
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Ear ppt
Similar to Ear ppt (20)
Recently uploaded
Recently uploaded (20)
Ear ppt
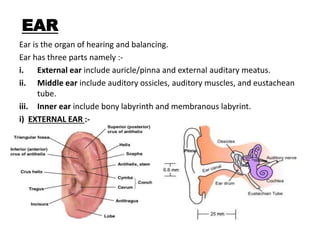
- 1. EAR Ear is the organ of hearing and balancing. Ear has three parts namely :- i. External ear include auricle/pinna and external auditary meatus. ii. Middle ear include auditory ossicles, auditory muscles, and eustachean tube. iii. Inner ear include bony labyrinth and membranous labyrint. i) EXTERNAL EAR :-
- 2. Cont…. a) Pinna/auricle :- The visible part is called the auricle, also known as the pinna. It is composed of a thin plate of yellow elastic cartilage, covered with integument, and connected to the surrounding parts by ligaments and muscles. The function of the pinna is to act as a kind of funnel which assists in directing the sound further into the ear. b) External auditory meatus :- It is a tube running from the outer ear to the middle ear. The adult human ear canal extends from the pinna to the eardrum. It is about 2.5 centimetres (1 in) in length and 0.7 centimetres (0.3 in) in diameter. The function of the ear canal is to transmit sound from the pinna to the eardrum. S shaped canal. To strenthen this canal in adult upward and backward pulling is done while in Children downward and backward is done.
- 3. Contd…. ii. MIDDLE EAR :- a) Auditory ossicles :- • The Malleus (Latin: "hammer") :- articulates with the incus through the incudomalleolar joint and is attached to the tympanic membrane (eardrum), from which vibrational sound pressure motion is passed. • The Incus (Latin: "anvil") :- It is connected to both the other bones. • The Stapes (Latin: "stirrup“) :- articulates with the incus through the incudostapedial joint and is attached to the membrane of the fenestra ovalis, the elliptical or oval window or opening between the middle ear and the vestibule of the inner ear. It is the smallest bone in the body. Note :- They serve to transmit sounds from the air to the fluid - filled labyrinth (cochlea).
- 4. Contd…. b) Auditory muscles :- Tensor tympani keep the T.M stretched for transmission of sound waves. Stapedius is the smallest skeletal muscles (1mm). It prevent the excess movement of stapes. Paralysis of this cause hyperacusis. Tympanic reflex :- When the middle ear muscles (tensor tympani and stapedius) contract, they pull the manubrium of the malleus inward and the footplate of the stapes outward.Loud sounds initiate a reflex contraction of these muscles called the tympanic reflex. Its function is protective the reaction time for the reflex is 40 to 160 ms.
- 5. Contd…. c) Eustachian tube :- The eustachian tube is a canal that connects middle ear to the nasopharynx. In adult humans the Eustachian tube is approximately 35 mm (1.4 in) long and 3 mm (0.12 in) in diameter. Function Pressure equalization. Mucus drainage. i) Normally, the Eustachian tube is collapsed, but it gapes open both with swallowing and with positive pressure. ii) when the eustachian tube will not open enough to equalize pressure, symptoms such as discomfort, dizziness, or ringing in the ear may result.
- 6. Contd…. iii) INNER EAR :- Inner ear is the innermost part of the vertebra. The inner ear is mainly responsible for sound detection and balance. It consist of a) bony labyrinth b) membranous labyrinth. CHOCHLEA :- The cochlea is the part of the inner ear involved in hearing. It is a spiral-shaped cavity in the bony labyrinth. In humans making 2 turns(full) and a 3/4(3 quarters) turn around its axis, the modiolus. A core component of the cochlea is the Organ of Corti, the sensory organ of hearing, which is distributed along the partition separating fluid chambers in the coiled tapered tube of the cochlea. The cochlea is a portion of the inner ear that looks like a snail shell.
- 7. Contd…. • Three scalae or chambers: – the vestibular duct or scala vestibuli (containing perilymph), which lies superior to the cochlear duct and abuts the oval window – the tympanic duct or scala tympani (containing perilymph), which lies inferior to the cochlear duct and terminates at the round window – the cochlear duct or scala media (containing endolymph) a region of high potassium ion concentration that the stereocilia of the hair cells project into • The helicotrema, the location where the tympanic duct and the vestibular duct merge, at the apex of the cochlea • Reissner's membrane, which separates the vestibular duct from the cochlear duct • The basilar membrane, a main structural element that separates the cochlear duct from the tympanic duct and determines the mechanical wave propagation properties of the cochlear partition • The Organ of Corti, the sensory epithelium, a cellular layer on the basilar membrane, in which sensory hair cells are powered by the potential difference between the perilymph and the endolymph • hair cells, sensory cells in the Organ of Corti, topped with hair-like structures called stereocilia.
- 8. Contd… VESTIBUL E :- The vestibule is the central part of the bony labyrinth in the inner ear, and is situated behind the cochlea, and in front of the three semicircular canals. it measures about 5 mm from front to back, the same from top to bottom, and about 3 mm across. There are two sets of end organs in the inner ear, or labyrinth semicircular canals, which respond to rotational movements (angular acceleration); and the utricle and saccule within the vestibule, which respond to changes in the position of the head with respect to gravity (linear acceleration).
- 9. Contd…. SEMICIRCULAR CANAL :- The semicircular canals are a component of the bony labyrinth. The superior and posterior semicircular canals are oriented vertically at right angles to each other. The lateral semicircular canal is about a 30-degree angle from the horizontal plane. The horizontal canal detects angular acceleration of the head when the head is turned and the superior and posterior canals detect vertical head movements when the head is moved up or down. The lateral or horizontal canal (external semicircular canal) is the shortest of the three canals. The lateral or horizontal canal measures from 12 to 15 mm. for example, when you turn your head to the left and right- hand sides before crossing a road The superior or anterior semicircular canal is 15 to 20 mm in length. This occurs, for example, when nodding your head. The Posterior semicircular canal measuring from 18 to 22 mm. This occurs, for example, when you move your head to touch your shoulders, or when doing a cartwheel.
- 10. Auditory pathway The fibers of audotory pathway pass through cochlear nerve division of CNVIII. The major part of auditory pathway lies in M.O, mid brain and thalamic region. The higher centre for hearing is in temporal Lobe of cerebral cortex. The hair cell in organ of corti are the receptor Of auditory sensation. Auditory area are Area 41, 42 and wernicks area. Area 22 concerned with analysis and interpreta- lesion of auditory sensation along with wernicks.
- 12. DISORDER OF EAR OTITIS MEDIA DEFINITION :- Inflammation of middle ear due to blocked Eustachian tube. common causative organism are strep. Pneumoniae, hemophilus influenza and beta streptococcus hemolyticus. It may be suppurative ,serous or mucoid. Otitis media are a) acute suppurative otitis media b) chronic suppurative otitis media , and c) secretory otitis media. Infants and young children are predisposed to the development of acute otitis media because of the physiologic characteristics of the ear—the eustachian tube is shorter, wider, and straighter in children than in adults PREVENTION :- Feed infant in upright position, to prevent reflex. Maintain routine immunization. Encourage breast feeding for at least the first 6 mnth of life. Avoid exposure to tobacco smoke and allergence.
- 13. Contd…. RISK FACTORS 1. Age: increased incidence from 6 months to 20 months; decreases with age. 2. Upper respiratory tract infection. 3. Allergies, asthma. 4. Increased incidence in infants who are exposed to passive cigarette smoke. 5. Feeding bottle to infant/toddler in the supine position. CLINICAL MANIFESTATIONS 1. Otalgia (pain from pressure in the middle ear). a. Infants are irritable; may pull at their ears; sucking exacerbates pain. b. Young children verbally complain of severe ear pain. 2. Fever as high as 104° F is not uncommon with AOM. 3. Otoscopic examination. a. AOM—tympanic membrane is immobile, bright red, and bulging, with no light reflex and purulent effusion. b. OME—tympanic membrane is immobile, dull gray, and may have fluid behind it.
- 14. Contd…. 4. Postauricular and cervical lymph node enlargement. 5. If tympanic membrane ruptures, purulent drainage or blood may be present in the outer ear; pain will decrease temporarily (AOM and OME). 6. Conductive hearing loss may occur with recurrent rupture. 7. Speech and language development may be delayed. STAGES OF AOM :- STAGE PATHOLOGY SYMPTOMS SIGN 1 TUBAL OCCLUSION 2 PRESUPPURATION • Edema and hyperemia of nasopharyngeal end of tube. • Retraction of T.M • TM congestion • pyogenic organism invade tympanic cavity • inflammatory exudate in middle ear. • TM congested • Defness and ear ache • ear ache • throbbing • disturbed sleep • adult- defness and tinnitus •Child - fever • Conductive defness • Cartwheel appearance of TM • Congestion of pars tensa • Conductive defness
- 15. Contd…. STAGES PATHOLOGY SYMPTOMS SIGN 3. SUPPURATION 4 RESOLUTION • pus in middle ear • TM bulge out • TM rupture • release of pus • subside of symptoms •Sever ear ache •Defness increases •Fever •Vomiting •Convulsion • ear ach releived • fever subside • TM large ,bulge, loss of land mark. • Tenderness over mastoid antrum • EAC contain blood tinged discharge • later become mucopurulant 5 COMLICATION • virulance of organism is high • resistance of host is poor • acute mastoiditis ( m/c in children ) • labyrinthitis • sub periosteal abcess ( m/c extra cranial complication) • facial paralysis • meningitis • brain abcess
- 16. Contd…. TREATMENT A Medications. 1. Antibiotics, analgesics, antipyretics. 2. Ear drops (antibiotic and steroid combination). 3. Decongestants and antihistamines. 4. Corticosteroids for eustachian tube edema as needed. 5. OME does not require antibiotic therapy. B Surgical—myringotomy: drainage of the middle ear with insertion of tubes or grommets (or tympanostomy myringotomy) to relieve pressure and promote healing; used for recurrent cases that do not respond to medication; tubes are also known as pressure equalizing tubes (PE tubes or myringotomy tubes). NURSING PRIORITY • Teach the parents to administer the full course of the antibiotic.
- 17. Contd…. NURSING INTERVENTIONS Goal: • To enable parents of clients to describe problem, handle medication schedule, and cope with home care. • Recurrent infections cause an increased risk for permanent hearing loss or mastoiditis with potential intracranial spread of infection. • Antibiotics should be continued until all prescribed medication is taken, even after all symptoms are relieved. • Administer acetaminophen or ibuprofen for pain and fever. There should be relief of symptoms within 24 to 72 hours; if not, the health care provider should be contacted. • Pain-relieving ear drops (Auralgan, Pramotic) should be used only when there is no tympanostomy tube or rupture of the tympanic membrane. NURSING PRIORITY Aspirin should not be used for fever or pain in children 18 years of age or younger. • Control allergies and upper respiratory congestion.
- 18. Contd…. • The child should be discouraged from forcefully blowing his or her nose or holding his or her nose closed when sneezing. • Decrease risk for recurrence by preventing fluids from pooling around eustachian tube. 1. Hold or elevate infant’s head while feeding. 2. Do not prop bottle or allow infant to fall asleep with a bottle. 3. Encourage intake of water before sleeping. Goal: • Care for child after placement of tympanostomy tubes (myringotomy tubes or grommets). • Do not allow any water to get into the child’s ears; use of earplugs is currently controversial. • Assure parents that if the ear grommet or tube falls out, it is not a significant problem.
- 19. HEARING LOSS DEFINITION :- Hearing loss results from an impairment of the transmission of sound waves. TYPES :- Conductive hearing loss – absence of conduction through outer or middle ear Sensorineural hearing loss – due to damage of inner ear Mixed hearing loss – include both CHL and SNHL Central hearing loss – due to problem in brain RISK FACTOR :- • A Risk factors. • 1. Prolonged exposure to high-intensity sound waves. • 2. Repeated, chronic ear infections. • 3. Prenatal problems of rubella and eclampsia. • 4. Ototoxic medications: aminoglycosides, diuretics. • 5. Female with family history of otosclerosis.
- 20. Contd…. CONDUCTIVE HEARING LOSS SENSORINEURAL HEARING LOSS 1. Due to damage of outer or middle ear. Due to damage of inner ear. 2. Reduction in sound level Reduction in sound level, affect speech understanding or ability to hear clearly 3. Can be corrected through medicine or surgery Cannot be corrected medically , it is permanent 4. Cause :- Tumors, otosclerosis, inflammation or obstruction of external or middle ear. Cause :- Inner damage, viii CN damage, medicine, long exposure of loud sound, Sx, DM etc 5. Rinne test negative Positive 6. Weber test lateralization to sick ear Lateralization to healthy ear 7. Schwabach test elongated Shortest 8. Absolute bone conduction is normal Decreased 9. Hearing aids is Tx Chochlear implant is Tx
- 21. Contd…. Treatment A Speech therapy. B Sign language. C Stapedectomy for otosclerotic lesions. D Cochlear implants for profound sensorineural hearing loss. Nursing interventions To promote communication and socialization of the hearing-impaired Client. A Teach client how to care for hearing aid. B Teach client how to remove ear wax if impacted cerumen is a problem; may need an ear irrigation OLDER ADULT CARE FOCUS Hearing Aid Care • Keep the hearing aid dry; do not wear it while bathing or swimming. • Avoid using hair spray, cosmetics, or oils around the ear. • Clean hearing aid with soft cloth and recommended cleanser; do not immerse in water. • At night turn it off and open the battery compartment to prevent draining the battery. • Avoid exposing it to extreme temperatures (e.g., leaving it on a window ledge in the sunlight)
- 22. Contd…. • When cleaning the hearing aid, use a toothpick or pipe cleaner to remove any debris or cerumen from the hole in the middle part of the device that goes in the ear. • If the hearing aid does not work, change the battery or check the on/off switch; check the connection between the ear mold and receiver; clean it using the steps described above, or take it to an authorized hearing aid service center. • Keep extra batteries on hand for the hearing aid. Goal: To prevent complications after stapedectomy. A Assess client for dizziness, nausea, and vomiting. B Teach client to avoid sudden movement to prevent dizziness. C Maintain safety measures. D Instruct client that hearing may not improve until edema subsides in the operative area. ALERT • Hearing loss is very common in older adult clients. Watch for questions about hearing loss to be incorporated into test situations pertaining to other chronic health care problems.
- 23. OTOSCLEROSIS DEFINITION :- Fixation of stapes preventing transmission of sound waves to the inner ear; cause unknown. it is a disease of bony labyrinth. TYPES :- a) Stapedial b) chochlear c) histological ASSESSMENT FINDINGS 1. Progressive hearing loss 2. Tinnitus 3. Vertigo 4. Soft speech, well modulated and monotonous INTERVENTIONS: stapedectomy • 1. Stapedectomy: removal of diseased portion of stapes and replacement with a prosthesis; usually performed under local anesthesia. .Postoperative care a. Elevate side rails and assist client when out of bed to prevent injury; client may be dizzy. b. Explain to the client that hearing may improve during surgery and then decrease due to edema and packing.
- 24. Contd…. c. Check dressings frequently and report excessive drainage or bleeding. d. Administer medications as ordered: antibiotics, antiemetics, anti–motion sickness drugs. e. Assess facial nerve function; ask client to wrinkle forehead, close eyelids, puff out cheeks, smile, and show teeth; report if not the same on both sides. f. Report pain, headache, or vertigo to physician. g. Teach client not to blow nose or cough and to sneeze with mouth open. h. Teach client not to shampoo until physician gives approval because ear should be kept dry. i. Explain to the client that air travel is not allowed for six months. j. Place cotton ball in meatus after packing is removed ;change twice a day. Note :- Treatment of choice is stepedotomy. It is an autosomal dominant disorder. otoscopy shows flamingo pink bluish TM k/a schwartze’s sign.
- 25. BALANCING DISORDER The vestibular system of the inner ear maintains balance and coordination. A Disorders. 1. Ménière’s disease: an inner ear disorder caused by excess endolymph in the vestibular and semicircular canals; also known as endolymphatic hydrops. 2. Labyrinthitis: an inflammation of the cochlear and/or vestibular portion of the inner ear. Assessment A Diagnostics 1. Results of Weber test and auditory testing may indicate hearing loss. 2. Romberg test. B Clinical manifestations. 1. Vertigo: a sense of moving or spinning that is usually stimulated by sudden movement of the head; may occur when lying down. 2. Sudden, severe paroxysmal episodes of vertigo (Ménière’s disease). a. Severe nausea, vomiting.
- 26. Contd…. a. Severe nausea, vomiting. b. Nystagmus. c. Loss of balance. d. No pain or loss of consciousness. 3. Fluctuating hearing loss and tinnitus (Ménière’s disease). 4. Client may have no symptoms between attacks. 5. Manifestations become less severe with time. 6. Hearing loss increases with each attack (Ménière’s). Treatment A Medications (Ménière’s disease). 1. Atropine may stop an acute attack. 2. Sedatives. 3. Antihistamines, anticholinergics, calcium channel blockers. 4. Diuretics (to decrease endolymph fluid). 5. Meclizine hydrochloride (Antivert) for prevention and treatment of “motion sickness” 6. Antiemetics. B Diet: low-sodium.
- 27. Contd…. Nursing interventions Goal: To provide emotional and physical support during an acute attack. Maintain bed rest in a quiet, dimly lit room; avoid flickering lights and television. Secure a position of comfort. Avoid unnecessary nursing procedures. Minimize stimulation and sudden position changes. If client is severely nauseated, administer medications parenterally. Maintain safety: instruct client to always call before getting out of bed. Rise and change positions (especially the head) slowly. NURSING PRIORITY As a safety precaution, instruct the client to lie down immediately if an attack feels imminent.
- 28. Ear irrigation Common solutions :- Warm tap water or normal saline solution • Before irrigation, visually inspect the external ear canal with an otoscope to ensure that tympanic membrane is intact and that the auditory canal is not obstructed by a foreign body. • Do not irrigate an ear with otitis media present. • Temperature of irrigating solution should be near body temperature (37° C, approximately 98° F). If the solution is too cold or hot, dizziness and/or nausea may occur. • Cerumen may be softened by adding a few drops of warm mineral oil or an OTC preparation. • A rubber bulb syringe or a water pressure device may be used. • Straighten the ear canal by either pulling the outer ear up for adults or down for children under 3 years of age. • Direct water flow toward the top of the ear canal to create a circular motion, but never on the eardrum itself. • Do not forcefully push fluid into the ear canal, because this may rupture the eardrum. If severe pain, nausea, vomiting, or dizziness develops, stop the irrigation immediately. • Position the client to allow drainage of solution from the ear after irrigation.
- 29. Test RINNE TEST :- is a hearing test, primarily for evaluating loss of hearing in one ear (unilateral hearing loss). It compares perception of sounds transmitted by air conduction to those transmitted by bone conduction through the mastoid. Thus, one can quickly screen for the presence of conductive hearing loss. PROCEDURE :- The Rinne test and weber test performed by placing a 512 Hz. • The doctor strikes a tuning fork and places it on the mastoid bone behind one ear. • When you can no longer hear the sound, you signal to the doctor. • Then, the doctor moves the tuning fork next to your ear canal. • When you can no longer hear that sound, you once again signal the doctor. • The doctor records the length of time you hear each sound. RESULT :- NORMAL = AC>BC CONDUCTING HEARING LOSS = BC>AC SENSORINEURAL HEARING LOSS = AC > BC
- 30. Contd…. WEBER TEST :- A Weber test is another way to evaluate conductive and sensorineural hearing losses. PROCEDURE :- • The doctor strikes a tuning fork and places it on the middle of your head. • You note where the sound is best heard: the left ear, the right ear, or both equally. RESULT • Normal hearing will produce equal sound in both ears. • Conductive loss will cause the sound to be heard best in the abnormal ear. • Sensorineural loss will cause the sound to be heard best in the normal ear.