Hydatid cyst
•Download as PPTX, PDF•
9 likes•2,308 views

kathmandu medical college, department of surgery

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Hydatid cyst
Similar to Hydatid cyst (20)
More from Youttam Laudari
More from Youttam Laudari (20)
Recently uploaded
Recently uploaded (20)
Hydatid cyst
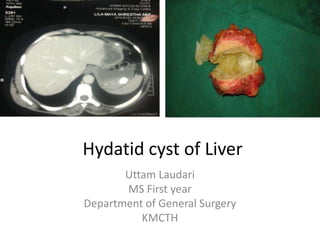
- 1. Hydatid cyst of Liver Uttam Laudari MS First year Department of General Surgery KMCTH
- 2. Objective • Introduction of H. Cyst • Review of life cycle • Pathology • Fate of H. Cyst • Investigations
- 3. Echinococcosis (hydatidosis, hydatid disease) • Zoonosis • Organism- larval (metacestode) stages of cestodes (flat worms) • genus -Echinococcus • family -Taeniidae • Definitve host-carnivores • animals are both intermediate and definitive hosts • Humans are the accidental intermediate host (dead end)
- 4. • The first North American case was observed in 1808 and published in 1822. The true nature of the disease was not known until the second half of the 19th century.
- 5. • There are three known forms of echinococcosis in humans: • (i) cystic echinococcosis (hydatid disease) caused by Echinococcus granulosus, • (ii) alveolar echinococcosis (alveolar hydatid disease) caused by Echinococcus multilocularis, and • (iii) polycystic echinococcosis caused by Echinococcus vogeli or Echinococcus oligarthus
- 7. Humans are an accidental, intermediate host and become infected when they accidentally ingest eggs of the tapeworm • The eggs hatch in the duodenum, and the released oncosphere penetrates the mucosa and reaches a blood vessel • most frequently settles in the liver and lungs • the parasite develops its larval stage, the hydatid cyst, the clinical presentation of E. granulosus • The cyst is a chronic, well-localized, and adapted space-occupying affliction that is not affected by the functional status of the host
- 10. Pathology • By 21 days becomes visible with with naked eye • Host tissue response- ecases parasite in fibous tissue • Parasite responds by forming inert chitinous material • 5 month- pericyst Avascular Spaces within contains BV, Bile ducts integral part of both the liver and the parasite Difficult to remove from liver
- 11. • Parasite can be separated by ectocyst • H. cyst – Unilocular – Increases size about 1 to 1.5mm/month – Fluid is under pressure – Liters of fluid Pathology
- 12. The fully developed wall of the cyst consists of two layers Ectocyst (laminated membrane) • is a cuticular chitinous structure without nuclei • never grows thicker than 5 mm, regardless of cyst size. Endocyst (germinative ) • microscopic dimensions • responsible for the production of the – crystal-clear hydatid fluid – ectocyst – brood capsules – scoleces – the daughter cysts Pathology
- 13. Pathology
- 14. • Daughter cyst formation is considered a defense reaction Endogenic vesiculation • Daughter cysts are true replicas of the mother cyst. • The presence of daughter cysts is a problem for chemotherapy, protoscolicide activity, and the standard PAIR procedure Ectogenic vesiculation of E. granulosus is infrequent. • It occurs when there is a small rupture or defect in the ectocyst and the endocyst passes through Pathology
- 15. • Hydatid fluid is antigenic • This antigenicity is rarely of great clinical significance • Allergic reactions range from skin rash to a frank anaphylactic reaction • The antigenicity of hydatid fluid is the basis of serodiagnostics Pathology
- 16. Clinical Presentation of Liver Hydatid Cysts • depend on the site, size, number, vitality, and stage of development of the cyst. • Simple, uncomplicated liver hydatid cysts usually asymptomatic or present with nonspecific symptoms • Complicated liver hydatid cysts cause specific symptoms and signs
- 18. Suppuration and Secondary Bacterial Infection • most frequent cause of infection is a cystobiliary communication • Clinically presents at pyogenic liver abscess • An infected hydatid cyst undergoes structural changes and the parasite dies • incidence in the literature ranges from 11.0% to 27.1
- 19. Pressure Effects • grow in the direction of the least resistance • Pressure effects appear sooner or later • symptoms result from direct pressure or distortion of neighboring structures or viscera. • An enlarging cyst – atrophy of surrounding hepatocytes – fibrosis – compensatory hypertrophy of the remaining liver parenchyma – replaces an entire liver lobe
- 20. • Serious consequence of cyst enlargement Rupture • Three types of cyst rupture have been addressed: – obscure – free – communicant rupture
- 21. Obscure (Internal) Rupture Injury or penetration of bile between pericyst and ectocyst Ruptue of ectocyst Protoscolesces occupies spaces Develops 100s of daughter cyst Unilocular multilocular
- 22. Such multilocular cyst when surgically opened No ectocyst Floating 100s of daughter cyst Within yellow fluid of gelatin like amorphous mass inside pericyst Obscure Rupture
- 24. Clinical significance of multivesicular cysts • host is exposed to hydatid antigens in the hydatid fluid • cyst is bacteriologically sterile • cyst contents cannot be easily aspirated and needs to be scooped out • the cyst must be treated as viable and infective • bile stained cyst contents mandates a meticulous search for CBC Obscure Rupture
- 25. Not all multivesicular cysts have bile-stained fluid, and not all cysts with bile-stained fluid have active communications with the bile ducts Obscure Rupture
- 26. hydatosis
- 27. Free Rupture In free rupture, the hydatid contents disseminates throughout the peritoneal or pleural cavity
- 28. Intraperitoneal Rupture • Hydatid cyst grows in the direction of the least resistance • superficial portion of the pericyst is stretched, thinned out • cyst irregularly shaped, fibrous whitish structure protruding from normal liver parenchyma • Cysts reaching the anterior and inferior part of the liver continue to grow, protruding into the abdominal cavity • high intracystic pressure causes rupture of both univesicular and multivesicular cysts
- 29. Clinical presentations of intraperitoneal rupture • (i) In acute symptomatic rupture, – peritoneal irritation and acute abdominal symptoms occur – The incidence is about 1% to 4%. • (ii) In anaphylactic shock – rupture precipitates severe circulatory collapse, which may be fatal mask the abdominal manifestations • (iii) In silent rupture, the patient presents with disseminated abdominal hydatidosis, unaware when the rupture occurred
- 30. (iv) Herniation of the laminated membrane occurs through the adventitial pericyst The herniating membrane does not actually burst and therefore no spillage of hydatid debris occurs The initial liver cyst remains small although the herniated, extrahepatic portion of the cyst can attain a volume of several liters – This condition mimics ascites, and attempts at percutaneous aspiration can lead to allergic manifestations Intraperitoneal Rupture
- 31. • Intraperitoneal rupture is a life-threatening complication that results in secondary echinococcosis • •Multiple cysts develop throughout the peritoneal cavity causing – intestinal obstruction, – gross abdominal distention, – ascites, – and cachexia several years after the rupture. • This is the secondary, smaller life cycle for the parasite, occurring only in the intermediate host. Intraperitoneal Rupture
- 32. Intrathoracic Rupture • Elevated hemidiaphragm and a sterile sympathetic pleural effusion can be the first signs of liver hydatid disease • Upward extension of a subdiaphragmatic cyst is usually asymptomatic, although it can cause dry cough, dyspnea, chest pain, and toxemia • The pleura and adherent basal lung segments often become inflamed and indurated • Frank intrapleural rupture with empyema (hydatopiothorax) is rare • pneumonitis or lung abscess
- 33. • The hydatid cyst may erode into a bronchiole and the contents can be evacuated • Rupture into bronchiole daughter cysts in the sputum • Ocassionally a bronchobiliary fistula will arise Expectoration of bile-tinged sputum • The incidence of diaphragmatic or transdiaphragmatic thoracic involvement by hydatid cysts in the dome of the liver ranges from 0.6% to 16% Intrathoracic Rupture
- 34. Communicant Rupture Hydatid cysts can rupture into physiologic channels (e.g., biliary, blood vessels) or adjacent organs (e.g., digestive tract)
- 36. • In silent rupture, bile leaks from eroded small ducts into the cyst, causing – endogenic vesiculation – suppuration – eventually death of the parasite • Such cysts are filled with bile-stained detritus, although no visible bile duct communications can be seen. • Probably 80% to 90% of hydatid cyst bile duct ruptures are of the silent type. Communicant Rupture
- 37. • A triad of symptoms characterizes rupture into the bile ducts: I. biliary colic II. partial intermittent or complete ductal obstruction with cholangitis and jaundice III. germinative membranes in the feces. Communicant Rupture
- 38. • The rapid discharge of the cyst contents into a major bile duct or body cavity can lead to the sudden absorption of the hydatid antigen in a sensitized patient, resulting in anaphylaxis. • More frequently, pruritus or urticarial rash is the major external manifestation. Episodes of asthma have been reported. Communicant Rupture
- 39. Organ Imaging in the Diagnosis and Treatment of Hydatid Disease •X-ray • Limited value • In endemic areas, elevation of the right hemidiaphragm in an otherwise healthy, asymptomatic patient is highly indicative of liver hydatidosis • Sometimes streaklike or round calcification of a senile hydatid cyst.
- 41. Ultrasound Imaging • readily available and easy to master • comparatively cheap, noninvasive, enables interventional procedures
- 42. • Pathognomonic US diagnostic features are I. unmistakable daughter cysts (rosettes•) within the main cyst cavity II. detachment of the membrane of the cyst (double-contoured membrane) III. agglomeration of daughter cysts in the dependent portion of a hydatid cyst IV. calcification of the cyst wall Ultrasound Imaging
- 43. • Based on US signs, Hassen Gharbi in 1981 classified liver hydatid cysts into five types I. pure fluid collection II. fluid collection with a split wall III. fluid collection with septa IV. heterogeneous appearance, and V. reflecting thick walls – Gharbi cyst types II and III as well as type V calcified cysts are characteristic for liver cystic hydatid disease. Ultrasound Imaging
- 45. Unilocular,no cyst wall Hydatid sand rossette Waterlily sign calcification Degenerative contents
- 46. 1/3rd sterile 2/3rd fertile ½ secndry cyst Wait and watch Further differential diagnosis Chemotherapy Surgery PAIR Chemotherapy Active cysts (type CL, CE 1, CE 2) No cyst wall Hydatid sand rossette Management options
- 47. living protoscoleces can exist and all treatment options should be considered Irregular wavy nature of fluid level produced by collapsed hydatid membrane floating on top of residual hydatid fluid Degenerating (transitional state) cysts (type CE 3)
- 48. further differential diagnosis is frequently Required Inactive cysts (type CE 4 and CE 5),
- 49. CT Scan • CT yields the most accurate information regarding the number, position, and cyst characteristics as well as the extent of intra- abdominal disease. • Discontinuity of the cyst wall in the vicinity of bile ducts is highly suggestive of CBC
- 50. ERCP • ERCP has little value in asymptomatic patients and should be avoided • Indications for endoscopic papillotomy in the preoperative period are 1. when US, CT, or ERCP detect hydatid material in the CBD 2. when cholangitis has been a feature of the clinical presentation, regardless whether a CBC is detected
- 51. indications for endoscopic papillotomy in the postoperative period are 1. hydatid material in the CBD 2. a biliary fistula lasting longer than 3 weeks 3. high-output biliary fistula (more than 1,000 mL per 24 hours) 4. Jaundice 5. short stricture obstructing the papilla Critical use of ERCP and papillotomy in patients with CBC has reduced mortality and in-hospital stay
- 52. References • Mastery of surgery • Sabiston text book of surgery • Schwartz text book of surgery
- 53. Next presentation on.. • Medical Management • Minimally Invasive techniques (PAIR) • Various Surgical Modalities of management
- 54. Thank you