
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Chronic lower limb ischemia
Similar to Chronic lower limb ischemia (20)
Recently uploaded
Recently uploaded (20)
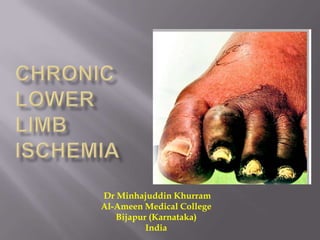
Chronic lower limb ischemia
- 1. Dr Minhajuddin Khurram Al-Ameen Medical College Bijapur (Karnataka) India
- 2. Peripheral areterial occlusive disease (PAOD/PAD/PVD) refers to the obstruction or detoriation of ateries other than those supplying the heart and within the brain
- 3. Impairment of circulation Incidence increases with age 0.3%/yr (40 to 55yrs) to 1%/yr (after 75yrs) Quality of life/cost of treatment Non whites> whites Male gender Obesity
- 4. Black (hispanic) Increasing age Smoking Hypertension Dyslipidemia Hypercoaguble states Renal insufficiency DM Younger>aged
- 5. Family history of vascular disease or stroke/ heart attack In study C-reactive protein Homocysteine
- 7. Intima Internal elastic membrane Media Composed of smooth m/s, collagen, elastin and preteoglycans Blood suply: Internal half: Direct diffusion External half: vasa vasorum External elastic membrane Adventitia • Fibroblasts and collagen
- 9. Acute Sudden occlusion of an artery No time for collateral openings Poikilothermia, Pain, Pulseless, Pallor, Parasthesia and Paralysis Chronic No sudden obstruction Gradual narrowing of lumen Enough time for collaterals to develop More tolerant to prolonged ischemia
- 10. Atherosclerosis {lower limb} TAO (Buerger’s Disease) {lower limb} Infective Vasculitis syndromes
- 12. Atherosclerosis = Athero + sclerois Plaque composed of smooth m/s, lipids, connective tissue and macrophages
- 13. Brief pathophysiology Lipid deposition calcification erosive areas and ulceration prothrombotic cell activity plaque lipid core becomes necrotic covered by FIBROUS CAP rupture, perceived as injury laying down of platelets and formation of a clot.
- 15. Ischemia may be due to Narrowing of the lumen Rupture leading to fibrous cap Embolization
- 16. More shearing stress/ increased turbulence Infra renal aorta Iliac bifurcation Carotid bifircation Superficaial femoral arteries Ostia or renal, coronary and mesenteric arteries.
- 17. Inflammatory reaction of the arterial wall with involvement of neighboring vein and nerves 2nd to 4th decade of life; male>females Specifically linked to smoking Low socio-economic groups Recently, familial disposition and autoimmune mechanism has also been postulated
- 19. Pathology smoking (nicotine) Increased % carboxy hb vasospasm damage to the vessel wall TAO fibrosis
- 20. Involves medium and small sized vessels; those distal to the popliteal artery Very rare upper limb involvement Acute Lesion: Arteritis, periarteritis, acute phlebitis (migratory in 30%) and periphlebitis. Invasion of wall by polymorphs and giant cells. Thrombus, with microabscesses
- 21. Chronic Lesion Arteries and veins bound together by fibrosis Nerve involvement Fibroblastic activity and endothelial proliferation in the thrombus Thrombus organized as fibrous tissue
- 22. Pain (Intermittent claudication) “Claudio”= I limp Cramp like pain Brought on by exercise Not present on walking the first step Relieved by standing still Slight variation each day Due to accumulation of substance P Site of Claudication: Group of muscles distal to the site of obstruction
- 23. Pain (Intermittent claudication) Clinical Classification a) Boyd’s Classification Grade Pain I Pain relieved on continued walking II Walks in pain III Compelled to take rest IV Pain at rest
- 24. Claudication distance : distance at which the pain first appears
- 27. Pain (Intermittent claudication) Occlusion and site of claudication Site of Occlusion Claudication site/ other symptoms Aorto-iliac obstruction • Claudication in in both buttocks, thighs and calf • Absent femoral, popliteal and DP pulses • Impotence (Leriche’s syndrome) Iliac obstruction • Unilateral claudication in thigh and calf • Unilateral absence of femoral and distal pulses Femoropopliteal obstruction • Unilateral claudication in the calf • Absent distal pulses Distal obstruction • Ankle pulses absent • Claudication in calf and foot
- 28. Pain (Intermittent claudication) Rest pain Grade IV Boyd’s classification Felt in the foot (most distal parts) Due to ischemia of the somatic nerves (cry of the dying nerves) Exacerbate on lying down or elevation of foot Worse at night; patient sits in “hen-holding” position Pressure of even bed clothes worsens the pain Lessened by hanging the foot down or sleeping on a chair Patient may commit suicide
- 29. Pain (Intermittent claudication) Rest pain – “Hen-holding”
- 30. Pain (Intermittent claudication) Critical limb ischemia Persistently recurring ischemic rest pain requiring regular, adequate analgesia for more than 2 weeks or ulceration or gangrene of foot or toes with ankle pressure <50mmHg or toe pressure <30mmHg
- 31. Pain (Intermittent claudication) Differential Diagnosis 1. Nerve root compression (eg: herniated disc) Sharp lacinating pain Sudden onset on walking History of back problems 2. Spinal stenosis History of back problems Motor weakness more prominent Onset by standing also Relived by change in position
- 32. Pain (Intermittent claudication) Differential Diagnosis 3. Arthritic/ inflammatory Aching pain Variable pain Not relieved as quickly 4. Baker’s cyst Swelling, tenderness Rest pain Subsides slowly Not intermittent
- 33. Pain (Intermittent claudication) Differential Diagnosis 5. Venous claudication Bursting type of pain Relief speeded by elevation h/o DVT Signs of venous congestion 6. Chronic compartment syndrome Bursting pain Heavily muscled legs Relief speeded by elevation
- 34. Other symptoms Ulceration Gangrene Loss of senstion Loss of movements
- 35. History Can identify the location and severity of the disease Pain: Location Precipitating and aggravating factors Frequency, duration and evolution Rule out other causes of pain in the lower limbs Patients with co- morbid conditions who cannot walk present late with gangrene and rest pain Drug/Medical history Surgical history Family history : first degree with abdominal aortic aneurysm
- 36. History Vascular review of symptoms TIA Difficulty in speech or swallowing Dizziness/ drop attacks Blurry vision Arm fatigue Pain in abdomen after eating Renal insufficiency (poorly controlled hypertension) Impotence Claudication Rest pain or tissue loss
- 37. Physical examination Inspection Change in colour Signs of ischemia Bueger’s test Capillary filling test Venous refilling Pregangrenous/ gangrenous part examination
- 38. Physical examination Palpation Skin temperature Venous refilling Perpheral pulses Disapperaing pulse Joint movements / muscle strength Sensations Auscultation: Bruits
- 39. Physical examination Dry vs Wet Gangrene Dry gangrene Wet gangrene Dry, shriveled, mummified Odematous, putrified and discoloured Occurs due to slow and gradual loss of blood supply Occurs due to sudden loss of blood supply Clear line of demarcation is present Vague/ No line of demarcation No proximal extention Proximal extension Limited amputation High amputation
- 40. Physical examination Dry vs Wet Gangrene
- 41. ABPI
- 42. ABPI Physiological testing SBP of PT/PT/PA (higher) --------------------------------- = ABPI Higher of the two brachial SBPs Normal value =>1 Claudication <0.9 Rest pain <0.5 Imminent necrosis <0.3 Note: Normal value doesn’t rule out ischemia Retest after exercise, ABPI may fall Wrong high readings in calcified arteries, e.g. seen in diabetics &ESRD
- 43. ABPI Note: Normal value doesn’t rule out ischemia Retest after exercise, ABPI may fall Post exercise ABPI considered POSITIVE when ABPI fall => 0.2 and/or Failure to return to baseline in 3 minutes Wrong high readings in calcified arteries, e.g. seen in diabetics &ESRD
- 44. Segmental pressure Difference of 20-30 mmHg is indicative of significant lesion
- 45. Photo-Plethysmography Investigation for segmental flow Infra-red light emitting source + a photosensor Light decreases when flow increases Generates a pressure and waveform of different arteries A difference of 20-30 mmHg is significant.
- 46. Doppler Ultrasound (DU) Continous wave DU with segmental waveforms Doppler shift converted to audio signal Normal Triphasic Signal Sharp systolic upstroke Reversal of flow in early diastole Low amplitude forward flow throughout diastole.
- 47. Doppler Ultrasound (DU) Obstructive disease Initial Loss of reversal flow in early diastole (Bi-phasic) Severe blunting of arterial waveform with decreased amplitude Worsening only diastolic flow (Mono-phasic ) In case of a proximal obstruction/ stenosis Assessment downstream is less accurate Shows moving blood but it may/ may not be sufficient
- 49. Duplex Ultrasound Provides with B mode settings (gray settings) Pulsed Doppler spectral waveforms Can even detect very low flow states Color flow data and waveforms for analysis by a computer. Shows blood flow and turbulence Peak systolic velocities (PSV) and End diastolic velocities are recorded.
- 50. Duplex Ultrasound Change in waveforms Triphasic biphasic Monophasic Ratio of PSV proximal and distal to occlusion >2.0 indicates a stenosis of 50% or more Difficult in aoto-illiac segments, especially in obese individuals (patient should fast overnight)
- 51. Angiography Invasive techique of visualising the arterial tree Hypaque 45 (Sodium Diatrazoate) is used as a dye (75 to 100 ml) Course of arteries, constrictions, and distal “Run off” To plan interventions 1. Transfemoral 2. Trans-lumbar (established bi-lateral obstruction) Seldinger technique is used
- 52. Angiography Done in 4 stages i. Dye released at the level of diaphragm in the aorta Abdominal aorta Celiac artery Sup mesenteric artery Inferior mesenteric artery ii. Dye released at aortic bifurcation B/L common iliac arteries Hypogastric arteries External iiliac arteries Common femoral arteries Sup Femoral arteries Profunda femoris
- 53. Angiography Done in 4 stages iii. Contralateral common femoral artery Contralateral Sup Femoral artery Profunda femoris Popliteal artery 3 crural arteries Pedal arteries iv. Ipsilateral common Femoral artery Sup Femoral artery Profunda femoris Popliteal artery 3 crural arteries Pedal arteries
- 54. Angiography Site of block in Atherosclerosis
- 55. Angiography Cork-screw pattern of vessels in TAO Block at multiple sites in small and medium sized arteries
- 56. Angiography Risk / Complications: a) Groin hematoma b) Retroperitoneal bleeding c) Pseudo-anuerysm d) Arterial dissection e) Contrast nephropathy f) Contrast allergy
- 57. CT angiography IV contrast followed by Ct imaging Thin slices of 0.625mm Allows 3-D reconstruction Improved speed Lesser contrast material Appreciation of thrombus, calcification, etc. better Disadvantages similar to angiography
- 58. Digital subtraction angiography (DSA) Angiographic images being digitilised by a computer With substraction of extrenous background (bone, soft tissues)
- 59. MR angiography Uses Godalinium as contrast Better sensitivity and specificity Disadvantages: longer study duration Costlier Metallic implants contra-indication Nephrotoxic contrast Fibrosed nodules of skin, eyes and joints (rare complication)
- 60. Carbon Dioxide angiography CO2 as contrast agent In cases of renal insuffieciency CO2 temporarily displaces blood but dissolves in 3-5 minutes Poor detail Significant patient discomfort Gas trapping mesenteric ischemia
- 61. General Investigations ECG ECHO Lipid profile COPD Blood tests to exclude Anemia DM Deranged RFT High blood viscosity (polycythemia and thrombocythemia)
- 62. Intravascular ultrasound (IVUS) Catheter based intravascular ultrasound Provides transverse and 360 degree image of the lumen of the vessel Qualitative data about the wall anatomy
- 63. Brown’s vasomotor index For Buerger’s disease Test of vasospasm Block the nerves with Local anesthesia to predict efficacy of Sympathectomy Rise in skin temperature is recorded Index = Rise in skin temperature – Rise of mouth temperature Rise of mouth temperature Index =>3.5 is positive for sympethectomy
- 64. Conservative management Indications: Ankle pressure >60mmHg Femoral pulse + No rest pain No tissue loss Controlled infection (eg diabetic patient) Unfit for surgery ABPI >0.5 (Relative indication)
- 65. Conservative management Stop smoking Keep walking Reduce weight (obese individuals) Exercise Diabestes and hypertension Care of feet Buerger’s position Buerger’s exercise
- 66. Conservative management Drugs Analgesics- Aspirin Vasodialtors Cilostazol (phosphodiasterase inhibitors) Pentoxyphylline (phosphodiasterase inhibitors) Prostacycline Platelet aggregation inhibitors Clopidrogel Aspirin Prostacycline
- 67. Conservative management Drugs To Control Diabetes Hypertension Dyslipidemia Atherosclerosis Infection Note: Risk of limb Loss to be explained to the patient (Failure in 25% of patients) Opening up of collaterals or change of gait with less usage of the affected muscle
- 68. Indirect surgeries Sympathectomy Chemical Surgical Indications: Rest pain Skin ulcerations TAO Elderly patient (senile gangrene)
- 69. Indirect surgeries Sympathectomy Chemical Produces cutaneous vasodilatation Injection in front of the lumbar fascia which contains sympathetic trunk; Under C-Arm 5ml phenol in water is inected in front of 2nd, 3rd and 4th lumbar vertebra
- 70. Indirect surgeries Sympathectomy Surgical (pre-ganglionic sympathectomy) Abdomen opened with oblique incision under genral anasthesia Dissection through flat abdominal muscles, and peritoneum The sympathic chain is situated medial to the medial margin of psoas muscle Rt side overlapped by IVC Lt side overlapped by aorta Sympathetic chain identified by the presence of ganglia First lumbar ganglia is as high as crus of the diaphragm
- 71. Indirect surgeries Sympathectomy Surgical Sympathectomy from 1 to 4th lumbar ganglion Closed the site in layers Note: in case of bilateral surgery; preserve L1 of atleast one side causes retrograde ejaculation.
- 73. Surgical Management Surgical Revascularization Procedures Open Endo-vascular Amputation
- 74. Surgical Revascularization Procedures Open vs endo-vascular Trans-Atlantic Inter Society Documentation Management of Peripheral Arterial Disease (TASC) 2000 TASC –II in 2007 “Endovascular therapy is the treatment of choice for Type A lesions and surgery is the treatment of choice for Type D lesions. Endovascular treatment is the preferred treatment for Type B lesions and surgery is the preferred treatment for good risk patients with Type C lesions”
- 75. TASC –II (Aorto-iliac)
- 76. TASC –II (Aorto-iliac)
- 77. TASC –II (Aorto-iliac)
- 78. TASC –II (Aorto-iliac)
- 79. TASC –II (Femoro-popliteal)
- 80. TASC –II (Femoro-popliteal)
- 81. TASC –II (Femoro-popliteal)
- 82. TASC –II (Femoro-popliteal)
- 83. Open Surgical Management (Aorto-iliac disease) Aorto-bifemoral bypass with a prosthetic graft via transabdominal or retroperitoneal approach. End to end or end to side proximal anastomosis Nervi erigentes should be taken care of (damage will lead to retrograde ejaculation) in the area of CIA Mortality 5%
- 84. Open Surgical Management Choice of Graft (Conduits) Great Sephanous vein Preferred for lower limbs with better patency rates (90% First yr and 60% five yrs) Should preferentially be used in all below knee by-passes Can be used in situ Better size match Removal of valves with valvulotome Reversed No need of disruption of valves May be harvested endoscopically No added advantage of one over the other
- 85. Open Surgical Management Choice of Graft (Conduits) PTFE (Polytetrafluoroethylene) Can be used as a replacement of LSV Poorer results compared to LSV (50% in five yrs) New: with heparin coating Dacron is a brand name of PTFE
- 86. Open Surgical Management Choice of Graft (Conduits) Small sephanous vein Basillic vein Cephalic vein All these three veins have very thin walls, hence no good results veins when joined to increase the length gives poor results Cryo-preserved arteries Cadevaeric arteries preserved in cold Bovine pericardial patches
- 87. Open Surgical Management (Aorto-iliac disease) Aorto-bifemoral bypass Midline or transverse abdominal incision CFA and branches exposed through groin incision Small bowel retracted to right Posterior peritoneum is open Retroperitoneal tunnels are made to groin. Heparin 5000U given iv bolus and vessels clamped
- 88. Open Surgical Management (Aorto-iliac disease) Aorto-bifemoral bypass Vertical incision on anterior aspect of Aorta Dacron sutured end to side (taking all the layers) The Limbs fed to the groin sutured end to side to CFA Posterior peritoneum closed over peritoneum
- 90. Open Surgical Management (femoro-popliteal) Open groin surgery CFA endarectomy + profundoplasty/ iliofemoral bypass In case of added proximal (iliac) occlusion CFA endarectomy + profundoplasty / iliofemoral bypass + iliac stenting In case of added distal (SFA)occlusion CFA endarectomy + profundoplasty +SFA stenting/ femoropopliteal bypass
- 91. Open Surgical Management Endarterectomy Open: When it involves short segment of big arteries Also called “dis-obliteration/ reboring” Heparin 5000U given pre-opeartively Artery is exposed after placing clamps Distal clamp applied first Longitudinal incision taken oven the occlusion till the plaque is reached
- 92. Open Surgical Management Endarterectomy Open: Plane created between plaque and media The plaque is removed with the diseased intima In case of thrombus, it is removed Closed with non absorbable fine sutures directly or a vein graft Post op anticoagulant therapy with warfarin
- 93. Open Surgical Management Endarterectomy Closed Artery exposed and clamped Proximal and distal transverse incisions taken Plane created between plaque and tunica media Wire loop passed from distal to lower arteriotomy insion, stripping the plaque Can be used in relatively longer occlusions
- 94. Open Surgical Management Endarterectomy Balloon Artery is exposed after clamping Proximal arteriotomy is made Fogarty ballon catheter is passed
- 95. Open Surgical Management Endarterectomy Passed beyond the obstruction Ballon is inflated Pulling the catheter removes the atheroma More commonly used for emboli (as they are comparetively loosely adherant)
- 96. Open Surgical Management Profundoplasty Repairing of profunda femoris Arises posterior to CFA The vessel is dissected out and clamps are applied Arteriotomy extending from CFA to distal to occlusion Atherectomy is then performed
- 97. Open Surgical Management Profundoplasty Defect is them closed by a vein patch On table angiography is then performed to check for patency May be done in adjunct to bypass surgeries
- 98. Open Surgical Management Femoro-popliteal bypass In patients with SFA and popliteal artery occlusion with a distal segment of patent popliteal artery. In continuity with any crural artery Longitudinal groin incision to access the CFA Popliteal artery is exposed medially from thigh or the leg In above knee bypass, incision proximal to the knee to access popliteal artery In below knee bypass, popliteal fossa is opened
- 99. Femoro-popliteal bypass Polpileat vein is held in Silastic loops Graft is tunnelled and placed at the anastomotic site Sephanous vein graft can be used In situ (requires desruption of valves) Reversed, can be accessed by a parallel skin incision
- 100. Open Surgical Management Infrapopliteal bypass Disease involving popliteal artery and proximal tibial arteries. the target artery must have luminal continuity with the foot Stenosis upto 50% is accepted as patent for surgery Calcification also not considered a contra-indiaction. SFA or Popliteal artery is used for “inflow”
- 101. Open Surgical Management Infrapopliteal bypass Access to PTA with dissection and separation of Soleal muscle attachment from tibea access to PTA and PA Access to ATA with anterolateral incision on legseparation of ant tibial muscle and external longus muscle ATA. Separation of interosseus membrane for tunneling of the graft. Small veins can be used for anastomosis Or PTFE graft can be used
- 102. Open Surgical Management Other bypasses A. Axillofemoral graft Tunnelled subcutaneously between the axillary artery proximally, to reachone or both CFA Low patency rates B. Femoro-femoral crossover bypass Crossover graft by tunnelling a prosthetic graft subcutaneously above the pubis between the groins
- 104. Endovascular management Basically involves gaining access into transmural space via percutaneous femoral artery puncture Balloon angioplasty Subintimal angioplasty Stenting Stent graft Variations of balloon angioplasty
- 105. Endovascular management Balloon angioplasty Guide wire is negotiated through the stenosis or occlusion Then a balloon is inflated to open the occlusion It is kept inflated for approx 1 minutes with high pressure then deflated May be combined with stenting
- 106. Endovascular management Balloon angioplasty Very good results for dilating the iliac and femporopopliteal segments Below knee procedures are less successful 98% success in CLI (extremely good results) Limb salvage rate of 91% over 5 fyrs Failure in TASC D patients
- 107. Endovascular management Subintimal angioplasty Creating an arterial dissection purposely begenning at the proximal end of the oclusion The guide wire is made to re-enter the lumen at the diastal end of occlusion Use of balloon angioplasty to increase the diameter of the false lumen Poor results 3 yrs patency rates being only 30% But good for critical limb ischemia
- 108. Endovascular management Subintimal angioplasty
- 109. Endovascular management Stenting If the vessel fail to remain dilated use stents Stainless steel stents May be introduced on a balloon catheter and placed in position Self expanding stents (nitinol), which expand on withdrawing the sheath Angioplasty (balloon) + stenting > primary stenting But primary stenting > only angioplasty Poor results in TASC D patients
- 110. Endovascular management Stenting
- 111. Endovascular management Stenting
- 112. Endovascular management Stent garft Expanded PTFE (ePTFE) with external nitinol stent Inner surface bonded with heparin Extremely flexible Can close conform to the shape of artery (esp: SFA) Self expanding stents Easier with better patency rates than atherectomy. It is easier, with more better technical succes comapred t o PTA Few studies show similar results comapred to bypass
- 113. Endovascular management Cutting balloon Originally designed for coronary arteries The balloon has three or four atherotomes or micro-surgical blades These are mounted longitudinally on the balloon The blades score the lesion and dilate the lesions
- 114. Endovascular management Cryoplasty Apoptosis by cooling Designed by Polar Cath Peripheral Dilatation System (Boston Scientific) Balloon filled with nitrous oxide gas To cool to -10 degrees C Supposed to prevent restenosis
- 115. Endovascular management Endovascular atherectomy Excision atherectomy catheters remove and collect the atheroma Ablative atherectomy device fragment it Rotational cutters turn at the speed of 8000rpm to shave the plaque and collect in a storage chamber Laser atherectomy has a cold tipped laser that delivers burst of ultraviolet Xenon energy in short pulse durations Results same as balloon angioplasty
- 116. Endovascular management Endovascular atherectomy Rotational cutter Laser tipped
- 117. Amputation Indication for amputation Dead Limb Gangrene Deadly Limb Wet gangrene Spreading cellulitis Dead Loss Limb Severe rest pain with Ischemia Paralysis Contracture
- 118. Amputation Choice of amputation Below knee amp[utation (BKA) Above knee amputation (AKA Ray amputation Transmetatarsal amputation Miscellaneous Syme’s Chopart’s Lisfranc’s
- 119. Amputation Level of amputation Skin perfusion pressure >=40 mmhg Transcuatneous oxygen pressure >= 30mmhg Predictors for Transmetatarsal amputation: Toe Blood Pressure >=30 mmhg Ankle Blood Pressure >= 80 mmHg
- 120. Amputation Below Knee Amputation Above Knee Amputation Poor Healing Better Healing More chances of revision/ healing by secondary intention Less chances of revision Better ambualtion Poor ambulation
- 121. Amputation Ray amputation
- 122. Amputation A. Syme’s B. Chopart’s C. Lisfranc’s D. Transmetatarsal
Editor's Notes
- Resulting into ischemiaMay be due to co-morbid conditions and poverty
- DESCRIBE EACHIntima, single layer of cells, longitudinal axis, in contact with bloodMedia: strengthProteoglycans: disachharide bound to proteins, act as cement
- I- limbs are viable and not immediately threatenedIIa – limbs are viable but salvagable if treatedIIb – limbs are salvagable if treated ungentlyIII- not salvagable
- Infective eg: syphilis
- Cap composed of smooth musclesandconnective tissuesIn this way an insignificant narrowing can result in major obstruction
- Occlusion one level above the site of claudication
- Evolution is important.. Decrease in claudication distance , finally rest painMedical history: prior stroke, diabetes, hypertension, dyslipidemia, tobocco abuseDrug history: anti platelet agents, beta blockers, statins, heparin, protamineSurgical history: previous surgeries, coronary artery bypass grafting, previous sephanous vein harvesting
- Theory Das
- Theory Das
- Theory Das
- Theory Das
- BP cuff and continous wave doppler
- BP cuff and continous wave doppler<0.9 …6 folds of cardiovascular morbity
- BP cuff and continous wave doppler<0.9 …6 folds of cardiovascular morbity
- A continous wave ultrasound is transmitted by the probe which is reflected by moving RBCsand picked up by the receiver within the probe and converted to audio signalsChange in frequency of the reflected beam gives Doppler shift
- A continous wave ultrasound is transmitted by the probe which is reflected by moving RBCsand picked up by the receiver within the probe and converted to audio signalsChange in frequency of the reflected beam gives Doppler shift
- Previously under LA , now under USG guidance
- Nephropathy:Increase hydration
- DSA with PA view
- High blood viscosity (polycythemia and thrombocythemia) smoking, malignancy, renal dysfunction,
- From erecter spinae to medial border of rectus
- From erecter spinae to medial border of rectus
- From erecter spinae to medial border of rectus
- End to end : better flow dynamicsEnd to side : the blood supply to pelvis is intact
- Bypass can be performed even if one or more tibial arteries are occluded in the leg
- PTA : percuatneous transluminal angioplasty
- Emotional decision for the patientCause of depressionMore hospital stayMortality of 5-10% (BKA) and 15%(AKA)
- Predictors of wound healing