Downloaded 31 times

















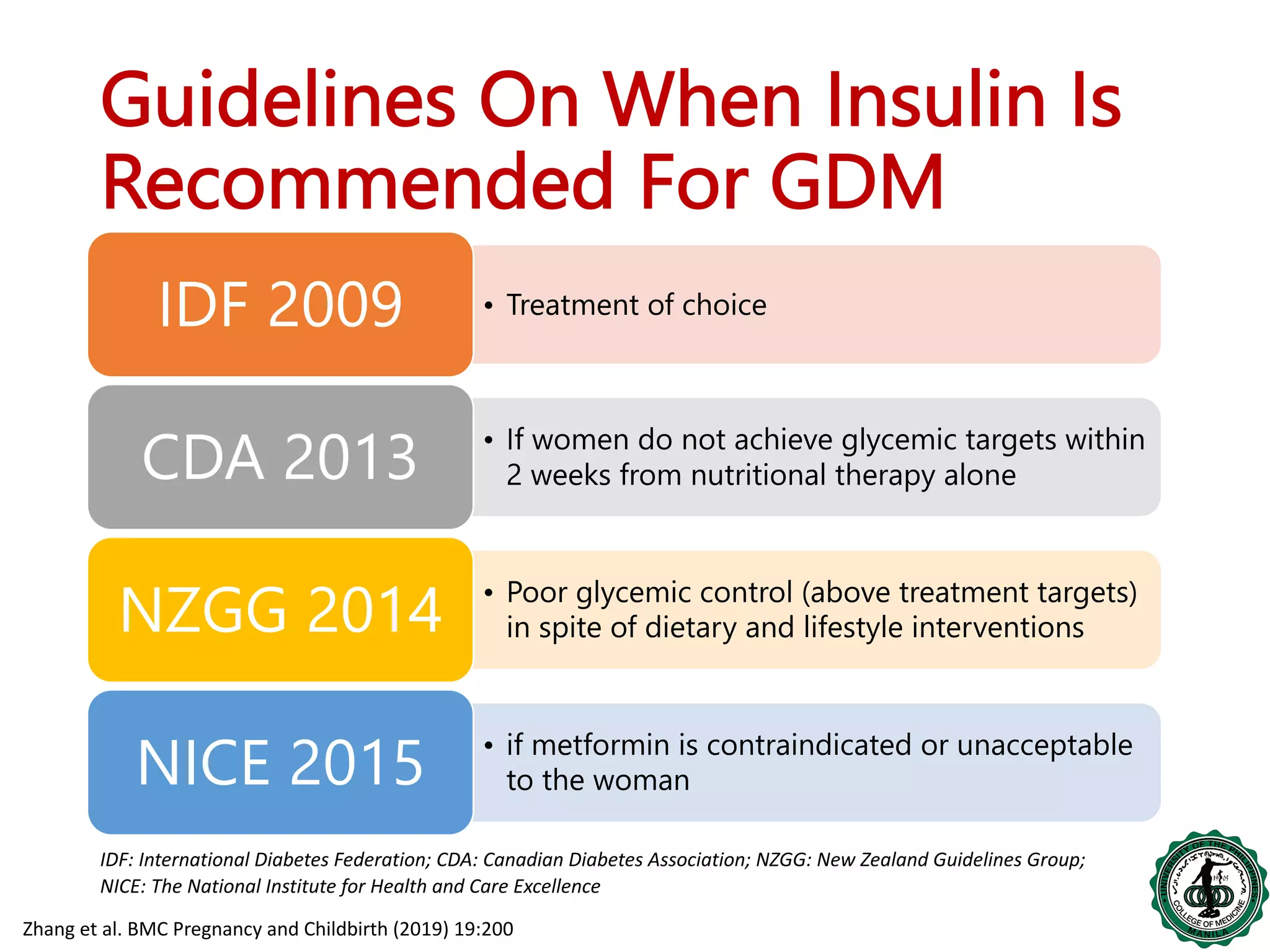













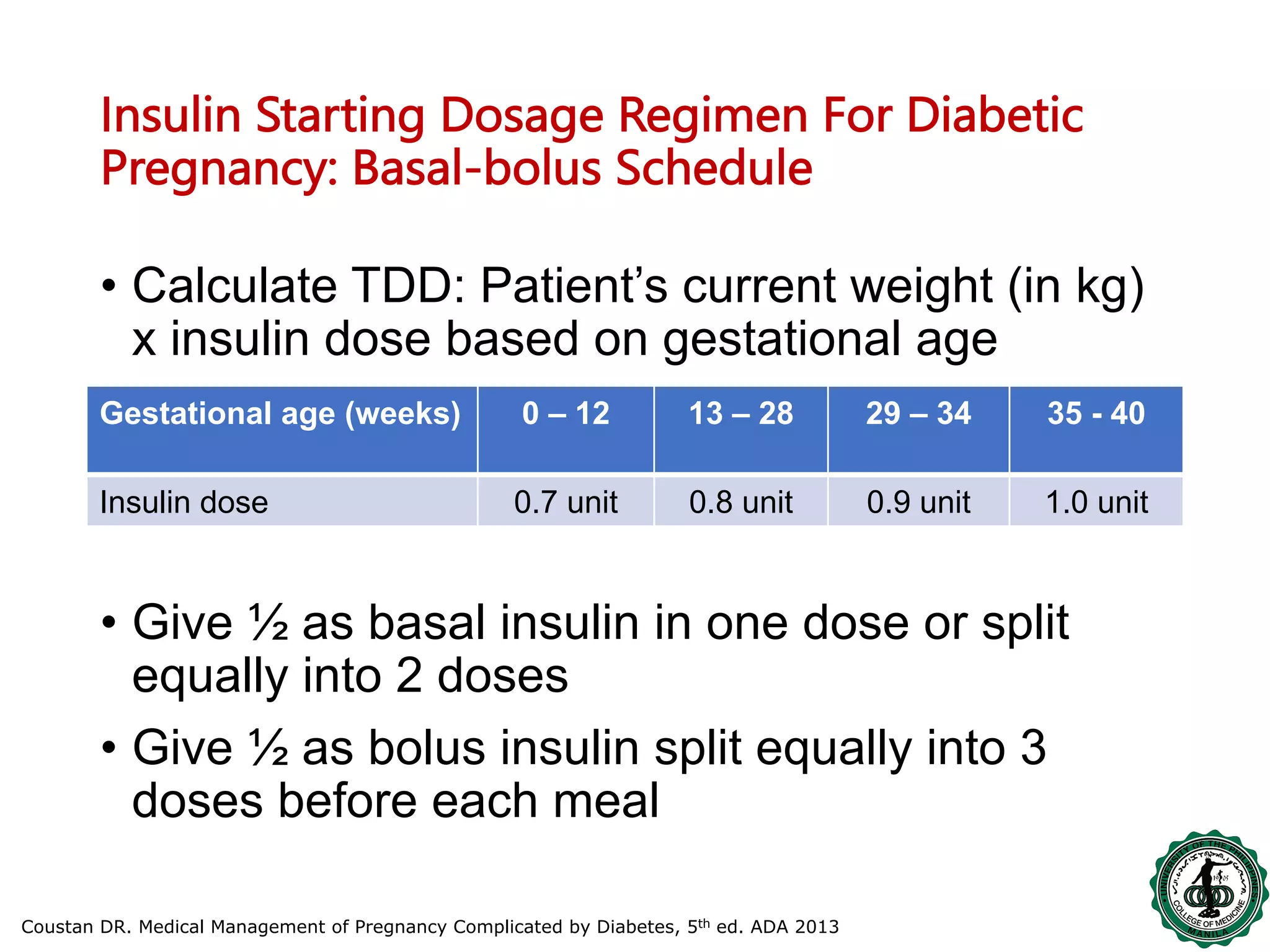




This document discusses the use of insulin in managing hyperglycemia during pregnancy. It begins by defining failure to manage blood glucose levels through medical nutrition therapy alone as an indication for insulin therapy. Guidelines recommend starting insulin if targets are not met within 2 weeks of nutrition management or if safety and growth parameters like weight gain are not being met. The document reviews types of insulin including human and analog varieties, providing evidence that various insulins can safely achieve targets when used as part of a basal-bolus regimen individualized to the patient's condition and blood glucose levels. The overall goal of insulin therapy in pregnancy is to maintain blood glucose within defined targets to support fetal and maternal health.












































































