulcerationThere may be ulceration
- 8. Cecal carcinoma The exophytic carcinoma projects into the lumen but has not caused obstruction.
- 9. Carcinoma of the descending colon. This circumferential tumor has heaped-up edges and an ulcerated central portion. The arrows identify separate mucosal polyps
- 10. HistologyHistology • Almost all are adenocarcinomas that range fromAlmost all are adenocarcinomas that range from well-differentiated to undifferentiated, franklywell-differentiated to undifferentiated, frankly anaplasticanaplastic • Many tumors produce mucin, which is secretedMany tumors produce mucin, which is secreted into the gland lumina or into the interstitiuminto the gland lumina or into the interstitium • Cancers of the anal zone are predominantlyCancers of the anal zone are predominantly squamous cell in originsquamous cell in origin
- 11. 1111 The red arrows point to normal crypts. • The blue arrows point to malignant glands which are growing both beneath the normal mucosa and on the right side of the picture up into the mucosa. • The normal crypts show some technical artifacts
- 12. Invasive adenocarcinoma of colon showing malignant glands infiltrating the muscle wall.
- 13. Clinical featuresClinical features • Right sided lesions present with fatigue,Right sided lesions present with fatigue, weakness, and iron deficiency anemiaweakness, and iron deficiency anemia • Left-sided lesions may produce occult bleeding,Left-sided lesions may produce occult bleeding, changes in bowel habit, or crampy left lowerchanges in bowel habit, or crampy left lower quadrant discomfortquadrant discomfort • the favored sites for metastasis are the regionalthe favored sites for metastasis are the regional lymph nodes, liver, lungs, and boneslymph nodes, liver, lungs, and bones • DiagnosisDiagnosis – digital rectal examinationdigital rectal examination – fecal testing for occult blood lossfecal testing for occult blood loss – barium enema,barium enema, – sigmoidoscopy, and colonoscopy requiresigmoidoscopy, and colonoscopy require confirmatory biopsyconfirmatory biopsy – Computed tomography to assess metastaticComputed tomography to assess metastatic spreadspread – carcinoembryonic antigen: nonspecific, alsocarcinoembryonic antigen: nonspecific, also raised in carcinomas of the lung, breast, ovary,raised in carcinomas of the lung, breast, ovary, urinary bladder, and prostate, as well asurinary bladder, and prostate, as well as alcoholic cirrhosis, pancreatitis, and ulcerativealcoholic cirrhosis, pancreatitis, and ulcerative colitiscolitis
- 14. TNM staging:TNM staging: • Tumor (T)Tumor (T) – T0 = none evidentT0 = none evident – Tis = in situ (limited to mucosa)Tis = in situ (limited to mucosa) – T1 = invasion of lamina propria or submucosaT1 = invasion of lamina propria or submucosa – T2 = invasion of muscularis propriaT2 = invasion of muscularis propria – T3 = invasion through muscularis propria intoT3 = invasion through muscularis propria into subserosa or nonperitonealized perimuscularsubserosa or nonperitonealized perimuscular tissuetissue – T4 = invasion of other organs or structuresT4 = invasion of other organs or structures
- 15. • Lymph Nodes (N)Lymph Nodes (N) – 0 = none evident0 = none evident – 1 = 1 to 3 positive pericolic nodes1 = 1 to 3 positive pericolic nodes – 2 = 4 or more positive pericolic nodes2 = 4 or more positive pericolic nodes • 3 = any positive node along a named blood3 = any positive node along a named blood vesselvessel • Distant Metastases (M)Distant Metastases (M) – 0 = none evident0 = none evident – 1 = any distant metastasis1 = any distant metastasis
- 16. SpreadSpread • Local invasion or direct extension into adjacentLocal invasion or direct extension into adjacent struturesstrutures • Distant Spread – Metastatis occurs through theDistant Spread – Metastatis occurs through the lymphatics & blood vesselslymphatics & blood vessels • Regional lymph nodes, liver, lungs & bones,Regional lymph nodes, liver, lungs & bones, peritoneum ectperitoneum ect
- 17. AppendicitisAppendicitis • Definition -Definition - Acute inflammation of the appendix,Acute inflammation of the appendix, AetiologyAetiology Exact cause is unknown. Contributory factors areExact cause is unknown. Contributory factors are • Age – mostly less than 10 years & adolescentAge – mostly less than 10 years & adolescent A. Obstructive agentsA. Obstructive agents 1. In Lumen of appendix –1. In Lumen of appendix – • FaecolithFaecolith • Threadworm or round wormThreadworm or round worm • Foreign bodyForeign body • True calculus, gallstoneTrue calculus, gallstone Dr S ChakradharDr S Chakradhar 1717
- 19. 2. in the wall2. in the wall • Hyperplasia of lymphoid tissueHyperplasia of lymphoid tissue • Extension of tumour of caecum, or primary tumorExtension of tumour of caecum, or primary tumor of appendixof appendix 3. Outside the wall3. Outside the wall • Compression by bands, adhesionCompression by bands, adhesion Mixed infectionMixed infection • with E Coli (85%A), enterococci, clostridiumwith E Coli (85%A), enterococci, clostridium perfringes & bacteroids are formed in inflammaedperfringes & bacteroids are formed in inflammaed appendixappendix 1919
- 20. PathogenesisPathogenesis According to obstruction to lumenAccording to obstruction to lumen • Non obstructiveNon obstructive • ObstructiveObstructive Non ObstructiveNon Obstructive Sequelae may beSequelae may be • ResolutionResolution • UlcerationUlceration • SuppurationSuppuration • Gangrene of the tip due to arterial occlusion byGangrene of the tip due to arterial occlusion by inflammation or thrombosisinflammation or thrombosis • FibrosisFibrosis Dr S ChakradharDr S Chakradhar 2020
- 21. ObstructiveObstructive • After obstruction, continuing secretion increasesAfter obstruction, continuing secretion increases intra luminal pressureintra luminal pressure • which causes collapse of veins & ischemic injurywhich causes collapse of veins & ischemic injury • followed by bacterial invasionfollowed by bacterial invasion • ischemic and septic necrosis,ischemic and septic necrosis, Gangrene or perforation is more common & rapidGangrene or perforation is more common & rapid 2121
- 22. MorphologyMorphology 1. Early acute appendicitis1. Early acute appendicitis GrossGross • Congestion. Serosa is read in appearanceCongestion. Serosa is read in appearance (dilatation)(dilatation) MicroMicro • Scanty neutrophil exudation throughout the mucosa,Scanty neutrophil exudation throughout the mucosa, submucosa & muscularissubmucosa & muscularis 2222
- 23. 2. Acute diffuse suppurative appendicitis (later2. Acute diffuse suppurative appendicitis (later stage )stage ) GrossGross • Dilated lumen, thickened wall, dusky discoloration ofDilated lumen, thickened wall, dusky discoloration of serosa,serosa, • fibrinous or fibrinopurulent serosal exudatefibrinous or fibrinopurulent serosal exudate MicroMicro • Marked neutrophil infiltration if the entire wallMarked neutrophil infiltration if the entire wall • There may be abscess formation & ulceration ofThere may be abscess formation & ulceration of mucosamucosa 2323
- 24. 2424 •Granular roughened serosa with marked congestion at tip (yellow arrow) •Grey yellow purulent exudate on the surface (green arrows) •Marked increase in diameter •The cross sectioned end appears dilated and the wall appears thickened and edematous •The serosa is congested with yellow plaques of exudate (arrow) •The serosal surface of the intact appendix shows
- 25. C.Acute gangrenous appendicitisC.Acute gangrenous appendicitis GrossGross • Distal part or large areas become gangrenous &Distal part or large areas become gangrenous & looks blacklooks black • It may ruptureIt may rupture MicroMicro • The histological picture of Extensive necrosis ofThe histological picture of Extensive necrosis of mucosa and muscularis, with microabscesses withinmucosa and muscularis, with microabscesses within the appendiceal wallthe appendiceal wall 2525Rupture of appendix secondary to transmural acute appendicitis. 0 5 0 1 0 0 第 一 季 度 第 四 季 度 东 部 西 部 北 部
- 26. 2626 Area of acute necrosis within the wall of the appendix in the setting of acute appendicitis. The mucosa on the left is totally necrotic and infiltrated by polys in contrast to the normal viable mucosa on the right which shows no necrosis
- 27. Acute appendicitisAcute appendicitis • Loss of continuity of mucosal lining in someLoss of continuity of mucosal lining in some places indicating mucosal ulceration or sloughingplaces indicating mucosal ulceration or sloughing • Infiltration of acute inflammatory cellsInfiltration of acute inflammatory cells (polymorphs) in all layers including muscle coats(polymorphs) in all layers including muscle coats • The lumen also contains inflammatory exudateThe lumen also contains inflammatory exudate Dr S ChakradharDr S Chakradhar 2727
- 28. 2828
- 29. 2929
- 30. 4 major causes of bowel obstruction
- 31. Hernia – InguinalHernia – Inguinal
- 32. Diverticulosis : • protrusion of mucosa and submucosa through the muscle wall.
- 35. 3535 A) which is superior the appendix. CT image “B” is distal to the ileocecal junction. It shows a swollen appendix due to acute appendicitis. The appendix is easier to see because it is fluid filled. This axial slice also demonstrates the location of the appendix, which is posteromedial in this patient and about 2.5 cm below the ileocecal junction.
- 36. 3636
- 37. 3737