
Recommended
Recommended
More Related Content
Similar to TTHIS IS LECTURER COMMENT FOR MODULE 5 ASSIGNMENT.Slide 2 The.docx
Similar to TTHIS IS LECTURER COMMENT FOR MODULE 5 ASSIGNMENT.Slide 2 The.docx (20)
More from juliennehar
More from juliennehar (20)
Recently uploaded
Recently uploaded (20)
TTHIS IS LECTURER COMMENT FOR MODULE 5 ASSIGNMENT.Slide 2 The.docx
- 1. TTHIS IS LECTURER COMMENT FOR MODULE 5 ASSIGNMENT. Slide 2: There is a typo in the notes page. The info on the slide is repeated in the notes page. Slide 3: There are grammatical errors. Slide 8: The article title in the reference list should be formatted like a sentence, only the first word should start with a capital letter. See Section 6.29 on page 185 of the APA manual. Describe the current problem or opportunity for change. The problem is not identified. What is the current problem? Include in this description the circumstances surrounding the need for change, the scope of the issue, the stakeholders involved, and the risks associated with change implementation in general. Who are the stakeholders and what are the risks? Identify an evidence-based idea for a change in practice. What is your plan for knowledge transfer of this change, dissemination, and organizational adoption and implementation? This is not included in the slides. · Describe the measurable outcomes you hope to achieve with the implementation of this evidence-based change. I do not see outcomes identified. The tables are not mentioned. Each study is summarized in one or two slides. There is no synthesis of the knowledge to determine interventions to implement. Some of the information from the tables is copied onto the slides, but there is no clearly identified knowledge gained from each table. Talk about the studies as a whole. Look at all the outcomes across the table-what do you know about all the studies? Look at all of the results across the table-what do you know? What level of evidence were the studies? All level1? Based on the tables what can be implemented? There is a title slide and two slides with introduction. After that there are about 1-2 slides per study, making a summary. No
- 2. conclusions are drawn. No discussion of dissemination. There is no reference list. It's harder to put bubbles on the slides so most comments are here. Let me know if there are questions. Describe the current problem or opportunity for change. The problem is not identified. What is the current problem? Include in this description the circumstances surrounding the need for change, the scope of the issue, the stakeholders involved, and the risks associated with change implementation in general. Who are the stakeholders and what are the risks? Identify an evidence-based idea for a change in practice. What is your plan for knowledge transfer of this change, dissemination, and organizational adoption and implementation? This is not included in the slides. · Describe the measurable outcomes you hope to achieve with the implementation of this evidence-based change. I do not see outcomes identified. The tables are not mentioned. Each study is summarized in one or two slides. There is no synthesis of the knowledge to determine interventions to implement. Some of the information from the tables is copied onto the slides, but there is no clearly identified knowledge gained from each table. Talk about the studies as a whole. Look at all the outcomes across the table-what do you know about all the studies? Look at all of the results across the table-what do you know? What level of evidence were the studies? All level1? Based on the tables what can be implemented? High Speed Response Teams for Patients. Name Institutional Affiliation Date
- 3. High speed response teams for patients is also known as the medical emergency team (MET). is also known as the high acuity response team (HART). It is a team of healthcare providers responsible for responding to the hospitalized clients. The targeted patients using this kind of response are those with early signs of deterioration. Introduction High speed response teams for patients is also known as the medical emergency team (MET). It is also refered to as the high acuity response team (HART). This is a team of healthcare providers who are responsible for responding to the hospitalized clients. The targeted patients using this kind of response are those with early signs of deterioration. 2 The patients are on non-intensive care units. The response it used to assists in the prevention of respiratory or cardiac arrest. This paper therefore aims at discussing the information provided by four articles on the topic related to high speed response Team for Patients
- 4. Cont’d These patients are on non-intensive care units. It is used to help in the prevention of respiratory or cardiac arrest. This paper therefore aims at discussing the information provided by four articles on the topic related to high speed response Team for Patients 3 Objective: to assess the impacts of delayed response by the rapid response team. The impact being assessed was related to the number of reported deaths, cardiac arrest, and the rates of intensive care transfer. Methods used: the review involved both randomized and non- randomized research works. Xu, M. K., Dobson, K. G., Thabane, L., & Fox-Robichaud, A. (2018). Evaluating the effect of delayed activation of rapid response teams on patient outcomes: a systematic review protocol. Systematic Reviews, 7 (1), 42. The main objective of the authors of this article was to assess the impacts of delayed response by the rapid response team. The impact being assessed was related to the number of reported deaths, cardiac arrest, and the rates of intensive care transfer. According to his article a review involving both randomized and non-randomized research works was adopted. 4
- 5. Rapid response team have been widely adopted in the global healthcare sector. They are helping in the detection and reaction to the deterioration of the patient population. Lack of evidence regarding their effectiveness is brought by the absent of standardized strategy regarding their use and implementation. Cont’d Authors states that rapid response team have been widely adopted in the entire world within the healthcare sector. Rapid response Team are helping in the detection and reaction to the deterioration of the patient population. There is lack of evidence regarding their effectiveness due to absent of standardized strategy regarding their use and implementation. 5 Objective: to assess whether the intervention which involves crew resource management training of the team leaders helps in the improvement of performance. Method: in situ observation of the Rapid Response Team activation. The dynamic of the performance from the team were measured through observation adherence to the ideal task and use of the Team Emergency Assessment Measure Tool. Siems, A., Cartron, A., Watson, A., McCarter, R., & Levin, A. (2017). Improving pediatric rapid response team performance through crew resource management training of team leaders. Hospital pediatrics, 7 (2), 88-95.
- 6. The study was aimed at assessing whether the intervention which involves crew resource management training of the team leaders helps in the improvement of performance. The method used by the authors were the in situ observation of the Rapid Response Team activation. The dynamic of the performance from the team were measured through observation adherence to the ideal task and use of the Team Emergency Assessment Measure Tool. 6 Response Team are helping in the improvement of the means of detection and responses to the deteriorating patients. The outcome of this study shows that the use of the targeted crew resources management of the team leaders is crucial It helps in increasing the team performance as well as the dynamics of the patients who needs transfer to the intensive care units. The trained team leaders helps in the improvement of the behaviors of the Rapid Response team members who are not trained. Cont’d According to this study, Rapid Response Team are helping in the improvement of the means of detection and responses to the deteriorating patients. The outcome of this study shows the use of the targeted crew resources management of the team leaders
- 7. is helping in increasing in the team performance as well as the dynamics of the patients who needs transfer to the intensive care units. The trained team leaders helps in the improvement of the behaviors of the Rapid Response team members who are not trained. 7 Obective: to quantitatively give a description of the effects of the High Speed Response Team at 944 bed within the university affiliated healthcare facility. Method: open-ended interviews using 49 questions were used Positive outcomes: improvement in the morale of nurses and the real time distribution of the workload for nurses. Negative impacts: increased tensions between nurses and physicians, burden to the response team, and reduction in the autonomy of the trainees. High speed response team offer benefits related to the reduction in the rates of transfers to the ICU. Benin, A. L., Borgstrom, C. P., Jeng, G. Y., Roumanis, S. A., & Horwitz, L. I. (2012). Defining Impact of a Rapid Response Team: Qualitative Study with Nurses, Physicians, and Hospital Administrators. Postgraduate Medical Journal, 88 (1044), 575- 582. Authors of this study aimed at quantitatively give a description of the effects of the High Speed Response Team at 944 bed within the unversity affiliated healthcare facility. Open-ended interviews using 49 questions were used for the administrators, physicians, trainees, and the Rapid Response Team specialists, nurses, and the respiratory technicians. The outcomes of the
- 8. study revealed a positive related to the improvement in the morale of nurses and the real time distribution of the workload for nurses. The negative impacts included increased tensions between nurses and physicians, burden to the response team, and reduction in the autonomy of the trainees. It was clear that high speed response team offer benefits related to the reduction in the rates of transfers to the ICU. 8 Objective: to determine the prolonged impact of the rapid response team implementation on the failure to rescue. Method: longitudinal research work on the performance of the institution through using control charts and Bayesian Charge Point (BCP) assessment. Setting: academic healthcare facility in the Midwest, USA. Moriarty, J. P., Schiebel, N. E., Johnson, M. G., Jensen, J. B., Caples, S. M., Morlan, B. W., et al. (2014). Evaluating implementation of a rapid response team: considering alternative outcome measures. International Journal for Quality in Health Care, 26 (1), 49-57. Authors of this article aimed at determining the prolonged impact of the rapid response team implementation on the failure to rescue. Authors of this study employed longitudinal research work on the performance of the institution through using control charts and Bayesian Charge Point (BCP) assessment. The study was performed at academic healthcare facility in the Midwest, USA. 9
- 9. There was a reduction in the failure to rescue. There was an increase in the unanticipated rate of the intensive care unit transfers. There was a greater reduction in the mortality amongst non- intensive care unit discharges in the control charts. Cont The outcome of the study reveal about a reduction in the failure to rescue. There was an increase in the unanticipated rate of the intensive care unit transfers. There was a greater reduction in the mortality amongst non-intensive care unit discharges in the control charts. 10 Sustaining Evidence-Based Practice Through Organizational Policies and an Innovative Model The team adopts the Advancing Research and Clinical Practice Through Close Collaboration model. This is the 12th and last article in a series from the Arizona State University College of Nursing and Health Innovation’s Center for the Advancement of Evidence-Based Practice. Evidence-based practice (EBP) is a problem-solving approach to the delivery of health care that integrates the best evidence from studies and patient care data with clinician expertise and patient preferences and values. When it’s delivered in a context of caring and in a supportive organizational culture, the
- 10. highest quality of care and best patient outcomes can be achieved. The complete EBP series is available as a collection on our Web site; go to www.ajnonline.com and click on Collections. In July’s evidence-based prac-tice (EBP) article, Rebecca R., Carlos A., and Chen M. eval- uated the outcomes of their rapid response team (RRT) implemen- tation project. Their findings in- dicated that a significant decrease in one outcome, code rates outside the ICU, had occurred after im- plementation of the RRT. This promising finding, together with many other considerations—such as organizational readiness; clini- cian willingness; and a judicious weighing of all the costs, benefits, and outcomes—encouraged the EBP team to continue with plans to roll out the RRT protocol throughout the entire hospital system. They also began to work on presentations and publications about the project so that others could learn from their experience and implement similar interven- tions to improve patient outcomes. USING EVIDENCE TO INFORM ORGANIZATIONAL POLICY Because Rebecca, Carlos, and Chen are concerned about whether the implementation of an RRT can be sustained over time in their hospi-
- 11. tal, they want to take the neces- sary steps to create a hospital- wide RRT policy. Therefore, they make an appointment with their hospi- tal’s director of policies and pro- cedures, Maria P., to share the outcomes data they’ve gathered from their project and to discuss the project’s success so far. Maria is impressed by the rigor of the team’s sequential EBP process and the systematic way in which they’ve gathered the outcomes data. She reminds them that the measurement of outcomes (inter- nal evidence) plus rigorous re- search (external evidence) result in the best evidence-based orga- nizational policies to guide the high est quality of care in health care institutions. Maria volunteers to assist the team in writing a new evidence- based policy to support having an RRT in their hospital. She suggests that each recommendation in the policy be supported by evidence. Maria explains that once the pol- icy is written, it needs to be ap- proved by the hospital-wide policy committee, representing all of the health disciplines. Maria empha-
- 12. sizes that transdisciplinary health care professionals and administra - tors should routinely be involved when planning and implementing evidenced-based organizational policies. She also reminds the EBP team that translating evidence and evidence-based organizational pol- icies into sustainable routine clin- ical practices remains a major challenge for health care systems. The new RRT policy written by Rebecca, Carlos, and Chen with Maria’s help is approved by the hospital-wide policy committee within three months. Now the By Bernadette Mazurek Melnyk, PhD, RN, CPNP/PMHNP, FNAP, FAAN, Ellen Fineout-Overholt, PhD, RN, FNAP, FAAN, Lynn Gallagher- Ford, MSN, RN, NE-BC, and Susan B. Stillwell, DNP, RN, CNE, ANEF [email protected] AJN ▼ September 2011 ▼ Vol. 111, No. 9 57 It only takes one passionate, committed person to spearhead a team vision to improve care for patients and their families.
- 13. http://www.ajnonline.com challenge for the team is to work with clinicians across the hospital system to implement it. The EBP team schedules a series of presen- tations throughout the hospital to introduce the new RRT policy. They rotate the days and times of this in-service to capture as many direct care clinicians as possible. To ensure that all clinicians are educated on the new policy, a da- tabase is created to track in-ser- vice attendees, and each hos pital unit is asked to appoint a volun- teer to deliver the presentation to any clinicians who missed it. Post- ers are created and buttons de- signed as visual triggers to remind staff to implement the new policy. Throughout this process, the EBP team learned that dissemi- nation of evidence alone doesn’t typ ically lead clinicians to make a sustainable change to EBP, and they were impressed by how im- portant it was to have unit-based champions reinforce the new pol- icy.1 They also learned that it’s critical to have an organizational culture that supports EBP (such as evidence-based decision making
- 14. in tegrated into performance ex- pectations, up-to-date resources and tools, ongoing EBP knowledge and skills-building workshops, and EBP mentors at the point of care) in order for clinicians to con- sistently deliver evidence-based care.2 Since the process they followed worked so well, the team believes that their hospital needs to adopt a model to guide and reinforce the creation of a culture to sus- tain the EBP approach they had initiated through this project. They review several EBP process and system integration models and decide to adopt the Advanc- ing Research and Clinical Prac- tice Through Close Collaboration (ARCC) model because its key strategy to sustain evidence-based care is the presence of an EBP mentor (a clinician with advanced knowledge of EBP, mentorship, and individual as well as organi- zational change). With Carlos’s success as an expert EBP mentor, and the mentorship model work- ing so well, they believe that de- veloping a cadre of EBP mentors system-wide is key to the ongoing 58 AJN ▼ September 2011 ▼ Vol. 111, No. 9 ajnonline.com
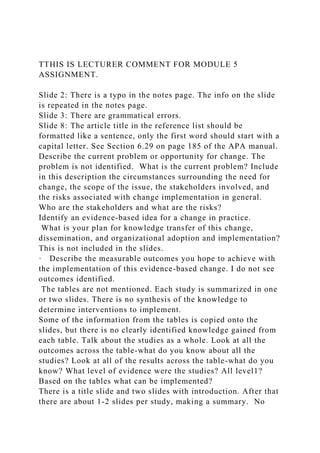
- 15. Potential Strengths Philosophy of EBP (paradigm is system-wide) Presence of EBP mentors and champions Administrative support Clinicians’ beliefs about the value of EBP and ability to implement the EBP processa Identification of strengths and major barriers to EBP implementation EBP implementationa, b Decreased hospital costs Potential Barriers Lack of EBP mentors and champions
- 16. Inadequate EBP knowledge and skills Lack of EBP valuing Implementation of ARCC strategies Interactive EBP skills building EBP rounds and journal clubs Improved patient outcomes Nurse/clinician satisfaction Cohesion Intent to leave Turnover Development and use of EBP mentors
- 17. Assessment of organizational culture and readiness for EBP a Figure 1. The ARCC Model for System-Wide Implementation and Sustainability of EBP ARCC = Advancing Research and Clinical Practice Through Close Collaboration; EBP = evidence-based practice. a Scale developed. b Based on the EBP paradigm and using the EBP process. © 2 00 5, M el ny k an d Fi
- 18. ne ou t-O ve rh ol t. that this model be adopted, not only for the nursing department, but for all disciplines throughout the organization. THE EBP JOURNEY HAS JUST BEGUN This series presented a case in- volving a hypothetical medical– surgical nurse and her colleagues to illustrate how EBP can be suc- cessfully implemented to improve key patient outcomes. It’s impor- tant that the process start with an ongoing spirit of inquiry, and that nurses always question the evidence behind the care we pro- vide and never settle for the sta- tus quo. Never forget that it only takes one passionate, committed person to spearhead a team vi- sion to improve care for patients and their families. It also takes
- 19. persistence through the “charac- ter builders” that are sure to appear as the vision comes to fruition. Although the EBP team has successfully completed their RRT implementation project and its incorporation as a hospital-wide policy, their EBP journey has just be gun. In fact, only days after the project’s completion, Rebecca asked Carlos another great PICOT question: “In critically ill patients, how does early ambulation com- pared with delayed ambulation affect ventilator-associated pneu- monia in the ICU?” Carlos looked at her and replied, as a great men - tor does, “I will help you search for the evidence and we will find and organizational culture change. These individuals, whether expert system-wide mentors, advanced practice mentors, or peer mentors, are focused on helping point-of- care clinicians to use and sustain EBP and to conduct EBP imple- mentation, quality improvement, and outcomes management proj- ects. When clinicians work with EBP mentors, their beliefs about the value of EBP and their ability to implement it increase, and this is followed by a greater achieve-
- 20. ment of evidence-based care.4 The ARCC model contends that greater implementation of EBP results in higher job satisfaction, lower turnover rate, and better patient outcomes. A series of studies now support the empiri- cal relationships in the ARCC model.4-8 The ARCC model has been and continues to be implemented in hospitals and health care sys- tems across the country with ex- cellent results in quality of care and patient outcomes. Valid and reli- able instruments, such as the EBP Beliefs and EBP Implementation scales,6 are used to measure key constructs in the model and, to- gether with organizational culture and readiness for EBP, help to de- termine the model’s effectiveness.6 The EBP team discusses how all the elements of the ARCC model are an excellent fit for their organization. They decide to make a recommendation to the Shared Governance Steering Committee implementation and sustainabil- ity of EBP in their organization. SUSTAINING AN EBP CULTURE WITH THE
- 21. ARCC MODEL In reviewing the ARCC model, the EBP team finds that its aim is to provide hospitals and health care systems with an organized conceptual framework to guide system-wide implementation and sustainability of EBP for the pur- pose of improving quality of care and patient outcomes. In addition, this model can be used to achieve a “high reliability” organization (one that delivers safe and high- quality care), decrease costs, and improve clinicians’ job satisfaction. Four assumptions are basic to the ARCC model3: • Both barriers to and facilitators of EBP exist for individuals and within health care systems. • Barriers to EBP must be re- moved or mitigated and facili- tators put in place in order for individuals and health care sys - tems to implement EBP as a standard of care. • For clinicians to change their practices to be evidence based, both their beliefs about the value of EBP and their confi- dence in their ability to imple- ment it must be strengthened.
- 22. • An EBP culture that includes EBP mentors is necessary in order to advance and sustain EBP in individuals and health care systems. The first step in the ARCC model is to assess the organiza- tion’s culture and readiness for EBP (see Figure 1). From that assess- ment, the strengths and limita tions of implementing EBP within the organization can be identified. The key implementation strategy in the ARCC model is the development of a cadre of EBP mentors, who are typically advanced practice nurses or clinicians with in-depth knowledge of and skills in EBP and in individual behavior change [email protected] AJN ▼ September 2011 ▼ Vol. 111, No. 9 59 Developing a cadre of EBP mentors system-wide is key to the ongoing implementation and sustainability of EBP in an organization. Wiley-Blackwell; Sigma Theta Tau; 2010. p. 169-84.
- 23. 4. Melnyk BM, et al. Nurses’ perceived knowledge, beliefs, skills, and needs regarding evidence-based practice: im - plications for accelerating the para- digm shift. Worldviews Evid Based Nurs 2004;1(3):185-93. 5. Levin RF, et al. Fostering evidence- based practice to improve nurse and cost outcomes in a community health setting: a pilot test of the advancing research and clinical practice through close collaboration model. Nurs Adm Q 2011;35(1):21-33. 6. Melnyk BM, et al. The evidence- based practice beliefs and implemen- tation scales: psychometric properties of two new instruments. Worldviews Evid Based Nurs 2008;5(4):208-16. 7. Melnyk BM, et al. Correlates among cognitive beliefs, EBP implementa- tion, organizational culture, cohesion and job satisfaction in evidence-based practice mentors from a community hospital system. Nurs Outlook 2010; 58(6):301-8. 8. Wallen GR, et al. Implementing evidence-based practice: effectiveness of a struc tured multifaceted mentor- ship programme. J Adv Nurs 2010; 66(12):2761-71. Practice. Contact author: Berna dette
- 24. Mazurek Melnyk, [email protected] The authors have disclosed no potential conflicts of inter est, financial or other- wise. REFERENCES 1. Melnyk BM, Wiliamson KM. Using evidence-based practice to enhance organizational policies, healthcare qual - ity, and patient outcomes. In: Hinshaw AS, Grady PA, editors. Shaping health policy through nursing research. New York: Springer Publishing Company; 2011. p. 87-98. 2. Melnyk BM, Fineout-Overholt E. Evidence-based practice in nursing and healthcare: a guide to best prac- tice. Philadelphia: Wolters Kluwer Health/Lippincott Williams and Wil- kins; 2011. 3. Melnyk BM, Fineout-Overholt E. ARCC (Advancing Research and Clini- cal prac tice through close Collabora- tion): a model for system-wide implementation and sustainability of evidence-based practice. In: Rycroft- Malone J, Bucknall T, editors. Models and frame works for implementing evidence-based practice: linking evi- dence to action. Oxford; Ames, IA: the answer to your question— because EBP, not practices steeped
- 25. in tradition, is the only way we do it here!” ▼ Bernadette Mazurek Melnyk is associate vice president for health promotion, uni- versity chief wellness officer, and dean of The Ohio State University College of Nurs - ing in Columbus, where Lynn Gallagher- Ford is director of Transdisciplinary Evidence-Based Practice and Clinical Innovation. Ellen Fineout-Overholt is dean of Professional Studies and chair of the Department of Nursing at East Texas Baptist University in Mar shall, TX. Susan B. Stillwell is clinical professor and associate director of the Center for the Advancement of Evidence-Based Practice at Arizona State Univer sity in Phoenix. At the time this article was written, Ber- nadette Mazurek Melnyk was dean and distinguished foundation professor of nursing in the College of Nurs ing and Health Innovation at Arizona State Uni- versity, where Ellen Fineout-Overholt was clinical pro fessor and director, and Lynn Gallagher-Ford was clinical assistant pro- fessor and assistant director, of the Center for the Advancement of Evidence-Based Original Article A Test of the ARCC C© Model Improves Implementation of Evidence-Based Practice,
- 26. Healthcare Culture, and Patient Outcomes Bernadette Mazurek Melnyk, RN, PhD, CPNP/PMHNP, FAANP, FNAP, FAAN • Ellen Fineout-Overholt, RN, PhD, FNAP, FAAN • Martha Giggleman, RN, DNP, NEA-BC • Katie Choy, RN, DNP, CNS, NEA-BC Keywords ARCC, evidence-based practice, organizational culture, patient outcomes ABSTRACT Background: Although several models of evidence-based practice (EBP) exist, there is a paucity of studies that have been conducted to evaluate their implementation in healthcare settings. Aim: The purpose of this study was to examine the impact of the Advancing Research and Clinical practice through close Collaboration (ARCC) Model on organizational culture, clinicians’ EBP beliefs and EBP implementation, and patient outcomes at one healthcare system in the western United States. Design: A pre-test, post-test longitudinal pre-experimental study was conducted with follow-up immediately following full implementation of the ARCC Model.
- 27. Setting and Sample: The study was conducted at a 341-bed acute care hospital in the western region of the United States. The sample consisted of 58 interprofessional healthcare professionals. Methods: The ARCC Model was implemented in a sequential format over 12 months with the key strategy of preparing a critical mass of EBP mentors for the healthcare system. Healthcare professionals’ EBP beliefs, EBP implementation, and organizational culture were measured with valid and reliable instruments. Patient outcomes were collected in aggregate from the hospital’s medical records. Results: Findings indicated significant increases in clinicians’ EBP beliefs and EBP implementation along with positive movement toward an organizational EBP culture. Study findings also indicated substantial improvements in several patient outcomes. Linking Evidence to Action: Implementation of the ARCC Model in healthcare systems can en- hance clinicians’ beliefs and implementation of evidence-based care, improve patient outcomes, and move organizational culture toward EBP. INTRODUCTION AND BACKGROUND It is well known that evidence-based practice (EBP) improves healthcare quality, safety, and patient outcomes as well as fos- ters clinicians’ active engagement in their practices. Nurses who use an evidence-based approach to care and practice in cultures that support EBP are more empowered as they are able to make a difference in the care of their patients. Although the positive impact of EBP has been demonstrated through multiple studies, major barriers exist that prevent EBP from
- 28. becoming the standard of care throughout the world. These barriers include (a) inadequate EBP knowledge and skills of clinicians, (b) misperceptions that EBP takes too much time, (c) organizational culture and politics, (d) lack of support from nurse leaders and managers, and (e) inadequate resources and investment in EBP (Jun, Kovner, & Stimpfel, 2016; Melnyk et al., 2016; Melnyk, Fineout-Overholt, Gallagher-Ford, & Ka- plan, 2012). Aside from equipping clinicians with the knowl- edge and skills needed to attain the EBP competencies and con- sistently implement evidence-based care, findings from studies have indicated that clinician access to EBP mentors can play a key role in their implementation of EBP and the development of organizational cultures that support the delivery of evidence- based care (Fineout-Overholt & Melnyk, 2015; Melnyk, 2007). Although several EBP models exist, most are process mod- els that outline the steps of EBP or the sequence of conducting an EBP project. EBP process models include the Johns Hopkins Nursing Evidence-Based Practice Model (Dearholt & Dang, 2012), the Iowa Model of Evidence-Based Practice to Promote Quality Care (Titler et al., 2001), the Model for Evidence-Based Practice Change (Rosswurm & Larabee, 1999), and the ACE Star Model of Knowledge Transformation (Stevens, 2012). Unlike EBP process models, the Advancing Research and Worldviews on Evidence-Based Nursing, 2017; 14:1, 5–9. 5 C© 2016 Sigma Theta Tau International A Test of the ARCC C© Model Improves Implementation of Evidence-Based Practice Figure 1. The Advancing Research and Clinical Practice Through Close Collaboration (ARCC) Model.
- 29. Clinical practice through close Collaboration (ARCC) Model is a system-wide model to advance and sustain EBP in healthcare systems (see Figure 1). The first step in implementing the ARCC Model is an organizational assessment of the current EBP culture in order to identify strengths and major barriers to EBP in the healthcare system so that strategies can be implemented to remove those barriers. At the core of the ARCC Model is a critical mass of EBP mentors who, through intentional strategic initiatives, assist point of care clinicians in enhancing their beliefs about the value of EBP and their confidence in implementing it. As a result, ARCC contends that heightened EBP beliefs in clinicians result in greater implementation of evidence-based care, which ultimately leads to higher job satisfaction, less staff turnover, and improved patient outcomes. Several studies now support the relationships among key constructs in the ARCC Model (Levin, Fineout-Overholt, Melnyk, Barnes, & Vetter, 2011; Melnyk, 2012; Melnyk & Fineout-Overholt, 2002; Melnyk et al., 2004; Melnyk, Fineout-Overholt, & Mays, 2008; Melnyk, Fineout- Overholt, Giggleman, & Cruz, 2010; Wallen et al., 2010). AIM The purpose of this study was to examine the impact of the ARCC Model on organizational culture, clinicians’ EBP beliefs and EBP implementation, and patient outcomes at one health- care system in the western region of the United States. DESIGN A pre-test, post-test longitudinal pre-experimental study was conducted with follow-up immediately following full imple- mentation of the ARCC Model. Institutional Review Board ap- proval was obtained from the authors’ institution as well as the organization’s research subject review board. SETTING AND SAMPLE
- 30. This study was conducted at Washington Hospital Healthcare System, a 341-bed acute care hospital in the San Francisco bay area. The sample consisted of 58 interprofessional health- care professionals, with complete follow-up data for 45 partic- ipants. Participants were point of care nurses, administrators, nurse managers, clinical nurse specialists, respiratory thera- pists, occupational therapists, physical therapists, dieticians, social workers, and pharmacists. Although physician cham- pions participated in the projects, they were not part of the data collection. Only the project teams participated in data collection. METHODS The ARCC Model was implemented in a sequential format over 12 months with the key strategy of preparing a critical mass of EBP mentors for the healthcare system. Intensive EBP workshops were first provided to the 58 participants in order to enhance their knowledge and skills in the seven steps of 6 Worldviews on Evidence-Based Nursing, 2017; 14:1, 5–9. C© 2016 Sigma Theta Tau International Original Article Table 1. Examples of PICOT Questions Formulated by the EBP Teams � In ventilated intensive care unit patients (P), how does early ambulation (I) compared to routinely scheduled ambulation (C) affect length of stay and episodes of ventilator associated pneumonia while in the intensive care unit (T) � In congestive heart failure patients (P), how does comprehensive pre-discharge education (I) compared to standard pre-discharge education (C), affect readmission
- 31. rates to the hospital (O)? EBP. In addition, content and skills building in the workshops focused on how to facilitate individual behavior change of clin- icians to implement EBP and how to facilitate an EBP organi- zational culture. The 58 participants were divided into working teams of six to eight members who were to collaborate on an EBP change project to improve patient outcomes within the hospital. Each team was then charged with formulating a PICOT (Patient population, Intervention or Issue of inter- est, Comparison intervention or issue, Outcome, and Time for the intervention to achieve the outcome if relevant) question about an important clinical issue, systematically searching for the best evidence, and critically appraising and synthesizing the evidence culminating in a recommendation for practice. See Table 1 for examples of PICOT questions developed by the teams. Strategic plans were then developed by the inter- professional EBP mentor teams to implement and evaluate the impact of the EBP changes on clinical outcomes within their organization. After implementation and evaluation of the prac- tice changes were completed, the final step for the teams was to submit their projects for presentation at local, regional, or national conferences to disseminate their successes to others within the healthcare community. OUTCOMES Study variables were measured with the following valid and reli- able instruments. The Evidence-Based Practice Beliefs (EBPB) Scale Melnyk & Fineout-Overholt, 2003a) measured clinicians’ beliefs about EBP and their ability to implement it. The 16-item Likert scale has established face, content, and construct valid- ity with internal consistency reliabilities greater than .85 across multiple studies (Melnyk et al., 2008). Responses on the scale range from 1 (strongly disagree) to 5 (strongly agree). Examples of items on the scale include (a) I am clear about the steps in
- 32. EBP, (b) I am sure that I can implement EBP, and (c) I am sure that evidence-based guidelines can improve care. The Evidence-Based Practice Implementation (EBPI) Scale measured delivery of evidence-based care (Melnyk & Fineout- Overholt, 2003b). Participants respond to each of the 18 Likert scale items on the EBPI by answering how often in the last eight weeks they have performed certain EBP activities, such as (a) generated a PICOT question about my practice, (b) used evi- dence to change my clinical practice, (c) evaluated the outcomes of a practice change, and (d) shared the outcome data collected with colleagues. The EBPI has established face, content, and construct validity as well as internal consistency reliabilities greater than .85 across multiple studies (Melnyk et al., 2008). The Organizational Culture and Readiness Scale for System-Wide Integration of Evidence-Based Practice (OCR- SIEP) measured the organization’s culture and its readiness for system-wide EBP (Fineout-Overholt & Melnyk, 2006). This instrument contains 26 Likert scale items that identify a de- scription of the existing support in the current culture for EBP, which offers insight into the strengths and opportunities for fostering evidence-based care within a healthcare system. The OCRSIEP scale has established face and content validity along with excellent internal consistency reliability of greater than .85 across multiple samples (Melnyk & Fineout-Overholt, 2015). Examples of items on the OCRSIEP include the following: (a) To what extent is EBP clearly described as central to the mission and philosophy of your institution? (b) To what extent do you believe that EBP is practiced in your organization? And (c) To what extent is the nursing staff with whom you work committed to EBP? Patient Outcomes
- 33. Aggregate data were gathered by the teams, including data from the hospital’s medical records (e.g., number of cases of ventilator associated pneumonia, hospital readmission rates) before and after implementation of the ARCC Model to evaluate relevant patient outcomes as results of the EBP projects. Analyses T tests and effect sizes were calculated for study variables to evaluate pre-to-post differences. A p value of .05 was set for statistical significance. RESULTS Findings indicated that the clinicians’ EBP beliefs, EBP im- plementation, and movement of organizational culture toward EBP significantly increased over the 12-month project. Specif- ically, clinicians’ EBP beliefs (n = 45) increased significantly from baseline (M = 60.7, SD = 7.6) to follow-up (M = 64.9, SD = 6.7; t = 4.2; p = .00; effect size = .62, which is a medium to large positive effect for ARCC). EBP implementation also significantly increased from baseline (M = 17.8, SD = 10.3) to follow-up (M = 51.9, SD = 16.8; t = 12.9; p = .00; effect size = 2.3, indicating a large positive effect for ARCC). In addition, organizational culture and readiness for EBP increased signifi- cantly from baseline (M = 80.9; SD = 90.8) to follow-up (M = 90.8; SD = 14.7; t = 3.9; p = .00; effect size = .70, which is a medium to large positive effect for ARCC). In addition, as a result of implementing the ARCC Model, evidence-based interventions improved key patient outcomes (see Table 2). Worldviews on Evidence-Based Nursing, 2017; 14:1, 5–9. 7 C© 2016 Sigma Theta Tau International A Test of the ARCC C© Model Improves Implementation of Evidence-Based Practice
- 34. Table 2. Project Outcomes From Implementation of the EBP Changes � A practice change to early ambulation in the ICU led to a 2.7 reduction in ventilator days (11.6–8.9) and no ventilator associated pneumonia. � With the implementation of a pressure ulcer prevention nursing standardized procedure on a medical-surgical unit, the acquired pressure ulcer rate was significantly decreased from 6.07% to 0.62% 1 year later. � Comprehensive education of congestive heart failure patients led to a 14.7% reduction in hospital readmissions. � After implementation of family centered care on the pediatric unit, 75% of parents perceived the overall quality of care as excellent compared to 22% pre-implementation. � The percentage of mothers not supplementing their breast milk with formula increased from 61.7% to 71.1% after the evidence-based baby friendly hospital initiative was implemented. � After implementation of a nurse-initiated pain protocol in the emergency room (ER), wait time for pain medication decreased from 46 minutes to 13 minutes and length of stay in the ER also decreased from 120 minutes to 91 minutes. DISCUSSION Findings support the positive impact of implementing the ARCC Model on clinicians’ EBP beliefs and a dramatic in- crease in EBP implementation in those who participated in the project. Organizational culture at the hospital shifted greatly toward system-wide EBP. Most important, as a result of imple-
- 35. menting ARCC, there were multiple improvements in patient outcomes. The establishment of a cadre of EBP mentors is cen- tral to building an organizational culture of EBP and im- plementing evidence-based care. The EBP mentors in this study garnered the knowledge and skills needed to successfully implement and evaluate EBP changes within the hospital as well as to work with their colleagues in creating an EBP culture in which to deliver high-quality evidence-based care. These findings affirm that culture eats strategy and assists clini- cians in making EBP the social norm within a system (Mel- nyk, 2016b). Without a culture and environment that supports EBP, high-quality evidence-based care will not sustain (Melnyk, 2016a). Numerous healthcare systems and hospitals throughout the United States and globe have implemented the ARCC Model in their efforts to build and sustain an EBP culture and environ- ment in their organizations. As a part of building this culture, position descriptions have been created or changed to include responsibilities as an EBP mentor. For example, at The Ohio State University Wexner Medical Center, the primary responsi- bility of the clinical nurse specialists throughout the healthcare system is to serve as EBP mentors for point of care staff in improving patient outcomes. Part of this role is ensuring compliance with the EBP competencies for advanced practice nurses (Melnyk, Gallagher-Ford, & Fineout-Overholt, 2016; Melnyk, Gallagher-Ford, Long & Fineout-Overholt, 2015). Research is needed to further confirm the advantages of using particular EBP models in real-world practice settings, including how implementation of these models impact both clinician, leader and patient outcomes (Dang et al., 2015). Com- parative effectiveness studies that evaluate the benefits of in-
- 36. dividual models as well as combining models also are needed. Those hospitals and systems who use an EBP model to guide implementation of evidence-based care should document their experiences and outcomes in order to better understand the model’s usefulness in facilitating EBP and share this impor- tant information with others who might use the model (Gra- ham, Tetroe, & KT Theories Research Group, 2007). Return on investment by including cost outcomes also should be eval- uated. WVN LINKING EVIDENCE TO ACTION � The ARCC Model is an evidence-based system- wide model for advancing the implementation and sustainability of EBP. � A key strategy in the ARCC model is the develop- ment of a critical mass of EBP mentors who assist point of care clinicians in the consistent imple- mentation of evidence-based care. � Use of ARCC EBP mentors enhances the EBP be- liefs and EBP implementation of clinicians and strengthens the EBP culture of an organization. � An organizational culture of EBP is central to sup- porting sustainable high quality evidence-based care. � Implementation of the ARCC Model can substan- tially improve patient outcomes. Author information Bernadette Mazurek Melnyk, Associate Vice President for Health Promotion, University Chief Wellness Officer, Dean
- 37. and Professor, College of Nursing, Professor of Pediatrics & Psychiatry, and College of Medicine, The Ohio State Univer- sity, Columbus, Ohio; Ellen Fineout-Overholt, Mary Coulter Dowdy Distinguished Professor of Nursing, College of Nurs- ing & Health Sciences University of Texas at Tyler, Tyler, Texas; Martha Giggleman, Healthcare Consultant & Advocate Liver- more, California; Katie Choy, Senior Director, Nursing Practice and Education, Washington Hospital Healthcare System, Fre- mont, California 8 Worldviews on Evidence-Based Nursing, 2017; 14:1, 5–9. C© 2016 Sigma Theta Tau International Original Article Address correspondence to Dr. Bernadette Mazurek Melnyk, The Ohio State University, 145 Newton Hall, 1585 Neil Avenue, Columbus, OH 43210; [email protected] Accepted 16 September 2016 Copyright C© 2017, Sigma Theta Tau International References Dang, D., Melnyk, B. M., Fineout-Overholt, E., Ciliska, D., Di- Censo, A., Cullen, L., . . . & Stevens, R. K. (2015). Models to guide implementation and sustainability of evidence-based prac- tice. In B. M. Melnyk & E. Fineout-Overholt (Eds.) Evidence- based practice in nursing & healthcare. A guide to best practice (3rd ed., pp. 274–315). Philadelphia, PA: Wolters Kluwer. Dearholt, S. L., & Dang, D. (2012). Johns Hopkins nursing
- 38. evidence- based practice model and guidelines (2nd ed.). Indianapolis, IN: Sigma Theta Tau International. Fineout-Overholt, E., & Melnyk, B. M. (2015). ARCC evidence- based practice mentors: The key to sustaining evidence-based practice. In B. M. Melnyk & E. Fineout-Overholt (Eds.) Evidence- based practice in nursing & healthcare. A guide to best practice (3rd ed., pp. 376–385). Philadelphia, PA: Wolters Kluwer. Fineout-Overholt, E., & Melnyk, B. M. (2006). Organizational cul- ture and readiness scale for system-wide integration of evidence-based practice. Gilbert, AZ: ARCC, llc. Graham, I. D., & Tetroe, J. & the KT Theories Research Group. (2007). Some theoretical underpinnings of knowledge transla- tion. Academic Emergency Medicine, 14(11), 936–941. Jun, J., Kovner, C. T., & Stimpfel, A. W. (2016). Barriers and facilitators of nurses’ use of clinical practice guidelines: An integrative review. International Journal of Nursing Studies, 60, 54–68. Levin, R. F., Fineout-Overholt, E., Melnyk, B. M., Barnes, M., & Vetter, M. J. (2011). Fostering evidence-based practice to improve nurse and cost outcomes in a community health setting: A pilot test of the advancing research and clinical practice through close collaboration model. Nursing Administration Quarterly, 35(1), 21–
- 39. 33. Melnyk, B. M. (2007). The evidence-based practice mentor: A promising strategy for implementing and sustaining EBP in healthcare systems. Worldviews on Evidence-Based Nursing, 4(3), 123–125. Melnyk, B. M. (2012). Achieving a high-reliability organization through implementation of the ARCC model for system wide sustainability of evidence-based practice. Nursing Administration Quarterly, 36(2), 127–135. Melnyk, B. M. (2016a). An urgent call to action for nurse lead- ers to establish sustainable evidence-based practice cultures and implement evidence-based interventions to improve healthcare quality. Worldviews on Evidence-Based Nursing, 13(1), 3–5. Melnyk, B. M. (2016b). Culture eats strategy every time: What works in building and sustaining an evidence-based practice cul- ture in healthcare systems. Worldviews on Evidence-Based Nurs- ing, 13(2), 99–101. Melnyk, B. M., & Fineout-Overholt, E. (2002). Putting research into practice. Reflections on Nursing Leadership, 28(2), 22–25. Melnyk, B. M., & Fineout-Overholt, E. (2003a). Evidence-based prac- tice beliefs scale. Gilbert, AZ: ARCC Publishing. Melnyk, B. M., & Fineout-Overholt, E. (2003b). Evidence-based prac- tice implementation scale (3rd ed.). Gilbert, AZ: ARCC
- 40. Publishing. Melnyk, B. M., & Fineout-Overholt, E. (2015). Evidence-based prac- tice in nursing and healthcare: A guide to best practice. Philadelphia, PA: Lippincott, Williams & Wilkins. Melnyk, B. M., Fineout-Overholt, E., Fischbeck Feinstein, N., Li, H., Small, L., Wilcox, L., & Kraus, R. (2004). Nurses’ perceived knowledge, beliefs, skills, and needs regarding evidence-based practice: Implications for accelerating the paradigm shift. World- views on Evidence-Based Nursing, 1(3), 185–193. Melnyk, B. M., Fineout-Overholt, E., Gallagher-Ford, L., & Kaplan, L. (2012). The state of evidence-based practice in U.S. nurses: Critical implications for nurse leaders and educators. Journal of Nursing Administration, 42(9), 410–417. Melnyk, B. M., Fineout-Overholt, E., Giggleman, M., & Cruz, R. (2010). Correlates among cognitive beliefs, EBP implementa- tion, organizational culture, cohesion and job satisfaction in evidence-based practice mentors from a community hospital system. Nursing Outlook, 58(6), 301–308. Melnyk, B. M., Gallagher-Ford, L., & Fineout-Overholt, E. (2016). Implementing the evidence-based practice competencies in healthcare. A practical guide for improving quality, safety and patient outcomes.
- 41. Indianapolis, IN: Sigma Theta Tau International. Melnyk, B. M., Fineout-Overholt, E., & Mays, M. (2008). The evidence-based practice beliefs and implementation scales: Psy- chometric properties of two new instruments. Worldviews on Evidence-Based Nursing, 5(4), 208–216. Melnyk, B. M., Gallagher-Ford, L., Thomas, B. K., Troseth, M., Wyngarden, K., & Szalacha, L. (2016). A study of chief nurse executives indicates low prioritization of evidence-based practice and shortcomings in hospital performance metrics across the United States. Worldviews on Evidence-based Nursing, 13(1), 6–14. Rosswurm, M. A., & Larrabee, J. H. (1999). A model for change to evidence-based practice. Image: Journal of Nursing Scholarship, 31(4), 317–322. Stevens, K. R. (2012). Star model of EBP: Knowledge transformation. Academic Center for Evidence-based Practice, TX: The Univer- sity of Texas Health Science Center at San Antonio. Titler, M. G., Kleiber, C., Steelman, V. J., Rakel, B. A., Budreau, G., Everett, L. Q., & . . . Goode, C. J. (2001). The Iowa Model of evidence-based practice to promote quality care. Critical Care Nursing Clinics of North America, 13(4), 497–509. Wallen, G. R., Mitchell, S. A., Melnyk, B. M., Fineout- Overholt, E., Miller-Davis, C., Yates, J., & Hastings, C. (2010). Implement- ing evidence-based practice: Effectiveness of a structured mul-
- 42. tifaceted mentorship programme. Journal of Advanced Nursing, 66(12), 2761–2771. doi 10.1111/wvn.12188 WVN 2017;14:5–9 Worldviews on Evidence-Based Nursing, 2017; 14:1, 5–9. 9 C© 2016 Sigma Theta Tau International Copyright of Worldviews on Evidence-Based Nursing is the property of Wiley-Blackwell and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use. Sustaining Evidence-Based Practice Through Organizational Policies and an Innovative Model The team adopts the Advancing Research and Clinical Practice Through Close Collaboration model. This is the 12th and last article in a series from the Arizona State University College of Nursing and Health Innovation’s Center for the Advancement of Evidence-Based Practice. Evidence-based practice (EBP) is a problem-solving approach to the delivery of health care that integrates the best evidence from studies and patient care data with clinician expertise and patient preferences and values. When it’s delivered in a context of caring and in a supportive organizational culture, the
- 43. highest quality of care and best patient outcomes can be achieved. The complete EBP series is available as a collection on our Web site; go to www.ajnonline.com and click on Collections. In July’s evidence-based prac-tice (EBP) article, Rebecca R., Carlos A., and Chen M. eval- uated the outcomes of their rapid response team (RRT) implemen- tation project. Their findings in- dicated that a significant decrease in one outcome, code rates outside the ICU, had occurred after im- plementation of the RRT. This promising finding, together with many other considerations—such as organizational readiness; clini- cian willingness; and a judicious weighing of all the costs, benefits, and outcomes—encouraged the EBP team to continue with plans to roll out the RRT protocol throughout the entire hospital system. They also began to work on presentations and publications about the project so that others could learn from their experience and implement similar interven- tions to improve patient outcomes. USING EVIDENCE TO INFORM ORGANIZATIONAL POLICY Because Rebecca, Carlos, and Chen are concerned about whether the implementation of an RRT can be sustained over time in their hospi-
- 44. tal, they want to take the neces- sary steps to create a hospital- wide RRT policy. Therefore, they make an appointment with their hospi- tal’s director of policies and pro- cedures, Maria P., to share the outcomes data they’ve gathered from their project and to discuss the project’s success so far. Maria is impressed by the rigor of the team’s sequential EBP process and the systematic way in which they’ve gathered the outcomes data. She reminds them that the measurement of outcomes (inter- nal evidence) plus rigorous re- search (external evidence) result in the best evidence-based orga- nizational policies to guide the high est quality of care in health care institutions. Maria volunteers to assist the team in writing a new evidence- based policy to support having an RRT in their hospital. She suggests that each recommendation in the policy be supported by evidence. Maria explains that once the pol- icy is written, it needs to be ap- proved by the hospital-wide policy committee, representing all of the health disciplines. Maria empha-
- 45. sizes that transdisciplinary health care professionals and administra - tors should routinely be involved when planning and implementing evidenced-based organizational policies. She also reminds the EBP team that translating evidence and evidence-based organizational pol- icies into sustainable routine clin- ical practices remains a major challenge for health care systems. The new RRT policy written by Rebecca, Carlos, and Chen with Maria’s help is approved by the hospital-wide policy committee within three months. Now the By Bernadette Mazurek Melnyk, PhD, RN, CPNP/PMHNP, FNAP, FAAN, Ellen Fineout-Overholt, PhD, RN, FNAP, FAAN, Lynn Gallagher- Ford, MSN, RN, NE-BC, and Susan B. Stillwell, DNP, RN, CNE, ANEF [email protected] AJN ▼ September 2011 ▼ Vol. 111, No. 9 57 It only takes one passionate, committed person to spearhead a team vision to improve care for patients and their families.
- 46. http://www.ajnonline.com challenge for the team is to work with clinicians across the hospital system to implement it. The EBP team schedules a series of presen- tations throughout the hospital to introduce the new RRT policy. They rotate the days and times of this in-service to capture as many direct care clinicians as possible. To ensure that all clinicians are educated on the new policy, a da- tabase is created to track in-ser- vice attendees, and each hos pital unit is asked to appoint a volun- teer to deliver the presentation to any clinicians who missed it. Post- ers are created and buttons de- signed as visual triggers to remind staff to implement the new policy. Throughout this process, the EBP team learned that dissemi- nation of evidence alone doesn’t typ ically lead clinicians to make a sustainable change to EBP, and they were impressed by how im- portant it was to have unit-based champions reinforce the new pol- icy.1 They also learned that it’s critical to have an organizational culture that supports EBP (such as evidence-based decision making
- 47. in tegrated into performance ex- pectations, up-to-date resources and tools, ongoing EBP knowledge and skills-building workshops, and EBP mentors at the point of care) in order for clinicians to con- sistently deliver evidence-based care.2 Since the process they followed worked so well, the team believes that their hospital needs to adopt a model to guide and reinforce the creation of a culture to sus- tain the EBP approach they had initiated through this project. They review several EBP process and system integration models and decide to adopt the Advanc- ing Research and Clinical Prac- tice Through Close Collaboration (ARCC) model because its key strategy to sustain evidence-based care is the presence of an EBP mentor (a clinician with advanced knowledge of EBP, mentorship, and individual as well as organi- zational change). With Carlos’s success as an expert EBP mentor, and the mentorship model work- ing so well, they believe that de- veloping a cadre of EBP mentors system-wide is key to the ongoing 58 AJN ▼ September 2011 ▼ Vol. 111, No. 9 ajnonline.com
- 48. Potential Strengths Philosophy of EBP (paradigm is system-wide) Presence of EBP mentors and champions Administrative support Clinicians’ beliefs about the value of EBP and ability to implement the EBP processa Identification of strengths and major barriers to EBP implementation EBP implementationa, b Decreased hospital costs Potential Barriers Lack of EBP mentors and champions
- 49. Inadequate EBP knowledge and skills Lack of EBP valuing Implementation of ARCC strategies Interactive EBP skills building EBP rounds and journal clubs Improved patient outcomes Nurse/clinician satisfaction Cohesion Intent to leave Turnover Development and use of EBP mentors
- 50. Assessment of organizational culture and readiness for EBP a Figure 1. The ARCC Model for System-Wide Implementation and Sustainability of EBP ARCC = Advancing Research and Clinical Practice Through Close Collaboration; EBP = evidence-based practice. a Scale developed. b Based on the EBP paradigm and using the EBP process. © 2 00 5, M el ny k an d Fi
- 51. ne ou t-O ve rh ol t. that this model be adopted, not only for the nursing department, but for all disciplines throughout the organization. THE EBP JOURNEY HAS JUST BEGUN This series presented a case in- volving a hypothetical medical– surgical nurse and her colleagues to illustrate how EBP can be suc- cessfully implemented to improve key patient outcomes. It’s impor- tant that the process start with an ongoing spirit of inquiry, and that nurses always question the evidence behind the care we pro- vide and never settle for the sta- tus quo. Never forget that it only takes one passionate, committed person to spearhead a team vi- sion to improve care for patients and their families. It also takes
- 52. persistence through the “charac- ter builders” that are sure to appear as the vision comes to fruition. Although the EBP team has successfully completed their RRT implementation project and its incorporation as a hospital-wide policy, their EBP journey has just be gun. In fact, only days after the project’s completion, Rebecca asked Carlos another great PICOT question: “In critically ill patients, how does early ambulation com- pared with delayed ambulation affect ventilator-associated pneu- monia in the ICU?” Carlos looked at her and replied, as a great men - tor does, “I will help you search for the evidence and we will find and organizational culture change. These individuals, whether expert system-wide mentors, advanced practice mentors, or peer mentors, are focused on helping point-of- care clinicians to use and sustain EBP and to conduct EBP imple- mentation, quality improvement, and outcomes management proj- ects. When clinicians work with EBP mentors, their beliefs about the value of EBP and their ability to implement it increase, and this is followed by a greater achieve-
- 53. ment of evidence-based care.4 The ARCC model contends that greater implementation of EBP results in higher job satisfaction, lower turnover rate, and better patient outcomes. A series of studies now support the empiri- cal relationships in the ARCC model.4-8 The ARCC model has been and continues to be implemented in hospitals and health care sys- tems across the country with ex- cellent results in quality of care and patient outcomes. Valid and reli- able instruments, such as the EBP Beliefs and EBP Implementation scales,6 are used to measure key constructs in the model and, to- gether with organizational culture and readiness for EBP, help to de- termine the model’s effectiveness.6 The EBP team discusses how all the elements of the ARCC model are an excellent fit for their organization. They decide to make a recommendation to the Shared Governance Steering Committee implementation and sustainabil- ity of EBP in their organization. SUSTAINING AN EBP CULTURE WITH THE
- 54. ARCC MODEL In reviewing the ARCC model, the EBP team finds that its aim is to provide hospitals and health care systems with an organized conceptual framework to guide system-wide implementation and sustainability of EBP for the pur- pose of improving quality of care and patient outcomes. In addition, this model can be used to achieve a “high reliability” organization (one that delivers safe and high- quality care), decrease costs, and improve clinicians’ job satisfaction. Four assumptions are basic to the ARCC model3: • Both barriers to and facilitators of EBP exist for individuals and within health care systems. • Barriers to EBP must be re- moved or mitigated and facili- tators put in place in order for individuals and health care sys - tems to implement EBP as a standard of care. • For clinicians to change their practices to be evidence based, both their beliefs about the value of EBP and their confi- dence in their ability to imple- ment it must be strengthened.
- 55. • An EBP culture that includes EBP mentors is necessary in order to advance and sustain EBP in individuals and health care systems. The first step in the ARCC model is to assess the organiza- tion’s culture and readiness for EBP (see Figure 1). From that assess- ment, the strengths and limita tions of implementing EBP within the organization can be identified. The key implementation strategy in the ARCC model is the development of a cadre of EBP mentors, who are typically advanced practice nurses or clinicians with in-depth knowledge of and skills in EBP and in individual behavior change [email protected] AJN ▼ September 2011 ▼ Vol. 111, No. 9 59 Developing a cadre of EBP mentors system-wide is key to the ongoing implementation and sustainability of EBP in an organization. Wiley-Blackwell; Sigma Theta Tau; 2010. p. 169-84.
- 56. 4. Melnyk BM, et al. Nurses’ perceived knowledge, beliefs, skills, and needs regarding evidence-based practice: im - plications for accelerating the para- digm shift. Worldviews Evid Based Nurs 2004;1(3):185-93. 5. Levin RF, et al. Fostering evidence- based practice to improve nurse and cost outcomes in a community health setting: a pilot test of the advancing research and clinical practice through close collaboration model. Nurs Adm Q 2011;35(1):21-33. 6. Melnyk BM, et al. The evidence- based practice beliefs and implemen- tation scales: psychometric properties of two new instruments. Worldviews Evid Based Nurs 2008;5(4):208-16. 7. Melnyk BM, et al. Correlates among cognitive beliefs, EBP implementa- tion, organizational culture, cohesion and job satisfaction in evidence-based practice mentors from a community hospital system. Nurs Outlook 2010; 58(6):301-8. 8. Wallen GR, et al. Implementing evidence-based practice: effectiveness of a struc tured multifaceted mentor- ship programme. J Adv Nurs 2010; 66(12):2761-71. Practice. Contact author: Berna dette
- 57. Mazurek Melnyk, [email protected] The authors have disclosed no potential conflicts of inter est, financial or other- wise. REFERENCES 1. Melnyk BM, Wiliamson KM. Using evidence-based practice to enhance organizational policies, healthcare qual - ity, and patient outcomes. In: Hinshaw AS, Grady PA, editors. Shaping health policy through nursing research. New York: Springer Publishing Company; 2011. p. 87-98. 2. Melnyk BM, Fineout-Overholt E. Evidence-based practice in nursing and healthcare: a guide to best prac- tice. Philadelphia: Wolters Kluwer Health/Lippincott Williams and Wil- kins; 2011. 3. Melnyk BM, Fineout-Overholt E. ARCC (Advancing Research and Clini- cal prac tice through close Collabora- tion): a model for system-wide implementation and sustainability of evidence-based practice. In: Rycroft- Malone J, Bucknall T, editors. Models and frame works for implementing evidence-based practice: linking evi- dence to action. Oxford; Ames, IA: the answer to your question— because EBP, not practices steeped
- 58. in tradition, is the only way we do it here!” ▼ Bernadette Mazurek Melnyk is associate vice president for health promotion, uni- versity chief wellness officer, and dean of The Ohio State University College of Nurs - ing in Columbus, where Lynn Gallagher- Ford is director of Transdisciplinary Evidence-Based Practice and Clinical Innovation. Ellen Fineout-Overholt is dean of Professional Studies and chair of the Department of Nursing at East Texas Baptist University in Mar shall, TX. Susan B. Stillwell is clinical professor and associate director of the Center for the Advancement of Evidence-Based Practice at Arizona State Univer sity in Phoenix. At the time this article was written, Ber- nadette Mazurek Melnyk was dean and distinguished foundation professor of nursing in the College of Nurs ing and Health Innovation at Arizona State Uni- versity, where Ellen Fineout-Overholt was clinical pro fessor and director, and Lynn Gallagher-Ford was clinical assistant pro- fessor and assistant director, of the Center for the Advancement of Evidence-Based LWW/NAQ NAQ200184 March 1, 2012 23:19 Nurs Admin Q Vol. 36, No. 2, pp. 127–135
- 59. Copyright c© 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins Achieving a High-Reliability Organization Through Implementation of the ARCC Model for Systemwide Sustainability of Evidence-Based Practice Bernadette Mazurek Melnyk, PhD, RN, CPNP/PMHNP, FNAP, FAAN High-reliability health care organizations are those that provide care that is safe and one that min- imizes errors while achieving exceptional performance in quality and safety. This article presents major concepts and characteristics of a patient safety culture and a high-reliability health care organization and explains how building a culture of evidence- based practice can assist organiza- tions in achieving high reliability. The ARCC (Advancing Research and Clinical practice through close Collaboration) model for systemwide implementation and sustainability of evidence-based practice is highlighted as a key strategy in achieving high reliability in health care organizations. Key words: evidence-based practice, high-reliability organizations, patient safety H IGH-RELIABILITY ORGANIZATIONS(HROs) are those that achieve a high degree of safety or reliability despite dan- gerous or hazardous conditions.1 They have defect-free or error-free operations for long periods of time.2 The Blue Angels and the
- 60. aviation industry are excellent examples of HROs. The Blue Angels are the United States Navy’s Flight Demonstration Squadron and the oldest formal flying aerobatic team. They operate 6 F/A-18 Hornet aircraft and conduct more than 70 daring flight exhibits every year throughout the United States in which they Author Affiliation: College of Nursing, The Ohio State University, Columbus. The author declares no conflict of interest. Correspondence: Bernadette Mazurek Melnyk, PhD, RN, CPNP/PMHNP, FNAP, FAAN, College of Nursing, The Ohio State University, 1585 Neil Ave, Columbus, OH 43210 ([email protected]). DOI: 10.1097/NAQ.0b013e318249fb6a perform many extremely dangerous maneu- vers, including high-speed passes (often just under the speed of sound), slow passes, fast rolls, tight turns, and the Diamond formation. Training and performance require intense focus, strong leadership, effective commu- nication, teamwork, data-based practices, root-cause analysis of errors, a safety and continuous learning culture, improvement processes, and an outcomes evaluation. The health care industry, which has been fraught with an epidemic of medical errors, has looked to HROs to learn about and imple- ment cultures along with practices that will lead to safer environments with a higher qual-
- 61. ity of care and efficiency. Every year, there are up to 200,000 unintended patient deaths, more than the number of deaths that occur due to motor vehicle accidents, breast can- cer, and AIDS.3 Patient injuries happen to ap- proximately 15 million individuals per year. Only 5% of medical errors are caused by Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. 127 LWW/NAQ NAQ200184 March 1, 2012 23:19 128 NURSING ADMINISTRATION QUARTERLY/APRIL– JUNE 2012 incompetence, whereas 95% of errors in- volve competent clinicians trying to attain the best outcomes in poorly designed sys- tems with poor uniformity.4 Furthermore, core processes in health care are defective 50% of the time and patients receive only ap- proximately 55% of the care that they should when entering the health care system.5 The movement to improve patient safety in health care systems accelerated after the land- mark publication by the Institute of Medicine of To Err Is Human: Building a Safer Health System.6 Evidence regarding major factors that reduce errors in health care systems in- clude (a) effective communication and trans-
- 62. disciplinary teamwork; (b) evidence-based interventions, which also improve standard- ization of care and decrease variation; (c) sensitivity to operations; and (d) improved systems design, which includes the use of checklists, decreasing interruptions, prevent- ing fatigue, avoiding task saturation, reducing clinician stress, and improving environmen- tal conditions.1,7,8 In addition to the current emphasis on reducing medical errors, pay for performance has placed pressure on health care systems to improve their quality of care and prevent sentinel events. One key strategy to improving quality of care is through the implementation of evidence-based practice (EBP). However, de- spite an aggressive research movement, the majority of findings from research are often not translated into clinical practice to enhance care and patient outcomes. At best, it usu- ally takes several years to translate research findings into health care settings to improve patent care. In an era of cost-driven health care systems, research that demonstrates a re- duction in costs has a higher probability of be- ing adopted in clinical practice. For example, through a series of 6 randomized controlled trials, the efficacy of the COPE (Creating Op- portunities for Parent Empowerment) pro- gram has been established with parents of hos- pitalized/critically ill children and premature infants. Findings from these trials have indi- cated that when parents receive COPE versus an attention control program, parents report
- 63. less stress, anxiety, depression, and posttrau- matic stress symptoms, up to 2 years follow- ing hospitalization.9-14 In addition, their chil- dren have better developmental and behavior outcomes. However, it was not until a clini- cal trial using COPE with parents of preterms demonstrated a 4-day shorter length of neona- tal intensive care unit (ICU) stay (8 days shorter for preterms younger than 32 weeks) that hospitals and insurers began implement- ing the program.10 Routine implementation of the COPE program to the parents of the more than 500 000 preterm infants born in the United States every year could save the health care system between $2.5 billion and $5 bil- lion per year.15 This is an example of the “so what factor” in an era of health care reform, which is conducting research and EBP/quality improvement projects with high-impact po- tential to positively change health care sys- tems, reduce costs, and improve outcomes for patients and their families.16 Key questions that anyone should ask themselves when em- barking on a research study or EBP/quality improvement project should be as follows: (1) So what will the outcome of the study or project be once it is completed? and (2) So what difference will the study or project make in improving health care quality, costs, or patient outcomes? Estimates are that the cost of health care de- livery in the United States is $2.3 trillion a year, a tripling of its cost in the past 2 decades.17 Poor quality health care cost the United States
- 64. approximately $720 billion in 2008. Wasteful health care spending costs the health care sys- tem $1.2 trillion annually. Half of American hospitals are functioning in deficit.18 In addi- tion to EBP improving patient outcomes by at least 28%, the US health care system could re- duce health care spending by 30% if patients receive evidence-based care.19 HIGH-RELIABILITY HEALTH CARE ORGANIZATIONS A high-reliability health care organization (HRHO) provides care that is safe and one that minimizes errors while achieving exceptional Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. LWW/NAQ NAQ200184 March 1, 2012 23:19 The ARCC Model for Systemwide Sustainability of EBP 129 performance in quality and safety. It has a mea- surable, near perfect performance on quality of care, patient safety, and efficiency. Creat- ing a culture and processes that radically re- duce system failures and effectively respond- ing when failures do occur is the goal of HROs. FIVE KEY CONCEPTS OF HIGH-RELIABILITY HEALTH CARE ORGANIZATIONS
- 65. The first key concept of an HRHO is sensi- tivity to operations, which is an awareness of the state of systems and processes that affect patient care. When an organization is sensi- tive to operations, potential errors are identi- fied and prevented. In addition, actual errors are identified immediately and corrected.20 The second key concept of HRHO is a reluc- tance to simplify. It is positive to create simple processes in health care systems but not to oversimplify explanations for adverse events. For example, if a clinician makes a medical error, it would be simple to conclude that the clinician was the cause of the error instead of investigating the complete chain of events, from the physician’s order to the filling of that order by a pharmacist to the delivery of the medication. The third key concept in an HRHO is pre- occupation with failure. Although it is very important to gather meticulous data on the number of medical errors or sentinel events in a health care system, when an error or ad- verse event happens, it is an opportunity to thoroughly examine the root cause for the problem and to make improvements. The fourth key concept in an HRHO is def- erence to expertise. In an HRHO, leaders lis- ten to and respond to others’ insights, includ- ing direct care clinicians, patients, and family members. Input from others is taken into con- sideration in establishing care processes and strategies to improve safety and quality.
- 66. The fifth key concept in an HRHO is re- silience. In an HRHO, leaders and staff need to be trained in how to respond when system failures do occur. They must be prepared and equipped with the right tools and resources to be able to respond to at-risk situations and prevent medical errors or sentinel events from occurring.20 In an HRHO, effective teams are key to op- timal functioning. Characteristics of effective teams in HROs include (a) outstanding team leadership, in which team members have a clear vision and purpose and the roles of each team member are clear; (b) backup behavior, which is when team members are capable of self-correcting behaviors and feedback is pro- vided regularly; (c) mutual performance mon- itoring, where team members understand and monitor each other’s roles; (d) communica- tion adaptability, in which communication is clear, often, and enough; and (e) mutual trust, in which each member of a team trusts each other’s intentions.21 A CULTURE OF PATIENT SAFETY Although a culture of patient safety is a ne- cessity in an HRHO, it is often challenging to define and measure a safe culture. In a com- prehensive literature review whose purpose was to organize the properties of a safety cul- ture, Sammer and colleagues3 identified the following as essential components: (a) lead-
- 67. ership, in which key leaders are aware that the health care environment is one of risk and seek to reduce risk by aligning the vi- sion/mission, staff competencies, and fiscal and human resources with frontline care; (b) teamwork, which includes collaboration and cooperation among leaders and staff mem- bers; (c) evidence-based, in which practices are based on the best evidence to improve standardization and reduce variation; (d) com- munication, in which the environment facili- tates each member to speak up on behalf of a patient; (e) learning, in which the health care system learns from its mistakes and seeks to continually improve its processes and perfor- mance; (f) just, in which the culture is one that sees errors as system failures rather than individual failures; and (g) patient-centered, in which the care in the health care system is centered around the patients and family members. Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. LWW/NAQ NAQ200184 March 1, 2012 23:19 130 NURSING ADMINISTRATION QUARTERLY/APRIL– JUNE 2012 MEASUREMENT OF PATIENT SAFETY Data-driven decisions are an important part of an HRHO; therefore, careful monitoring
- 68. of patient safety is essential. Scorecards can be used to track patient safety outcomes. For example, Pronovost and colleagues1 describe the framework for a patient safety scorecard in an HRO that includes the following: (a) How often do we harm patients (measured by the number of medical errors or sen- tinel events, such as catheter-associated blood stream infections)? (b) How often do we pro- vide interventions that patients should receive (eg, the proportion of patients who receive evidence-based interventions)? (c) How often do we learn from defects? (eg, the propor- tion of months that each patient care area learns from its mistakes and includes root- cause analysis along with revised policies to prevent future errors); (d) How well have we created a culture of safety? (eg, the percent- age of patient care areas in which 80% of the staff report a positive safety and teamwork cli- mate). The framework and concepts from an HRO are helpful in developing HRHOs. How- ever, it should be remembered that, although concepts from HROs can be used to improve processes and outcomes in health care sys- tems, they are not meant to replace safety and quality initiatives that are already be- ing implemented and successful in improving outcomes. RECOMMENDATIONS FOR LEADERS TO CREATE HIGH-RELIABILITY CULTURES A variety of strategies can be implemented by leaders to create HRHOs. The first strat- egy is to conduct transdisciplinary team train-
- 69. ing in which all managers and staff are taught about HROs and methods to achieve them. The second strategy is deliberately designing key care processes to reduce risk and en- sure high-quality care. Third, it is important that all members of the team understand its key processes. Fourth, it is critical to error proof the organization. The fifth strategy in- volves process standardization (ie, uniformity in how care is delivered to patients).21 Finally, as part of building an HRHO, it is critical to cultivate a culture of EBP in which there is a never-ending spirit of inquiry within ev- eryone in the organization regarding how to improve the quality, safety, and efficiency of care. EVIDENCE IS KEY IN BOTH HIGH-RELIABILITY ORGANIZATIONS AND EVIDENCE-BASED PRACTICE CULTURES Careful tracking of data along with outcomes monitoring of key system and patient outcomes is critical in an HRHO. Furthermore, external evidence from both rigorous research and internal evidence (ie, data that are generated from practice, pa- tients, and outcomes management) is criti- cal to formulating the best practices to im- prove the quality and safety of care. In an HRHO and an EBP culture, leaders engage in evidence-based management and clinicians engage in EBP. Evidence-based practice is a problem-solving approach to the delivery of
- 70. care that integrates the best evidence from well-designed studies with a clinician’s ex- pertise, including clinical wisdom, reasoning, patient history, physical data collection and resource utilization, and a patient’s prefer- ences and values to make decisions about the type of care provided.22 The ultimate pur- pose of EBP is to improve health care qual- ity and patient outcomes and reduce hospital costs. When evidence-based care is delivered within an EBP culture and a context of car- ing, the best patient outcomes are achieved (Figure 1). THE STEPS OF EVIDENCE-BASED PRACTICE To build HRHOs and EBP cultures, clini- cians should learn and consistently implement the steps of EBP, which include (1) cultivate a spirit of inquiry; (2) ask clinical questions in PICOT format, which stands for patient pop- ulation of interest, intervention of interest, Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. LWW/NAQ NAQ200184 March 1, 2012 23:19 The ARCC Model for Systemwide Sustainability of EBP 131 Clinical decision making
- 71. Quality patient outcomes Research evidence and evidence-based theories Clinical expertise (eg, evidence from patient assessment, internal evidence, and the use of health care resources) Patient preferences Context of caring EBP organizational culture Figure 1. The evidence-based practice (EBP) paradigm. Copyright 2003 Melnyk and Fineout-Overholt. comparison intervention or group, outcome, and time (eg, In intubated patients in the ICU (P), how does early ambulation (I) vs delayed ambulation (C) affect episodes of ventilator- associated pneumonia (O) while in the ICU (T)?); (3) search for the best evidence; (4) in- tegrate the evidence with clinical expertise and patient preferences to make the best clin- ical decision; (5) evaluate the outcome(s) of the EBP change; and (6) disseminate the out- comes so that other patients can benefit. In EBP, if there is enough high-quality evidence
- 72. from research to change practice, the prac- tice is changed and outcomes are monitored to support that the change in practice based on research produces positive outcomes in the real-world setting. If there is not enough high-quality evidence to change practice, ex- ternal evidence must be generated through rigorous research or internal evidence pro- duced through quality improvement or out- comes management projects. High-reliability health care organizations begin with leaders and point-of-care providers who take the time to think and reflect about the care that is be- ing delivered and continually ask how it can be improved, which is analogous to cultivat- ing a spirit of inquiry or step 0 in the EBP process. CHARACTERISTICS OF BOTH HIGH-RELIABILITY HEALTH CARE ORGANIZATIONS AND EVIDENCE-BASED PRACTICE CULTURES There are many similarities between build- ing an HRHO and an EBP culture. Character- istics of both are included in the Table. Both HRHOs and EBP cultures work to obtain the highest levels of health care quality, safety, and patient outcomes. Outcomes monitoring Table. Characteristics of Both High- Reliability Organizations and Evidence- Based Practice Cultures Commitment to delivering high-quality care and patient safety and reducing costs
- 73. Strong leadership Emphasis on process and systems design Transdisciplinary teamwork Effective communication Delivery/standardization of best practices and policies An environment that promotes a spirit of inquiry and continuous learning Focus on continual process improvement Outcomes monitoring/evaluation Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. LWW/NAQ NAQ200184 March 1, 2012 23:19 132 NURSING ADMINISTRATION QUARTERLY/APRIL– JUNE 2012 is a critical strategy in both HRHOs and EBP cultures because outcomes reflect the impact that is being made on health care quality, pa- tient outcomes, and system outcomes. BARRIERS TO AND FACILITATORS OF ADVANCING HIGH-RELIABILITY HEALTH CARE ORGANIZATIONS AND EVIDENCE-BASED PRACTICE CULTURES There are multiple barriers to leaders and clinicians succeeding in developing an HRHO
- 74. and an EBP culture. Some of the major barri- ers include (a) lack of knowledge and skills in both HRHOs and EBP; (b) perceived lack of time; (c) lack of organizational/administrative support; and (d) educational programs that continue to teach the “traditional way” with a focus on producing research instead of us- ing evidence to improve practice; and (e) lack of mentorship.23-26 Conversely, facilitators of building HRHOs and EBP cultures include (a) knowledge and skills of HRHOs and EBP, (b) beliefs that these types of organizations and cultures improve care and patient out- comes; (c) beliefs in the ability to implement EBP and key concepts of HRHOs; (d) men- tors who are skilled in EBP and HRHO con- cepts; and (e) administrative/organizational support, including leaders and managers who model important behaviors related to EBP and HRHOs.22,27,28 THE ARCC MODEL AS AN EXAMPLE OF HOW BUILDING AN EVIDENCE-BASED PRACTICE CULTURE FACILITATES A HIGH-RELIABILITY HEALTH CARE ORGANIZATION Use of the EBP paradigm assists organi- zations in achieving high reliability. There is evidence to indicate that implementation of evidence-based care helps reduce defects in care processes, improves quality of care and patient outcomes, standardizes care, de- creases variations in care, increases efficiency and decreases health care costs.1,22,25,29,30
- 75. The ARCC (Advancing Research and Clin- ical practice through close Collaboration) model is a systemwide model that can be used by health care systems and hospitals for sus- taining EBP and facilitating an HRHO (Figure 2). The ARCC model was first conceptualized in 1999 as part of a strategic planning process at a major medical center to rapidly integrate research findings with clinical practice for the ultimate purpose of improving quality of care and patient outcomes. Four assumptions are inherent in the ARCC model: (1) There are barriers and facilitators of EBP for individu- als and within health care systems. (2) Barri- ers to EBP must be removed or mitigated and facilitators put in place for both individuals and health care systems to implement EBP as standard of care. (3) In order for clinicians to change their practices to be evidence-based, cognitive beliefs about the value of EBP and confidence about the ability to implement it must be strengthened. (4) A culture of EBP that includes EBP mentors (ie, clinicians with advanced knowledge and skills in EBP, men- torship, and individual as well as organiza- tional change) is necessary to advance and sustain evidence-based care.31 Implementation of the ARCC model be- gins with an assessment of the culture and readiness for EBP, which allows for the iden- tification of strengths and limitations within the health care system that either facilitate or hinder the development of an EBP culture. Next, a cadre of EBP mentors is developed
- 76. whose role is to address the limitations, en- hance the strengths in the health care system to build an EBP culture, and work directly with point-of-care clinicians in implementing and sustaining EBP. The ARCC model con- tends that, when clinicians are mentored in EBP, their cognitive beliefs about the value of EBP and their ability to implement it are strengthened, which results in greater imple- mentation of EBP. Furthermore, when EBP is implemented, there is improvement in patient outcomes and clinician group cohesion and job satisfaction, which ultimately results in less turnover within the organization. To date, several studies have been conducted that have supported relationships among constructs in the ARCC model.28,32,33,34 Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. LWW/NAQ NAQ200184 March 1, 2012 23:19 The ARCC Model for Systemwide Sustainability of EBP 133 Figure 2. The ARCC model for systemwide implementation and sustainability of evidence-based practice (EBP) can facilitate a high-reliability health care organization. Copyright 2005 Melnyk and Fineout-Overholt. aScale developed. bBased on EBP paradigm and using the EBP process. Implementation of the ARCC model is ac- complished through a 12-month program to
- 77. prepare a cadre of EBP mentors who then work with direct care staff to implement and sustain EBP throughout the health care sys- tem. Evidence-based practice mentors are typ- ically advanced practice nurses or transdisci- plinary professionals or clinicians with bach- elor’s degrees. A series of 6 workshops with 8 days of educational and skills building ses- sions are conducted over the yearlong ARCC program, which is focused on implementing the 7-step EBP process and necessary strate- gies for building an EBP culture. Major con- tent of the ARCC workshops includes (a) EBP skills building; (b) creating a vision to mo- tivate a change to EBP; (c) transdisciplinary team building and effective communication; (d) mentorship to advance EBP; (e) strate- gies to build an EBP culture; (f) quality im- provement processes; (g) data management and outcomes monitoring/evaluation; and (h) theories and principles of individual behav- ior change and organizational change. Before the first workshop, a baseline assessment is conducted to assess the clinicians’ EBP be- liefs, EBP implementation, organizational cul- ture and readiness for EBP, job satisfaction, and group cohesion. Patient data on problems identified for improvement by the clinicians in the ARCC program are also collected and ana- lyzed. Each team that is attending the series of workshops implements an EBP implementa- tion project during the course of the 12-month program focused on improving quality of care, safety, and/or patient outcomes. Examples of projects and outcomes from the most re-
- 78. cent implementation of the ARCC model at the Washington Hospital Healthcare System, a 355-bed community hospital system in the Western region of the United States, include the following: (a) Early ambulation in the ICU Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. LWW/NAQ NAQ200184 March 1, 2012 23:19 134 NURSING ADMINISTRATION QUARTERLY/APRIL– JUNE 2012 resulted in a reduction in ventilator days from 11.6 to 8.9 days and no ventilator-associated pneumonias. (b) Pressure ulcer rates were re- duced from 6.07% to 0.62% on a medical sur- gical unit. (c) Education of patients with con- gestive heart failure led to a 14.7% reduction in hospital readmissions. (d) Seventy-five per- cent of parents perceived the overall quality of care as excellent after implementation of an evidence-based family-centered care program compared with 22.2% before implementation. MAJOR FACTORS INFLUENCING ADOPTION OF EVIDENCE-BASED PRACTICES There are a number of factors that can in- fluence the adoption of EBPs. Some of these factors include (a) the characteristics of the EBP (eg, the strength of evidence to support
- 79. the practice, ease of administration, and cost); (b) characteristics of the clinician (eg, the un- derstanding and cognitive beliefs/confidence to implement it and self-efficacy; (c) the envi- ronment and culture of the organization; and (d) the process through which the change is implemented (eg, consensus building and use of EBP mentors and opinion leaders).35,36 These same factors are likely to exist when ap- plying concepts from HROs in health care or- ganizations. For clinicians to implement best practices and concepts from HROs, it must be made easy and fun as they are overburdened with patient loads and competing priorities. In addition, routine recognition and apprecia- tion for efforts should be built in on a regular basis to recognize individuals and teams for their efforts. Furthermore, building EBPs and concepts from HROs into electronic medical records may help improve quality of care and patient safety, but too many reminders may lead clinicians to ignore them. CONCLUSION Concepts from HROs are being built into health care systems both to improve quality of care and patient safety and to improve ef- ficiency and reduce health care costs. Sub- stantial overlap exists in building HRHOs and EBP cultures. Implementation of the ARCC model for systemwide implementation and sustainability of EBP can assist organizations in achieving high reliability.
- 80. REFERENCES 1. Pronovost PJ, Berenholtz SM, Goeschel CA, et al. Creating high reliability in health care organizations. Health Serv Res. 2006;41(4)(pt II):1599-1617. 2. Reinertsen JL, Clancy C. Keeping our promises: re- search, practice and policy issues in healthcare re- liability. A special issue of health services research (Forward). Health Serv Res. 2006;10:1677-1689. 3. Sammer CE, Lykens K, Singh KP, Mains DA, Lackan NA. What is a patient safety culture? A review of the literature. J Nurs Scholarsh. 2010;42(2):156-165. 4. Leonard M, Frankel A, Simmonds T, Vega KB. Achiev- ing Safe and Reliable Healthcare. Chicago, IL: Health Administration Press; 2004. 5. Resar RK. Practical applications of reliability the- ory. Making noncatastrophic health care processes reliable: learning to walk before running in creat- ing high reliability organizations. Health Serv Res. 2006;41(4)(pt II):1677-1689. 6. Kohn LT, Corrigan J, Donaldson MS. Institute of Medicine. To Err Is Human: Building a Safer Health System. Washington, DC: National Academies Press; 2000. 7. Carroll JS, Rudolph JW. Design of high reliability or- ganizations in health care. Qual Saf Health Care. 2006;15(suppl 1):i4-i9. 8. McKeon LM, Oswaks JD, Cunningham PD. Safeguard-
- 81. ing patients. Complexity science, high reliability or- ganizations, and implications for team training in healthcare. Clin Nurse Spec. 2006;20(6):298-304. 9. Melnyk BM. Coping with unplanned childhood hos- pitalization: effects of informational interventions on mothers and children. Nurs Res. 1994;43(1):50-55. 10. Melnyk BM, Feinstein NF, Alpert-Gillis L, et al. Re- ducing premature infants length of stay and im- proving parents’ mental health outcomes with the COPE NICU program: a randomized clinical trial. Pediatrics. 2006;118(5):1414-1427. 11. Melnyk BM, Alpert-Gillis L, Feinstein NF, et al. Creat- ing opportunities for parent empowerment (COPE): program effects on the mental health/coping outcomes of critically ill young children and their mothers. Pediatrics. 2004;113(6):e597-e607. http:// pediatrics.aappublications.org/content/113/6/e597. full.html. Accessed June 1, 2011. Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. LWW/NAQ NAQ200184 March 1, 2012 23:19 The ARCC Model for Systemwide Sustainability of EBP 135 12. Melnyk BM, Alpert-Gillis L, Feinstein NF, et al. Im- proving cognitive development of LBW premature infants with the COPE program: a pilot study of the benefit of early NICU intervention with mothers. Res Nurs Health. 2001;24:373-389.
- 82. 13. Melnyk BM, Alpert-Gillis LJ, Hensel PB, Cable-Billing RC, Rubenstein J. Helping mothers cope with a crit- ically ill child: a pilot test of the COPE intervention. Res Nurs Health. 1997;20:3-14. 14. Vulcan [Melnyk] BM, Nikulich-Barrett M. The ef- fects of selected information on mothers’ anxiety lev- els during their children’s hospitalization. J Pediatr Nurs. 1988;3(2):97-102. 15. Melnyk BM, Feinstein N. Reducing hospital expen- ditures with the COPE (Creating Opportunities for Parent Empowerment) program for parents and pre- mature infants: an analysis of direct healthcare neona- tal intensive care unit costs and savings. Nurs Adm Q. 2009;33(1):32-27. 16. Melnyk BM. The “so what” factor in a time of health- care reform: conducting research & EBP projects that impact healthcare quality, cost and patient outcomes. Distinguished Research Lecturer paper presented at: the proceedings of the Western Institute of Nursing Conference; April 2011; Las Vegas, Nevada. 17. Hader R. The evidence that isn’t. Nurs Manag. 2010;41(9):22-26. 18. American Hospital Association. TrendWatch Chartbook 2007: trends affecting hospitals and health systems. http://www.aha.org/aha/ trendwatch/chartbook/2007/07chapter4.ppt#10. Accessed June 1, 2011. 19. Buntin MB, Damberg C, Haviland A, et al. Consumer- directed health care: early evidence about effects on
- 83. cost and quality. Health Aff. 2006;25(6):W516-W530. 20. Hines S, Luna K, Lofthus J, et al. Becoming a High Re- liability Organization: Operational Advice for Hos- pital Leaders. Prepared by the Lewin Group under Contract No. 290-04-0011. Rockville, MD: Agency for Healthcare Research and Quality; 2008.AHRQ Publi- cation No. 08-0022. 21. Riley W. High reliability and implications for nursing leaders. J Nurs Manag. 2009;17:238-246. 22. Melnyk BM, Fineout-Overholt E. Evidence-Based Practice in Nursing & Healthcare: A Guide to Best Practice. 2nd ed. Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins; 2011. 23. Cabana MD, Slish KK, Evans D, et al. Impact of physi- cian asthma care education on patient outcomes. Pe- diatrics. 2006;117(6):2149-2157. 24. Hannes K, Vandersmissen J, De Blaeser L, Peeters G, Goedhuys J, Aertgeerts B. Barriers to evidence- based nursing: a focus group study. J Adv Nurs. 2007;60(2):162-171. 25. McGinty J, Anderson G. Predictors of physician com- pliance with American Heart Association Guidelines for acute myocardial infarction. Crit Care Nurs Q. 2008;31(2):161-172. 26. Melnyk BM, Fineout-Overholt E, Mays M. The evidence-based practice beliefs and implementation scales: psychometric properties of two new instru- ments. Worldviews Evid Based Nurs. 2008;5(4):208-
- 84. 216. 27. Melnyk BM. The evidence-based practice mentor: a promising strategy for implementing and sustaining EBP in healthcare systems. Worldviews Evid Based Nurs. 2007;4(3):123-125. 28. Melnyk BM, Fineout-Overholt E, Giggleman M, Cruz R. Correlates among cognitive beliefs, EBP im- plementation, organizational culture, cohesion and job satisfaction in evidence-based practice mentors from a community hospital system. Nurs Outlook. 2010;58(6):301-308. 29. Williams DO. Treatment delayed is treatment denied. Circulation. 2004;109:1806-1808. 30. PricewaterhouseCoopers’ Health Research Institute. What works: healing the healthcare staffing shortage. http://www.pwc.com/us/en/healthcare/publications /what-works-healing-the-healthcare-staffing-shortage .jhtml. Published 2007. Accessed June 1, 2011. 31. Melnyk BM, Fineout-Overholt E. ARCC (Advancing Research and Clinical practice through close Col- laboration). A model for system-wide implemen- tation and sustainability of evidence-based prac- tice. In: Rycroft-Malone J, Bucknall T, eds. Models and Frameworks for Implementing Evidence-Based Practice. Philadelphia, PA: Blackwell Publishing; 2010: 169–184. 32. Levin RF, Fineout-Overholt E, Melnyk BM, Barnes M, Vetter MJ. Fostering evidence-based practice to improve nurse and cost outcomes in a community health setting: a pilot test of the advancing research