
Recommended
Recommended
More Related Content
Similar to DIET QUALITY OF COLLEGIATE ATHLETESK elly W ebber, PhD, RD.docx
Similar to DIET QUALITY OF COLLEGIATE ATHLETESK elly W ebber, PhD, RD.docx (20)
More from mariona83
More from mariona83 (20)
Recently uploaded
Recently uploaded (20)
DIET QUALITY OF COLLEGIATE ATHLETESK elly W ebber, PhD, RD.docx
- 1. DIET QUALITY OF COLLEGIATE ATHLETES K elly W ebber, PhD, RD, LD University o f Kentucky A manda Ireland Stoess, M .S ., RD, LD University o f Kentucky H azel F orsythe, PhD,RD University o f Kentucky Janet K urzynske, PhD, RD University o f Kentucky C orresponding A uthors: Joy Ann Vaught, M S , R D , LD University o f Kentucky Bailey Adams, M S, R D , L D University o f Kentucky Abstract Background/Objectives: Collegiate athletes generally appear healthy according to weight for height and body fat standards. Despite the fact that there are well known connections between athletic performance and nutrition, little is known about the diets o f collegiate athletes. The objective o f this study was to determine the diet quality o f 138 collegiate athletes.
- 2. Subjects and Methods: Data were collected in the laboratory and via survey. Anthropometries were assessed using a free standing sta- diometer and the BodPod® for body fat assessment. The Block 2005 Food Frequency Questionnaire© was used to assess diet. The Healthy Eating Index (HEI) 2005 was used to calculate diet quality scores. Results: The average BM1 was 23.2 + 2.3 kg/m2 and the average body fat was 17.8 % ± 6.5. The average HEI score was 51.2 + 8.8 out o f 100 possible. Higher HEI scores were correlated with higher body fat percentages in this sample. Diets were adequate in calcium, iron, and vitamin C. Diets were inadequate in fiber, fruits and vegetables. The athletes had excessive intakes o f sodium and percent fat. Conclusion: These findings demonstrate the need for and potential benefit o f nutrition education for collegiate athletes. Keywords: Diet quality, collegiate athletes, Healthy Eating Index 2005, Block 2005 Food Frequency Questionnaire, Nutrition Knowledge 251
- 3. 252 / College Student Journal Introduction College athletes spend hours a day train- ing for their sport. While physical achieve- ments require training, more emphasis may be needed on the diet quality of these athletes. An athletes’ macronutrient and mi- cronutrient intake have an influence on the athletes physical output (Bonci, 2011). Nu- tritional needs for athletes vary based on the type of sport, hours spent training, season, weather conditions, gender, and body mass index. Nutritional needs also vary between training days and competition days. Athletes who consume a balanced diet tend to per- form better than those who have poor diet quality (Bonci, 2011). Depending on the sport, physical appear- ance is often important to the coach and the athlete. Some athletes and coaches tend to be more concerned about physical appear- ance than nutritional intake. Collegiate ath- letes may be pressured by their coaches and strength staff to have a specific body size because of performance expectations and comparison with other competitors (Hoogen- boom et al 2009). While body size can play an important role in performance, the nutritional status of an athlete also plays an important role (Rodriguez, DiMarco, & Langley, 2009). Athletes receive most of their nutrition knowledge from the coaches, strength and
- 4. conditioning staff, and athletic training staff; however, the accuracy of the information they receive may be questionable (Torres-McGe- hee et al 2012). These athletic professionals may have some general knowledge of nutri- tion; however, they are not licensed nutrition professionals. Some colleges provide their athletes with access to nutrition professionals but many do not. It is important for athletes to consume adequate nutrients for both short-term per- formance goals and long-term health. Many athletes have health issues after their careers are concluded because nutritional care of their bodies’ was not a priority during their athletic careers. Some of the health concerns that female athletes face later in life are high risks of arthritis, infertility and obesi- ty (Manore 1999) while male athletes face risks for orthopedic problems in addition to arthritis and obesity. Athletes have also been found to have more degenerative joint and spine problems compared to a control popu- lation (Kujala et al 2003). The purpose of this study was to assess the diet quality and body composition of male and female collegiate athletes. Overall diet quality, as well as food groups, macro and micronutrients, and total calories were assessed. Body composition was assessed using body mass index and body fat percent- age. The relationship between diet quality and body composition was also assessed.
- 5. This is one of the few studies to assess colle- giate athlete diet quality and its’ relationship to body composition. Subjects and Methods Study Design The study was a cross-sectional study and data were collected between September 2010 and January 2012 on collegiate athletes who volunteered. This study was based at a university and approved by the university Institutional Review Board (IRB). All ath- letes signed consent forms for participation. Data were taken from the first measurement of an individual athlete when more than one assessment was conducted during the study period. The athletes’ height and weight were measured and his/her body composition was determined using air displacement plethys- mography with the BodPod® (Fields, Hunter and Goran, 2000). The athletes’ demographics were also collected by a questionnaire at the initial assessment. The athletes completed a Block 2005 Food Frequency Questionnaire© and a diet quality score was calculated using the Healthy Eating Index 2005. Diet Quality Of Collegiate Athletes / 253 Participants Participants were drawn from college ath- letes involved in various sports. A total o f 138
- 6. male and female athletes signed consent forms and completed data at the time of data analy- sis. All participants were 18+ years o f age and were on the active roster for their team. Food Frequency Questionnaire The Block 2005 Food Frequency Ques- tionnaire© was used to assess the athletes’ diets (Block et al., 1986). The question- naire contains questions on over 100 foods and includes portion size and frequency of consumption. The validity (r = 0.59) and reliability (r = 0.75) o f the Block FFQ was confirmed among a sample o f Canadian women (Boucher et al., 2006). The analysis o f the questionnaires was conducted at Nutri- tionQuest (Berkeley, CA, USA). The intake o f macronutrients, micronutrients and food group servings were obtained from the anal- ysis. The intake from supplements was not included in the dietary data. All analyses were performed using SPSS, version 19.0 (SPSS Inc., Chicago, IL, USA). The Healthy Eating Index 2005 The Flealthy Eating Index (HEI) 2005 was used to determine diet quality. This measure assesses diet quality that conforms to the United States (U.S.) federal dietary guidance and recommendations published in the 2005 Dietary Guidelines for Americans. The components on the HEI 2005 index and the scoring standards are shown in Table I (Guenther, Krebs-Smith, Reedy, Britten,
- 7. Juan, Lino, Carlson, Hiza & Basiotis, 2005). The HEI is a valuable tool in that it meets the least restrictive o f food-group recommenda- tions for diets expressed on a per 1000 kcal basis-and receives maximum scores for the nine adequacy components o f the index. Lesser amounts were prorated linearly. The following three components measuring mod- eration and population probability densities were examined when setting the standards for minimum and maximum scores for these components: (i) Saturated Fat, (ii) Sodium and (iii) Calories from Solid Fats, Alcoholic Beverages and Added Sugars (SoFFAS). SoFFAS is a proxy for the discretionary cal- orie allowance (Guenther et al., 2008a). The HEI-2005 measure was previously shown to be valid for assessing diet quality (Guenther et al., 2008). The HEI-2005 score is highly associated with plasma biomarkers including: vitamin C (r = 0.41), a-carotene (r = 0.28), P-carotene (r = 0.28), P-cryptoxanthin (r = 0 .4 1 ) and lutein (r = 0.23) (Hann et al., 2001). See Table I. Results There were a total o f 138 participants in the study. The sample was 65.2% female and 89.1% Caucasian. The average age o f all the participants was 19.4 years old. There were five sports represented in this study. The lean sports included gymnastics, and swimmers and divers. The ball sports included soccer, basketball and volleyball. Those in their first
- 8. year o f school made up 42.8% o f the study. The mean body mass index for all o f the participants was 23.2 (2.3) kg/m2. The male participants had a mean body mass index of 23.6 (2.4) kg/m2. The females had a mean body mass index o f 22.9 (2.2) kg/m2 (P=0.07). All o f the participants had an average body fat o f 17.8 (6.5%). The male participants had a body fat o f 11.1(3.9%), females were 24.1 (4.5%) (PO.OOl). The HEI scores for males and females differed significantly (Males= 47.7 + 7.9 and Females= 53.1 + 8.6, p<0.001). Calorie intakes were significantly different for males and females also (p<0.001). Females reported consuming fewer than recommended calories (1866.9 + 976.8) and males reported con- suming more than the recommended calories 254 / College Student Journal (3615.8 ± 2238.4). See Table II for detailed dietary intake. Overall, there was a positive correlation between diet score and percent body fat (r= 0.30; P<0.001) and no correlation between BMI and diet score, r=0.03; P=0.72. When grouping the participants by lean vs. ball sports, there was a significant difference in HEI scores in males (lean= 45.4, ball= 50.6, p=0.02). For females there was no difference
- 9. in HEI score in lean vs. ball sports (lean= 54.7, ball= 52.0, p=0.14). Discussion The purpose o f this study was to determine the diet quality o f collegiate athletes and to determine which groups o f athletes might be most at risk for nutritional deficiencies. In this study, athletes with lower body fat had lower HEI scores. Females had better diet quality than males and males in the ball sports had better diet quality than males in sports that require a leaner body type. Cumulatively, the participants had diets that were high in solid fats, alcohol, and added sugar (SoFAS). Their diets were also high in sodium and lacked in fiber and fruit. Previous studies have found that diet qual- ity in collegiate athletes affects performance. Both malnourishment and over-nourishment can have a negative impact on an athletes’ performance (Quatromoni, 2008). According to Quatromoni, there is a need for nutrition education for athletes because meal skipping, limited finances and limited cooking skills are common issues for athletes. It is also very common for athletes to have misconceptions about the types and amount o f food that they should be eating (Quatromoni, 2008). Skinner, Kopeck, Seburg, Roth and Lew- is developed a medical nutrition therapy protocol for female athletes because female
- 10. athletes tend to be at the highest risk for suboptimal caloric intake, stress fractures, and eating disorders (Skinner et al, 2001). According to these authors, there needs to be Table I. Healthy Eating Index 2005 Component Maximum Points Standard for Maximum Score Standard for minimum score of zero Total Fruit (includes 100% juice) 5 >0.8 cups equiv. per 1,000 Calorie No Fruit Whole Fruit (not juice) 5 >0.4 cups equiv. per 1,000 Calorie No Whole Fruit Total Vegetables 5 >1.1 cups equiv. per 1,000 Calorie No Vegetables Dark Green and Orange Vegeta- bles and Legumes 5 >0.4 cups equiv. per 1,000 Calorie No Dark Green or Orange Vegetables or Legumes Total Grains 5 >3.0 cups equiv. per 1,000 Calorie No Grains Whole Grains 5 >1.5 cups equiv. per 1,000 Calorie No Whole Grains
- 11. Milk 10 >1.3 cups equiv. per 1,000 Calorie No Milk Meat and beans 10 >2.5oz equiv. per 1,000 Calorie No Meat or Beans Oils 10 >12 grams equiv. per 1,000 Calorie No Oil Saturated Fat 10 <7% o f energy >15% o f energy Sodium 10 >0.7 grams equiv. per 1,000Calorie >2.0 grams o f 1,000 Caloric Calories from Solid Fats, Alcoholic beverages, and added sugars (SoFAS) 20 <20% o f energy >50% o f energy Diet Quality Of Collegiate Athletes / 255 a consistent MNT for collegiate athletes in order to prevent health issues that are caused by inadequate nutrition. Four nutrition re- lated issues were highlighted: amenorrhea, decreased bone density, hydration and iron status Nutrition education and intervention are key to preventing these health issues that can have long term negative effects (Skinner et al 2001). In a study by Shriver, Betts, and Wol- lenberg, the diets of female college athletes
- 12. were assessed using a 3-day food record, 24 hour dietary recall, a nutrition questionnaire and anthropometric data. The diets of these athletes were compared to minimum recom- mendations for athletes. Only 9 percent of the athletes met their energy needs, 25% met their carbohydrate needs and 16% monitored their hydration status. This study speaks to the need for both nutrition intervention and nutrition education (Shriver, Betts and Wol- lenberg, 2013). While female athletes have a higher rate of disordered eating than male athletes (Thrash and Anderson, 2003), male athletes are certainly not immune to disordered eating patterns that cause long term metabolic dis- turbances (Chatterton and Petrie, 2013). In a survey of 732 male collegiate athletes the most common form of weight control was dieting and males that participated in weight controlled sports had the highest rates of dieting (Chatterton and Petrie, 2013). While dieting can aid in weight loss, it is important that athletes consume all required nutrients to prevent long term health effects. If an athlete is not educated on proper nutrition than nutri- tional deficiencies can be caused by dieting (Chatterton and Petrie, 2013). The strengths and limitations of this study are related to variation in the types of sport. One limitation may be the composition of the pool of athletes studied. The small numbers of male and female athletes in each sport make
- 13. it hard to generalize this to a larger popula- tion. In order to gather a large enough pool of both male and female athletes in one sport would require a larger longitudinal study to build a statistically relevant pool. However, the study is strengthened by the diversity of participants. There was a large enough sample size to see differences in groups and start to pinpoint which athletes might be at greatest risk for malnutrition and benefit most of a nutritional intervention. The practice implications of these find- ings suggest that college athletic staff should include nutrition care for their athletes’ that Table II. Dietary Intake Fem ale In tak e Fem ale Recom m endation M ale Intake Male R ecom m endation Calories 1867 2400 3616 3000 Fruits (cups/day) 1.6 2 1.8 2 Vegetables (cups/day)
- 14. 2.0 2.5 3.1 2.5 Fiber (gm) 9 per 1000 calories 14 per 1000 calories 8 per 1000 calories 14 per 1000 calories SoFAS Calories 965 per 2000 calorics 267 per 2000 calories 1020 per 2000 calorics 267 per 2000 calories Sodium (mg) 2875 2300 5803 2300 256 / College Student Journal supports the long term health o f the athlete. While arthritis, orthopedic disorders, and infertility may not be widespread disorders, they pose issues that cannot be ignored in terms o f individual wellbeing and health care costs. The serious nature o f nutrition care should be noted as obesity and nutrition relat- ed diseases become more endemic in the pop-
- 15. ulation. Athletes’ risks for obesity and other health issues should not be ignored. Athletic staff should be proactive when considering the nutritional health o f their athletes for both athletic performance and future health. References 1. B o n d LJ. Eating for performance: bringing science to the training table. Clin Sports Med 2011; 30(3), 661. 2. Hoogenboom BJ, Morris J, Morris C, & Schaefer K. Nutrition Knowledge and Eating Behaviors o f Female, Collegiate Swimmers. N Am J Sports Phys Ther 2009; 4(3), 139-148. 3. Rodriguez NR, DiMarco NM, & Langley S. Position o f the American Dietetics Association, Dietitians o f Canada, and the American College o f Sports Medi- cine: Nutrition and Athletic Performance. J Am Diet Assoc 2009; 109(3), 509-527. 4. Torres-McGehee, TM., Pritchett KL, Zippel D, Minton DM., Cellamare A, & Sibilia M. Sports Nutrition Knowledge Among Collegiate Athletes, Coaches, Athletic Trainers, and Strength and Conditioning Specialists. J Athl Train 2012; 47(2), 205-211. 5. Manore M. Nutritional Needs o f the Female Athlete. Clin Sports M ed 1999; 18 (3) 549-563. 6. Kujala UM, Orava S, Parkkari J, Kaprio J, & Sama S. Sports Career Related Musculoskeletal Injuries: Long-Term Flealth Effects on Former Athletes. Or- thop J Sports Med 2003; 33(12).
- 16. 7. Fields D, Hunter G, & Goran M. Validation o f the BOD POD with hydrostatic weighing: influence of body clothing. Int J Obes 2000; 24(2), 200 8. Assessment and analysis services: Question- naires and screeners. (2013). Retrieved from h t t p : / /w w w . n u t r i t i o n q u e s t . c o m / a s s e s s m e n t / list-of-qucstionnaires-and-screeners/ 9. Guenther PM, Krebs-Smith S, Reedy M, Britten P, Juan WY, Lino M, Carlson A, & Basiotis PP. Healthy eating index-2005. Retrieved from website: http:// w w w .c n p p .u sd a .g o v /P u b lic a tio n s/H E I/h e a lth y - catingindcx.2005factsheet.pdf 10. Guenther PM, Reedy J, & Krebs-Smith SM. Devel- opment o f the Healthy Eating Index-2005. J Am Diet Assoc 2008; 108(11) 1896. 11. Quatronomi P. Clinical Observations from Nutrition Services in College Athletes. J Am Diet Assoc 2008; 108(4) 689-694 12. Skinner P, Kopecky L, Scburg S, Roth T, Eich J, Lew- is NM. Development o f a Medical Nutrition Therapy Protocol for Female Collegiate Athletes. J Am Diet Assoc 2008; 101: 914-917. 13. Shrivcr LH, Betts NM, & Wollcnbetg G. Dietary Intakes and Eating Habits o f College Athletes: Are Female Col- lege Athletes Following the Current Sports Nutrition Standards? Am J Health Stud 2012; 61(1) 10-16. 14. Thrash LE, Anderson JJB. The Female Athlete Triad:
- 17. Nutrition, Menstrual Disturbances, and Low Bone Mass. Nutt Today Sep/Oct 2012; 168-174. 15. Chattcrton JM, Petrie TA. Prevalence o f disordered eating and pathogenic weight control behaviors among male collegiate athletes. J Eat Disord 2013; 21(4):328^tl. http://www.nutritionquest.com/assessment/ http://www.cnpp.usda.gov/Publications/HEI/healthy- catingindcx.2005factsheet.pdf http://www.cnpp.usda.gov/Publications/HEI/healthy- catingindcx.2005factsheet.pdf Copyright of College Student Journal is the property of Project Innovation, Inc. and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use. Vogel et al. Journal of the International Society of Sports Nutrition (2015) 12:12 DOI 10.1186/s12970-015-0074-y RESEARCH ARTICLE Open Access Safety of a dose-escalated pre-workout supplement in recreationally active females Roxanne M Vogel1,2, Jordan M Joy1, Paul H Falcone1, Matt M Mosman1, Michael P Kim1 and Jordan R Moon1,3* Abstract
- 18. Background: Pre-workout supplements (PWS) have increased in popularity among athletic populations for their purported ergogenic benefits. Most PWS contain a “proprietary blend” of several ingredients, such as caffeine, beta-alanine, and nitrate in undisclosed dosages. Currently, little research exists on the safety and potential side effects of chronic consumption of PWS, and even less so involving female populations. Therefore, the purpose of the present study was to examine the safety of consuming a dose-escalated PWS over a 28-day period among active adult females. Methods: 34 recreationally active, adult females (27.1 ± 5.4 years, 165.2 ± 5.7 cm, 68.2 ± 16.0 kg) participated in this study. Participants were randomly assigned to consume either 1 (G1) or 2 (G2) servings of a PWS daily or remain unsupplemented (CRL) for a period of 28 days. All were instructed to maintain their habitual dietary and exercise routines for the duration of the study. Fasting blood samples, as well as resting blood pressure and heart rate, were taken prior to and following the supplementation period. Samples were analyzed for hematological and clinical chemistry panels, including lipids. Results: Significant (p < 0.05) group by time interactions were present for absolute monocytes (CRL −0.10 ± 0.10; G1 + 0.03 ± 0.13; G2 + 0.01 ± 0.12×10E3/uL), MCH (CRL −0.13 ± 0.46; G1 + 0.36 ± 0.52; G2 -0.19 ± 0.39 pg), creatinine (CRL 0.00 ± 0.05; G1 -0.06 ± 0.13; G2 -0.14 ± 0.08 mg/dL), eGFR (CRL −0.69 ± 5.97; G1 + 6.10 ± 15.89; G2 + 14.63 ± 7.11 mL/min/1.73), and total cholesterol (CRL −2.44 ± 13.63; G1 + 14.40 ± 27.32; G2 -10.38 ± 15.39 mg/dL). Each of these variables remained within the accepted physiological range. No other variables had significant interactions. Conclusion: The present study confirms the hypothesis that a
- 19. PWS containing caffeine, beta-alanine, and nitrate will not cause abnormal changes in hematological markers or resting vital signs among adult females. Although there were statistically significant (p < 0.05) group by time interactions for absolute monocytes, MCH, creatinine, eGFR, and total cholesterol, all of the results remained well within accepted physiological ranges and were not clinically significant. In sum, it appears as though daily supplementation with up to 2 servings of the PWS under investigation, over an interval of 28 days, did not adversely affect markers of clinical safety among active adult females. Keywords: Pre-workout, Safety, Health, Female Background Nutrient timing refers to the methodical, timed ingestion of carbohydrate, protein, fat and other dietary supple- ments either before, during, or after physical activity [1]. Supplementation during the period immediately preced- ing physical activity has become an increasingly popular * Correspondence: [email protected] 1MusclePharm Sports Science Institute, MusclePharm Corp., 4721 Ironton St. Building A, Denver, CO 80239, USA 3Department of Sports Exercise Science, United States Sports Academy, Daphne, AL, USA Full list of author information is available at the end of the article © 2015 Vogel et al. ; licensee BioMed Central. Commons Attribution License (http://creativec reproduction in any medium, provided the or Dedication waiver (http://creativecommons.or unless otherwise stated. strategy among competitive and recreational athletes alike as a means of improving performance [2]. In re-
- 20. sponse to this trend, manufacturers have developed pre- workout supplements (PWS), which typically combine caffeine with any number of purported ergogenic sub- stances, such as beta-alanine, nitrate, and amino acids. As the number of PWS available on the market grows, each containing their own “proprietary blend” of active ingredients, it must be determined which, if any, are safe for chronic consumption. This becomes particularly im- portant as concerns have arisen over the concept of This is an Open Access article distributed under the terms of the Creative ommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and iginal work is properly credited. The Creative Commons Public Domain g/publicdomain/zero/1.0/) applies to the data made available in this article, mailto:[email protected] http://creativecommons.org/licenses/by/4.0 http://creativecommons.org/publicdomain/zero/1.0/ Vogel et al. Journal of the International Society of Sports Nutrition (2015) 12:12 Page 2 of 6 proprietary blends, namely the fact that the Food and Drug Administration does not monitor the amounts of ingredients used in these blends or the accuracy of prod- uct labeling by manufacturers [2]. Caffeine is one of the most commonly found ingredi- ents in PWS. An extensive amount of scientific literature exists on the ergogenic properties of caffeine [3-5]. Ac- cording to the International Society of Sports Nutrition’s position stand on caffeine and performance, it is most effective when consumed in low to moderate doses,
- 21. about 3–6 mg per kilogram bodyweight, 30–60 minutes prior to exercise [4]. Caffeine has been shown to im- prove performance in endurance events and time-trials, improve cognitive function and alertness, and delay the onset of fatigue during exhaustive exercise [3,5]. More- over, caffeine anhydrous, which is frequently used in PWS, has been shown to have greater ergogenic effects than caf- feine ingested in the form of coffee, tea, or cola [4]. Beta-alanine (BA), another common ingredient in PWS, is an amino acid which serves as a rate-limiting precursor to carnosine in skeletal muscle [6]. Carnosine’s suggested mechanism of action may be to buffer hydro- gen ions during exercise, thereby influencing intracellu- lar muscle pH, and ultimately increasing work capacity [7]. In a recent review of the literature by Quesnele et al. [8], the authors concluded that although there is evi- dence to suggest that BA supplementation enhances ath- letic performance, the safety of its use remains unclear, and there is a general under-reporting of its side effects in the literature. Despite the existing literature pertaining to individual ingredients contained in PWS and the growing number of studies that address multi-ingredient PWS specifically, we are unaware of any published reports examining the safety of PWS in a solely female population. Therefore, the purpose of the present study was to examine the safety of chronic consumption of a PWS over a 28 day period among active adult females. We hypothesized that daily PWS supplementation would not produce ab- normal changes in hematological or metabolic safety markers or resting vital signs. Methods Experimental design
- 22. In a dose-escalated, simple randomized design, 34 sub- jects were randomly assigned to control (CRL, n = 16; 27.1 ± 5.9 y, 166.2 ± 4.0 cm, 65.2 ± 12.9 kg), 1 serving (G1, n = 10; 24.9 ± 3.9 y, 164.7 ± 5.8 cm, 72.4 ± 23.3 kg), or 2 serving (G2, n = 8; 29.6 ± 5.8 y, 163.8 ± 8.8 cm, 69.0 ± 11.6 kg) groups via random number generation by the investigators and asked to remain unsupplemented, or consume either 1 or 2 servings, respectively, of a pre- workout formula (Fitmiss Ignite™, MusclePharm Corp., Denver, CO) every day for 28 days. The pre-workout formula contained 1 g of carbohydrate, 23 mg of Cal- cium, and 5,700 mg of a proprietary blend consisting of beta-alanine, choline bitartrate, L-tyrosine, glycine, tau- rine, L-carnitine, beetroot extract, hawthorn berry pow- der, agmatine sulfate, caffeine anhydrous, and huperzine A. The supplement was analyzed by a third party (Euro- fins Supplement Analysis Center, Petaluma, CA) and verified to contain all of the ingredients on the label. Subjects were instructed to consume 1–2 level scoop(s) of the supplement with 12 oz water per scoop either 30 minutes prior to exercise or at the same time of day on rest days. Compliance was monitored using supple- ment consumption logs, as well as by weighing supple- ment containers before and after the supplementation period. A total of 38 subjects were initially recruited for this study. From G1, one subject discontinued the study due to noncompliance, and from G2, three subjects dis- continued due to noncompliance. The CRL group con- tained more total participants, as CRL group data was added from a previously conducted study which fea- tured a design exactly identical to the present study. Participants completed the study with an average sup- plementation compliance of 94.6% for G1 and 100% for G2. Blood draws were taken prior to and following the supplementation period. Approval for the human sub- ject protocol was obtained from MusclePharm Sports
- 23. Science Institute’s IRB, and subjects were provided with written informed consent documents prior to participa- tion in the study. Participants 34 recreationally active female adults (27.1 ± 5.4 years, 165 ± 5.7 cm, 68.2 ± 16.0 kg) participated in the study. Recreationally active was defined as habitually participat- ing in moderate to vigorous physical activity on three or more days a week for a duration of thirty minutes or more. Subjects were required to be non-smokers, free of any disease or disorder which may have produced con- founding effects, and have abstained from taking any other pre-workout supplements for one month prior to the beginning of the study. Exclusion criteria included having a significant history or current presence of a treated condition, such as high blood pressure (≥140 mmHg systolic and/or ≥90 mmHg diastolic), tachyarrhythmia, or heart, kidney, or liver disease, or any contraindication to physical activity. Also excluded from the study were participants whose willingness or ability to comply with the study protocol was uncertain. Eligibility was determined upon evaluation of pre- participation health history, exercise, and supplementa- tion screening questionnaires. A caffeine usage question- naire was given as part of the pre-participating screening process, with average self-reported caffeine consumption prior to study being 131 mg/day for G1 and 269 mg/day Vogel et al. Journal of the International Society of Sports Nutrition (2015) 12:12 Page 3 of 6 for G2. Subjects were instructed to maintain their habit- ual dietary and exercise routines, and to not take any additional supplements during their participation in the
- 24. study. Measurements All measurements were taken prior to and following the 28-day supplementation period in a quiet, temperature controlled private office. Upon arrival at the office, sub- jects were instructed to remain seated quietly for 15 mi- nutes before resting vital signs, height, and weight were taken. Subjects then submitted a blood sample in the fasted state. All blood draws were performed in the morning to prevent diurnal variations by a trained phle- botomist via venipuncture. Samples were analyzed for comprehensive metabolic panels, complete blood counts and lipid profiles by an external laboratory (Laboratory Corporation of America, Denver, CO). Variables re- corded from blood analysis consisted of white blood cell count (WBC), red blood cell count (RBC), hemoglobin, hematocrit, mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), red blood cell dis- tribution width (RDW), platelets (absolute), neutrophils (percent and absolute), lymphocytes (percent and abso- lute), monocytes (percent and absolute), eosinophils (percent and absolute), basophils (percent and absolute), serum glucose, blood urea nitrogen (BUN), creatinine, estimated glomerular filtration rate (eGFR), BUN:cre- atinine, sodium, potassium, chloride, carbon dioxide, cal- cium, protein, albumin, globulin, albumin:globulin, bilirubin, alkaline phosphatase, aspartate aminotransfer- ase (AST), alanine aminotransferase (ALT), total choles- terol, triglycerides, high density lipoprotein (HDL) cholesterol, and low density lipoprotein (LDL) choles- terol. Inter-test reliability results from 12 men and women measured up to one week apart at the aforemen- tioned laboratory resulted in no significant differences for any of the variables noted above from day-to-day (p > 0.05) and an average inter-test Coefficient of Vari-
- 25. ation (CV) of 6.9%. Statistical analyses Data was analyzed using a 3×2 repeated measures ANOVA model for all group, time, and group by time in- teractions. A Bonferroni post-hoc analysis was used to lo- cate differences. Shapiro-Wilk tests were used to determine normality of the data. The Minimal Difference (MD) needed to be considered real was determined using the method previously described by Weir [9]. Data are presented as means ± standard deviation. All data were analyzed using Statistica software (Statsoft, Version 10). Results Significant group by time interactions were present for ab- solute monocytes (p < 0.05), wherein CRL decreased rela- tive to G1 and G2. Absolute monocytes had a normal distribution at baseline (p = 0.07), yet the distribution was positively skewed (p < 0.05) after the supplementation period. Significant group by time interactions were ob- served with MCH (p < 0.05), with G1 increasing relative to CRL and G2. Significant group by time interactions were detected for creatinine (p < 0.05), with G2 decreasing rela- tive to CRL. Significant group by time interactions were noted for eGFR (p < 0.05), with G2 increasing relative to control. Significant group by time interactions were also present for total cholesterol (p < 0.05), G1 increasing relative to CRL and G2. Total cholesterol was positively skewed at baseline (p < 0.05), and at post-supplementation, it became normally distributed (p = 0.99). MCH and eGFR were normally distributed (p > 0.05) at both time points, and creatinine was positively skewed (p < 0.05) at both time points. All variables remained within the accepted physio- logical range at baseline and post supplementation. No other variables had significant group by time interactions. Data are presented in Additional file 1 as means ± standard deviation. Tolerability data collected from participants reported no serious adverse events. The most common re-
- 26. ported side effects were a tingling sensation (n = 6), itchi- ness (n = 2), and nausea (n = 2). Other reported side effects included dizziness, lightheadedness, dry mouth, headache, a burning sensation, and diarrhea (all n = 1). Most of these effects occurred within the first several days of supplemen- tation and subsided over time. Discussion The results of the present study suggest that daily sup- plementation with the PWS under investigation does not appear to cause any abnormal changes in hematological and clinical chemistry/metabolic safety markers or rest- ing vital signs in female subjects. While significant group by time interactions (p < 0.05) were observed for abso- lute monocytes, MCH, creatinine, eGFR, and total chol- esterol, all group values remained well within the accepted physiological range and were not clinically sig- nificant. While remaining within range, unusual effects were observed between groups. For instance, the CRL group decreased relative to G1 and G2 for absolute monocytes, and for MCH and total cholesterol, G1 in- creased relative to both CRL and G2. Similar to total cholesterol, although not reaching significance (p > 0.05), both LDL and HDL increased in G1 but decreased in G2 over time. These findings are somewhat discrepant, since intuitively, one would think that if a lower dose in- creases a given parameter compared to control, then a higher dose should amplify this effect. This, however, was not the case. Such results suggest a natural variation Vogel et al. Journal of the International Society of Sports Nutrition (2015) 12:12 Page 4 of 6 in these clinical markers, and may not necessarily be re- lated to supplementation. Additionally, the control
- 27. group (n = 16) was larger than either of the experimental groups (G1, n = 10; G2, n = 8), so individual variations within the experimental groups had greater impact on the group mean values. Variables that were significantly different at the group level were evaluated at the individual level to determine clinical significance. Analysis of clinical significance at the individual level was conducted using the MD statis- tic, which calculates the magnitude of the inter-test dif- ference (between baseline and post-supplementation) needed to be exceeded in order for a single measure- ment to be considered real, as described by Weir [9]. The MD is calculated using the standard error of meas- urement (SEM), which is considered an absolute index of the reliability of a given test/measurement, not rela- tive to the characteristics of the sample or population from which values were obtained. Unlike other reliability measures, such as the CV, the SEM and thus the MD, are not affected by between-subject variability [9]. If a subject’s measured values exceeded the MD, the change was considered a true change. Clinical significance at the individual level was reached when a score that exceeded the MD crossed the upper or lower limits of the ac- cepted physiological range for each variable. For creatin- ine, this occurred in three subjects, one from G1 and two from G2, wherein values decreased pre to post, bringing them within the clinical reference range. For total cholesterol, changes observed in two subjects from G1 and one from G2 exceeded the MD. Specifically, the two subjects from G1 increased over time, moving from within range to out of range, while the subject from G2 decreased pre to post, entering the accepted reference range. Also worth noting is the fact that three individ- uals from the CRL group experienced changes in total cholesterol values that both exceeded the MD and
- 28. moved in or out of range. In this case, one subject in- creased over time to leave the accepted range, one started outside of the range and remained out of range, and one decreased pre to post, entering back into range. All subjects remained within 3 standard deviations of the mean and exceeded the MD. Collectively, individual analysis supports the present hypothesis and also sup- ports the notion of intra-subject diurnal variability. Fur- thermore, absolute monocytes and total cholesterol were distributed differently pre to post, increasing the prob- ability for a type 1 statistical error [10]. These findings generally agree with previous literature. Aside from the research pertaining to PWS effects on performance [11-16], only a limited number of studies have also examined the clinical safety of PWS. Kedia et al. [17] looked at the effects of a multi-ingredient PWS containing caffeine, betaine, and dendrobium extract on body composition, performance measures, and hematological markers of clinical safety in healthy, young men and women undergoing concurrent resist- ance training for six weeks. While the investigators did not see an improvement in objective assessments of ex- ercise performance or body composition with supple- mentation, they found the PWS to be well tolerated with no significant changes in clinical laboratory safety markers at the end of six weeks. Similarly, Shelmadine et al. [18] examined the effects of 28 days consuming a commercially available PWS, NO-Shotgun®, combined with heavy resistance exercise on body composition, muscle strength and mass, myofi- brillar protein content, markers of satellite cell activa- tion, and clinical safety markers in male subjects. They found no negative side effects or abnormal impact on clinical safety markers after 28 days of supplementation.
- 29. In a follow up study of the same nature, this time with a post-workout supplement added (NO-Synthesize®), Spil- lane et al. [19] again found no detrimental effects on clinical safety markers following 28 days supplementa- tion and resistance training with NO-Shotgun®. Farney et al. [20] investigated hemodynamic and hematological effects of two supplements containing caf- feine and 1,3- dimethylamylamine (a constituent of gera- nium) after 14 days of supplementation in men and women, and found only a significant change in blood glucose for one of the supplements (Jack3d™) over this time period. A follow up to this study conducted by Whitehead et al. [21] supplemented with the same prod- uct containing caffeine and 1,3- dimethylamylamine (Jack3d™) over a 10-week period in healthy males and also found it did not negatively impact hematological markers of health when consumed daily. Kendall et al. [22] investigated the safety and efficacy of a PWS containing caffeine, creatine, beta-alanine, amino acids and B-vitamins in recreationally trained, college-age men over an identical period of 28 days. In that study, no adverse effects were observed for renal or hepatic clinical blood markers or resting vital signs. Re- searchers concluded that PWS with similar ingredients in similar doses should be safe for ingestion periods up to 28 days in healthy males. More recently, Joy et al. [23] found that supplementation with a PWS containing caf- feine, nitrate, and amino acids in healthy, recreationally active men and women was apparently safe when taken within recommended dosage guidelines for 28 days. To our knowledge, this is the first study assessing the clinical safety of a PWS in an all-female population. Female-specific recommendations for sports nutrition
- 30. and supplementation is an area that warrants more attention. A review article by Volek, Forsythe, and Kraemer [24], for instance, identifies the subtle, yet important differ- ences in exercise metabolism between male and female Vogel et al. Journal of the International Society of Sports Nutrition (2015) 12:12 Page 5 of 6 athletes. The authors suggest that nutritional strategies, in- cluding nutrient timing and supplement use, should be tai- lored to meet the sex-specific needs of female athletes. In another review article addressing gender differences in sports nutrition, Tarnopolsky [25] similarly concluded that future studies in nutrition and metabolism should exam- ine and consider sex differences in response to supple- mentation and exercise. It therefore seems prudent for future research to continue to address sports nutrition supplementation in females to evaluate both safety and ef- ficacy in this population as compared to males. Limitations The present study included a short duration supplemen- tation period and small sample size. Future studies should examine the effects of supplementation for lon- ger than 28 days among more subjects, especially given the fact that statistically significant interactions did take place over time in the present study. Again, while none of the significant variables left the accepted physiological range, the possibility that these could be the beginnings of adverse trends cannot be ruled out. This leaves long- term safety of PWS supplementation, at least greater than 28 days, still open to question. Conclusion This study supports the hypothesis that a PWS contain-
- 31. ing caffeine, beta-alanine, and nitrate will not cause ab- normal changes in hematological or clinical chemistry/ metabolic markers, or resting vital signs among recre- ationally active females. Although there were statistically significant (p < 0.05) group by time interactions for abso- lute monocytes, MCH, creatinine, eGFR, and total chol- esterol, all of the results remained well within accepted physiological ranges and were not clinically significant. In sum, it appears as though daily supplementation with up to 2 servings of the PWS used in this investigation, over a period of 28 days, had no adverse impact on markers of clinical safety among active adult females. Additional file Additional file 1: Data collected pre and post supplementation. Abbreviations PWS: Pre-workout supplement(s); BA: Beta-alanine; WBC: White blood cell; RBC: Red blood cell; MCV: Mean corpuscular volume; MCH: Mean corpuscular hemoglobin; MCHC: Mean corpuscular hemoglobin concentration; RDW: Red blood cell distribution width; BUN: Blood urea nitrogen; eGFR: Estimated glomerular filtration rate; AST: Aspartate aminotransferase; ALT: Alanine aminotransferase; CV: Coefficient of variation; MD: Minimum difference; SEM: Standard error of measurement. Competing interests RV, JJ, PF, MM, MK and JM are employees of the funding source, MusclePharm Corporation. However, this publication should not
- 32. be viewed as endorsement by the investigators, Metropolitan State University of Denver, the United States Sports Academy, or MusclePharm Corporation. Authors’ contributions RV, JJ, and PF participated in data collection for this investigation. All authors contributed to the conception of the experimental design, drafting of the manuscript, and interpretation of data. All authors have read and approved the final manuscript. Acknowledgements We would like to thank all of the participants as well as MusclePharm Corporation for supplying product and funding the investigation. Author details 1MusclePharm Sports Science Institute, MusclePharm Corp., 4721 Ironton St. Building A, Denver, CO 80239, USA. 2Metropolitan State University, Denver, CO, USA. 3Department of Sports Exercise Science, United States Sports Academy, Daphne, AL, USA. Received: 19 December 2014 Accepted: 16 February 2015 References 1. Kerksick C, Harvey T, Stout J, Campbell B, Wilborn C, Kreider R, et al.
- 33. International society of sports nutrition position stand: nutrient timing. J Int Soc Sports Nutr. 2008;5:17. 2. Eudy AE, Gordon LL, Hockaday BC, Lee DA, Lee V, Luu D, et al. Efficacy and safety of ingredients found in preworkout supplements. Am J Health Syst Pharm. 2013;70:577–88. 3. Astorino TA, Roberson DW. Efficacy of acute caffeine ingestion for short-term high-intensity exercise performance: a systematic review. J Strength Cond Res. 2010;24:257–65. 4. Goldstein ER, Ziegenfuss T, Kalman D, Kreider R, Campbell B, Wilborn C, et al. International society of sports nutrition position stand: caffeine and performance. J Int Soc Sports Nutr. 2010;7:5. 5. Graham TE. Caffeine and exercise: metabolism, endurance and performance. Sports Med. 2001;31:785–807. 6. Harris RC, Wise JA, Price KA, Kim HJ, Kim CK, Sale C. Determinants of muscle carnosine content. Amino Acids. 2012;43:5–12. 7. Derave W, Everaert I, Beeckman S, Baguet A. Muscle carnosine metabolism and beta-alanine supplementation in relation to exercise and training. Sports Med. 2010;40:247–63.
- 34. 8. Quesnele JJ, Laframboise MA, Wong JJ, Kim P, Wells GD. The effects of beta-alanine supplementation on performance: a systematic review of the literature. Int J Sport Nutr Exerc Metab. 2014;24:14–27. 9. Weir JP. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J Strength Cond Res. 2005;19:231–40. 10. Delaney HD, Vargha A. The effect of nonnormality on student's two-sample t test. In: The education resources information center. U.S. Department of Education. 2000. http://eric.ed.gov/?q=ED443850&id=ED443850. Accessed 20 November 2014. 11. Fukuda DH, Smith AE, Kendall KL, Stout JR. The possible combinatory effects of acute consumption of caffeine, creatine, and amino acids on the improvement of anaerobic running performance in humans. Nutr Res. 2010;30:607–14. 12. Hoffman JR, Kang J, Ratamess NA, Hoffman MW, Tranchina CP, Faigenbaum AD. Examination of a pre-exercise, high energy supplement on exercise performance. J Int Soc Sports Nutr. 2009;6:2. 13. Lowery RP, Joy JM, Dudeck JE, Oliveira de Souza E, McCleary SA, Wells S, et al. Effects of 8 weeks of Xpand(R) 2X pre workout supplementation on
- 35. skeletal muscle hypertrophy, lean body mass, and strength in resistance trained males. J Int Soc Sports Nutr. 2013;10:44. 14. Outlaw JJ, Wilborn CD, Smith-Ryan AE, Hayward SE, Urbina SL, Taylor LW, et al. Acute effects of a commercially-available pre-workout supplement on markers of training: a double-blind study. J Int Soc Sports Nutr. 2014;11:40. 15. Smith AE, Fukuda DH, Kendall KL, Stout JR. The effects of a pre-workout supplement containing caffeine, creatine, and amino acids during three weeks of high-intensity exercise on aerobic and anaerobic performance. J Int Soc Sports Nutr. 2010;7:10. 16. Spradley BD, Crowley KR, Tai CY, Kendall KL, Fukuda DH, Esposito EN, et al. Ingesting a pre-workout supplement containing caffeine, B- vitamins, amino http://www.jissn.com/content/supplementary/s12970-015-0074- y-s1.xlsx http://eric.ed.gov/?q=ED443850&id=ED443850 Vogel et al. Journal of the International Society of Sports Nutrition (2015) 12:12 Page 6 of 6 acids, creatine, and beta-alanine before exercise delays fatigue while improving reaction time and muscular endurance. Nutr Metab (Lond). 2012;9:28.
- 36. 17. Kedia AW, Hofheins JE, Habowski SM, Ferrando AA, Gothard MD, Lopez HL. Effects of a pre-workout supplement on lean mass, muscular performance, subjective workout experience and biomarkers of safety. Int J Med Sci. 2014;11:116–26. 18. Shelmadine B, Cooke M, Buford T, Hudson G, Redd L, Leutholtz B, et al. Effects of 28 days of resistance exercise and consuming a commercially available pre-workout supplement, NO-Shotgun(R), on body composition, muscle strength and mass, markers of satellite cell activation, and clinical safety markers in males. J Int Soc Sports Nutr. 2009;6:16. 19. Spillane M, Schwarz N, Leddy S, Correa T, Minter M, Longoria V, et al. Effects of 28 days of resistance exercise while consuming commercially available pre- and post-workout supplements, NO-Shotgun(R) and NO- Synthesize(R) on body composition, muscle strength and mass, markers of protein synthesis, and clinical safety markers in males. Nutr Metab (Lond). 2011;8:78. 20. Farney TM, McCarthy CG, Canale RE, Allman Jr RJ, Bloomer RJ. Hemodynamic and hematologic profile of healthy adults ingesting dietary supplements containing 1,3-dimethylamylamine and caffeine. Nutr Metab Insights.
- 37. 2012;5:1–12. 21. Whitehead PN, Schilling BK, Farney TM, Bloomer RJ. Impact of a dietary supplement containing 1,3-dimethylamylamine on blood pressure and bloodborne markers of health: a 10-week intervention study. Nutr Metab Insights. 2012;5:33–9. 22. Kendall KL, Moon JR, Fairman CM, Spradley BD, Tai C-Y, Falcone PH, et al. Ingesting a preworkout supplement containing caffeine, creatine, beta-alanine, amino acids, and B vitamins for 28 days is both safe and efficacious in recreationally active men. Nutr Res. 2014;34:442–9. 23. Joy JM, Mosman MM, Falcone PH, Tai C-Y, Carson LR, Kimber D, et al. Safety of 28 days consumption of a pre-workout supplement. J Int Soc Sports Nutr. 2014;11 Suppl 1:30. 24. Volek JS, Forsythe CE, Kraemer WJ. Nutritional aspects of women strength athletes. Br J Sports Med. 2006;40:742–8. 25. Tarnopolsky MA. Gender differences in metabolism; nutrition and supplements. J Sci Med Sport. 2000;3:287–98. Submit your next manuscript to BioMed Central and take full advantage of: • Convenient online submission
- 38. • Thorough peer review • No space constraints or color figure charges • Immediate publication on acceptance • Inclusion in PubMed, CAS, Scopus and Google Scholar • Research which is freely available for redistribution Submit your manuscript at www.biomedcentral.com/submit AbstractBackgroundMethodsResultsConclusionBackgroundMeth odsExperimental designParticipantsMeasurementsStatistical analysesResultsDiscussionLimitationsConclusionAdditional fileAbbreviationsCompeting interestsAuthors’ contributionsAcknowledgementsAuthor detailsReferences A 41-year-old woman came to the Emergency Department in January, 1998. She had awoken that morning in severe pain and had taken ibuprofen without improvement. The previous day, she had walked 4 miles. Examination showed a temperature of 36·9°C, pulse 86 beats per min, and blood pressure 118/56 mm Hg. She weighed 72 kg and her height was 158 cm. She had diffuse muscle tenderness in her thighs and biceps. No neurological deficits were noted. She was diagnosed as having musculoskeletal pain and given a prescription for paracetamol with codeine. 2 days later, she returned to the Emergency Department complaining of continued muscle pain, now accompanied by symmetrical muscle weakness. Examination again showed diffuse muscle tenderness in her arms and legs,
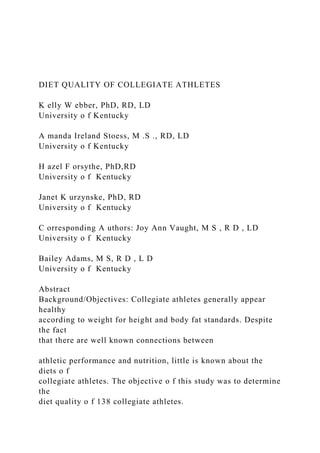
- 39. with normal muscle tone and symmetrical, proximal, and distal muscle weakness (power 4/5). Laboratory investigations showed a sodium of 141 mmol/L, potassium of 1·1 mmol/L, chloride of 98 mmol/L, bicarbonate of 33 mmol/L, blood urea nitrogen of 3·9 mmol/L, creatinine of 106 �mol/L, and a glucose of 5·8 mmol/L. Her haemoglobin was 11·9 g/dL (mean corpuscular volume 77·0 fL), albumin 3·5 g/dL, calcium 1·9 mmol/L, magnesium 0·57 mmol/L, and phosphate 0·94 mmol/L. She had high concentrations of lactate dehydrogenase (748 U/L), aspartate aminotransferase (244 U/L), and creatine kinase (CK; 13 182 U/L). Her urine was positive for myoglobin. She was admitted to hospital with a diagnosis of rhabdomyolysis and hypokalaemia. She was treated with intravenous hydration and electrolyte replacement. Her CK peaked at 21 072 U/L. Her creatinine remained normal. Further investigation of her hypokalaemia included urine chemistry (random urine potassium 3·8 m m o l / L ; normal 10–160 mmol/L), a negative screen for diuretics, and normal corticotropin and renin concentrations. We discovered from the patient’s husband that her diet consisted mostly of cheese sandwiches. She did not eat any fruits, vegetables, or meat products. No history of purging was discovered. A psychiatric consultation was arranged, but no definitive evidence for a primary eating disorder (anorexia or bulimia nervosa) was found. She received nutritional advice and was discharged. She came back to the Emergency Depratment in August, 1998, with a 1-day history of weakness. Her potassium was 1·1 mmol/L with a normal CK. An electrocardiogram showed first-degree atrioventricular block and probable TU wave fusion (figure). A h i s t o r y of purging and laxative abuse was obtained. After
- 40. medical treatment she was transferred to the psychiatric service for management of her bulimia nervosa. She was last seen in January, 1999. She had maintained more normal eating pattterns and a normal serum potassium, but had not attended for psychiatric follow-up. Rhabdomyolysis is associated with both traumatic, (crush syndrome)1 and non-traumatic causes. Rhabdomyolisis secondary to hypokalaemia is a well- described non-traumatic cause2 and has been associated with several medical conditions including use of diuretics, eating liquorice, coeliac disease, infectious diarrhoea, anorexia nervosa/bulimia, and abuse of laxatives. Rhabdomyolysis can be a life-threatening disorder, with acute renal failure being one of the most serious complications.3 Although this patient did not develop renal failure, that consequence has been associated with rhabdomyolysis secondary to laxative abuse and induced hypokalaemia.4 The primary mechanism of rhabdomyolysis secondary to hypokalaemia appears to be that potassium is released from normal contracting muscle cells resulting in a vasodilatory response of the surrounding arterioles.5 Failure of this potassium-mediated arteriolar dilation may lead to muscle ischaemia. This case demonstrates the need to include hypokalaemia in a differential diagnosis of rhabdomyolysis, and the importance of screening for eating disorders in patients with hypokalaemia associated with a low urinary potassium. Other clues in the initial presentation suggesting an underlying eating disorder include the hint of excessive exercise, her very restricted eating patterns, and the laboratory abnormalities that point to malnutrition (eg, microcytic anaemia and low calcium, magnesium, potassium, and phosphate concentrations).
- 41. R e f e r e n c e s 1 Bywater EGL, Beall D. Crush injuries with impairment of renal function. BMJ 1941; i: 4 2 7 – 3 2 . 2 Singhal PC, Abramovici M, Venkatesan J, Mattana J. Hypokalemia and rhabdomyolysis. Miner Electrolyte Metab 1991; 17: 3 3 5 – 3 9 . 3 Zager RA. Rhabdomyolysis and myohemoglobinuric acute renal failure. Kidney Int 1996; 49: 3 1 4 – 2 6 . 4 Copeland PM. Renal failure associated with laxative abuse. Psychother Psychosom 1994; 62: 2 0 0 – 0 2 . 5 Knochel PL, Schlein EM. On the mechanism of rhabdomyolysis in potassium depletion. J Clin Invest 1972; 51: 1 7 5 0 – 5 8 . Muscle pain after exerc i s e Craig Nielsen, Peter Mazzone 1062 THE LANCET • Vol 353 • March 27, 1999 Case report Lancet 1999; 353: 1062 Cleveland Clinic Foundation, Cleveland, Ohio 44195, USA (C Nielsen MD, P Mazzone MD) Correspondence to: Dr Craig Nielsen
- 42. Patient’s electrocardiogram Muscle pain after exerciseReferences