Common medical emergencies and their management in Dental Practice
1. COMMON MEDICAL EMERGENCIES AND THEIR MANAGEMENT IN DENTAL PRACTICE
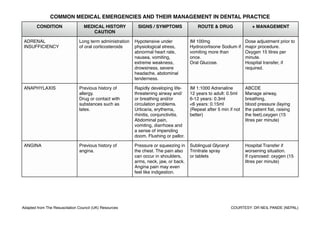
CONDITION MEDICAL HISTORY SIGNS / SYMPTOMS ROUTE & DRUG + MANAGEMENT
CAUTION
ADRENAL Long term administration Hypotensive under IM 100mg Dose adjustment prior to
INSUFFICIENCY of oral corticosteroids physiological stress, Hydrocortisone Sodium if major procedure.
abnormal heart rate, vomiting more than Oxygen 15 litres per
nausea, vomiting, once. minute.
extreme weakness, Oral Glucose. Hospital transfer, if
drowsiness, severe required.
headache, abdominal
tenderness.
ANAPHYLAXIS Previous history of Rapidly developing life- IM 1:1000 Adrenaline ABCDE
allergy. threatening airway and/ 12 years to adult: 0.5ml Manage airway,
Drug or contact with or breathing and/or 6-12 years: 0.3ml breathing,
substances such as circulation problems. <6 years: 0.15ml blood pressure (laying
latex. Urticaria, erythema, (Repeat after 5 min if not the patient flat, raising
rhinitis, conjunctivitis. better) the feet),oxygen (15
Abdominal pain, litres per minute)
vomiting, diarrhoea and
a sense of impending
doom. Flushing or pallor.
ANGINA Previous history of Pressure or squeezing in Sublingual Glyceryl Hospital Transfer if
angina. the chest. The pain also Trinitrate spray worsening situation.
can occur in shoulders, or tablets If cyanosed: oxygen (15
arms, neck, jaw, or back. litres per minute)
Angina pain may even
feel like indigestion.
Adapted from The Resuscitation Council (UK) Resources COURTESY: DR NEIL PANDE (NEPAL)
2. COMMON MEDICAL EMERGENCIES AND THEIR MANAGEMENT IN DENTAL PRACTICE
CONDITION MEDICAL HISTORY SIGNS / SYMPTOMS ROUTE & DRUG + MANAGEMENT
CAUTION
ASTHMA Known Asthmatics, Acute severe asthma: Salbutamol Inhaler Oxygen (15 litres per
under oral and Inability to complete 100microgram per minute)
inhalational therapy / sentences in one breath. actuation upto 10 Hospital Transfer, if
nebuliser / steroid / Respiratory rate > 25 per actuation with a spacer, required.
hospitalisation minute. every 10 mins. if
Tachycardia (heart rate > required.
110 per minute).
Life threatening Bronchospasm / Life
asthma: threatening signs:
Cyanosis or respiratory IM 1:1000 Adrenaline
rate < 8 per minute. 12 years to adult: 0.5ml
Bradycardia (heart rate < 6-12 years: 0.3ml
50 per minute). <6 years: 0.15ml
Exhaustion, confusion, (Repeat after 5 min if not
decreased conscious better)
level.
CARDIAC ARREST Heart condition Absence of pulse, AED ABCDE
breathing.
CHOKING & Iatrogenic Cough and splutter. Symptomatic treatment If any large pieces of
ASPIRATION Loose prosthesis. Difficulty breathing. of wheeze with a foreign material have
Local anaesthesia may Breathing may become salbutamol inhaler. been aspirated, chest x-
diminish the normal noisy with wheeze Follow algorithm. ray may be warranted.
protective pharyngeal (usually aspiration) or
reflexes. stridor (usually upper
airway obstruction).
‘Paradoxical’ chest or
abdominal movements.
Cyanosis and loss of
consciousness
Adapted from The Resuscitation Council (UK) Resources COURTESY: DR NEIL PANDE (NEPAL)
3. COMMON MEDICAL EMERGENCIES AND THEIR MANAGEMENT IN DENTAL PRACTICE
CONDITION MEDICAL HISTORY SIGNS / SYMPTOMS ROUTE & DRUG + MANAGEMENT
CAUTION
EPILEPTIC SEIZURE Epileptic with recent Aura If blood glucose <3.0 Must continue their
change in medication/ Sudden loss of mmol per litre:oral/buccal normal dosage of
precipitating factor and consciousness, rigid, glucose, or glucagon anticonvulsant drugs
time of last attack to be falls, may give a 1mg IM. before attending for
noted cry, and becomes Convulsive movements dental treatment.
cyanosed (tonic phase) lasting 5 minutes or Check glucose level.
followed by jerking longer) or recur in quick During a seizure try to
movements of the limbs; succession: Midazolam ensure that the patient is
the tongue may be bitten not at risk from injury but
(clonic phase). Frothing, make no
urinary incontinence. attempt to put anything
Floppy, unconscious. in the mouth or between
Conscious, confused. the teeth. Oxygen (15
Decreased BP, Pulse. litres per minute)
HYPERVENTILATION Severe Anxiety and Light headedness or Reassurance
Breathing faintness, spasm of
muscles around the
face and of the hands
Adapted from The Resuscitation Council (UK) Resources COURTESY: DR NEIL PANDE (NEPAL)
4. COMMON MEDICAL EMERGENCIES AND THEIR MANAGEMENT IN DENTAL PRACTICE
CONDITION MEDICAL HISTORY SIGNS / SYMPTOMS ROUTE & DRUG + MANAGEMENT
CAUTION
HYPOGLYCEMIA Insulin treated diabetics Shaking and trembling. Early stages - where the ABCDE if no sign of life.
more prone / Poorly Sweating. patient is co-operative
controlled less aware Headache. and conscious with an
diabetics!!! Difficulty in intact gag reflex, give
concentration / oral glucose (sugar
vagueness. (sucrose), milk with
Slurring of speech. added sugar, glucose
Aggression and tablets or gel). (may be
confusion. repeated in 10 -15 mins)
Fitting / seizures. In more severe cases -
Unconsciousness. where the patient has
Blood glucose <3.0mmol impaired consciousness,
per litre . is uncooperative or is
unable to swallow safely
buccal glucose gel and /
or IM Glucagon (1mg in
adults and children >8
years old or >25 kg,
0.5mg if <8 years old or
<25 kg)
MILD ALLERGY Previous history of Urticaria, Oral Chlorphenaramine Monitor
allergy. Maleate
Drug or contact with
substances such as
latex.
Adapted from The Resuscitation Council (UK) Resources COURTESY: DR NEIL PANDE (NEPAL)
5. COMMON MEDICAL EMERGENCIES AND THEIR MANAGEMENT IN DENTAL PRACTICE
CONDITION MEDICAL HISTORY SIGNS / SYMPTOMS ROUTE & DRUG + MANAGEMENT
CAUTION
MYOCARDIAL Cardiac Conditions Progressive onset Give sublingual Call Ambulance
INFARCTION severe, crushing pain in Nitroglycerine. immediately. Allow the
the centre and across 300mg Aspirin orally. patient to rest in his most
the front of chest. May comfortable position.
radiate to the shoulders Oxygen 15 litres/min.
and down the arms Assess.
(more commonly the If becomes unresponsive
left), into the neck and ABCDE.
jaw or through to the
back.
Pale, clammy skin
Nausea/vomiting
Weak pulse, low bp
Shortness of breath.
POSTURAL Rising abruptly or of Dizziness Lay the patient flat as When rising, patients
HYPOTENSION standing upright for too Going towards syncope. soon as possible and should take their time.
long raise the legs to improve
ACE inhibitors to control venous
BP return.
Loosen any tight
clothing.
Adapted from The Resuscitation Council (UK) Resources COURTESY: DR NEIL PANDE (NEPAL)
6. COMMON MEDICAL EMERGENCIES AND THEIR MANAGEMENT IN DENTAL PRACTICE
CONDITION MEDICAL HISTORY SIGNS / SYMPTOMS ROUTE & DRUG + MANAGEMENT
CAUTION
STROKE Hypertension Sudden numbness, Hospital Transfer
Heart Disease tingling, weakness, or
High Cholesterol loss of movement in your
Tobacco user face, arm, or leg,
Diabetes especially on only one
Overweight/obesity side of your body, vision
Family History changes, trouble
speaking.
Sudden confusion or
trouble understanding
simple statements,
problems with walking or
balance, severe
headache that is
different from past
headaches.
SYNCOPE Repeated Faints Faint / dizzy / light Lay the patient flat as Oxygen (15 litres per
headed. soon as possible and minute)
Slow pulse rate. raise the legs to improve
Low blood pressure. venous
Pallor and sweating. return.
Nausea and vomiting. Loosen any tight
Loss of consciousness. clothing.
Adapted from The Resuscitation Council (UK) Resources COURTESY: DR NEIL PANDE (NEPAL)