
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Appendicitis
Similar to Appendicitis (20)
Recently uploaded
Recently uploaded (20)
Appendicitis
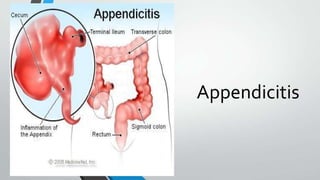
- 1. Appendicitis
- 2. Definition Source: Bailey & Loves Short Practice of Surgery 25th ed • An inflammation of the vermiform appendix etiology: • No unifying hypothesis • Decreased dietary fibre and increased consumption of refined carbohydrates • Obstruction of the appendix lumen –Fecolith (composed of inspissated faecal material, calcium phosphates, bacteria, epithelial debris, rarely a foreign body) –Tumour (carcinoma of caecum) –Intestinal parasites (Oxyuris/Enterobius vermicularis – pinworm)
- 3. Risk Factors for Perforation of TheAppendix Source: Bailey & Loves Short Practice of Surgery 25th ed
- 4. Clinical Manifestations Source: Bailey & Loves Short Practice of Surgery 25th ed
- 8. Differential Diagnosis Source: Bailey & Loves Short Practice of Surgery 25th ed
- 9. Investigation Source: Bailey & Loves Short Practice of Surgery 25th ed
- 10. Diagnostic Scoring Source: Bailey & Loves Short Practice of Surgery 25th ed • Diagnosis is essentially clinical; • HOWEVER a decision to operate based on clinical suspicion only can lead to the removal of a normal appendix. • A number of clinical and laboratory-based scoring systems have been devised to assist diagnosis. • The most widely used is Alvarado score.
- 11. The Alvarado (MANTRELS)Score Source: Bailey & Loves Short Practice of Surgery 25th ed Score Symptoms •Migratory RIF pain 1 •Anorexia 1 •Nausea and vomiting 1 Signs •Tenderness (RIF) 2 •Rebound tenderness 1 •Elevated temperature 1 Laboratory •Leucocytosis 2 •Shift to the left (segmented neutrophils) 1 TOTAL 10 • • • < 5 is strongly against a diagnosis of appendicitis 7 or more is strongly predictive of acute appendicitis In patients with an equivocal score of 5 or 6, abdominal USG or contrast-enhanced CT scan is used to further reduce the rate of negative appendicectomy
- 12. CT Scan images of Appendicitis: 1. enlarged appendix 2. appendiceal wall thickening Source:Choi D, Park H, Lee YR, Kook SH, Kim SK, Kwag HJ, Chung EC. The most useful findings for diagnosing acute appendicitis on contrast-enhanced helical CT. Acta Radiologica 44 (2003) 574-582.
- 13. CT Scan images of Appendicitis 3. appendicolith 4.periappendiceal fat stranding Source:Choi D, Park H, Lee YR, Kook SH, Kim SK, Kwag HJ, Chung EC. The most useful findings for diagnosing acute appendicitis on contrast-enhanced helical CT. Acta Radiologica 44 (2003) 574-582.
- 14. Treatment Source: Bailey & Loves Short Practice of Surgery 25th ed • Intravenous fluids • to establish adequate urine output • Appropriate antibiotics • • Reduces the incidence of postoperative wound infection When peritonitis is suspected, therapeutic intravenous antibiotics to cover Gram- negative bacilli as well as anaerobic cocci should be given • Salicylates • Appendicectomy
- 16. Appendicectomy Source: Bailey & Loves Short Practice of Surgery 25th ed • • • Conventional Appendicectomy Laparoscopic Appendicectomy Postoperative Complications
- 17. Conventional Appendicectomy Gridiron incision : right angles to a line joining the ASIS to the umbilicus.Centred on McBurney’s point Lanz incision : 2 cm below the umbilicus centred on the mid- clavicular-midinguinal line 2/3 1/3 2 cm
- 18. ConventionalAppendicectomy Source: Bailey & Loves Short Practice of Surgery 25th ed • Caecum is identified • Base of mesoappendix is clamped in artery forceps, divided, and ligated • The freed appendix is crushed near its junction with the caecum in artery forceps, which is removed and reapplied just distal to the crushed portion • An absorbable ligature is tied around the crushed portion close to the caecum • The appendix is amputated between the artery forceps and the ligature • An absorbable purse-string or ‘Z’ suture may then be inserted into the caecum about 1.25 cm from the base • The stump of the appendix is invaginated while the purse-string or ‘Z’ suture is tied, thus burying the appendix stump
- 19. Source: Bailey & Loves Short Practice of Surgery 25th ed
- 20. Laparoscopic appendicectomy Source: Bailey & Loves Short Practice of Surgery 25th ed • • • • • • • • • • The placement of operating ports may vary according to operator preference and previous abdominal scars. The operator stands to the patient’s left and faces a video monitor placed at the patient’s right foot. A moderateTrendelenburg tilt of the operatingtable The appendix is identify & controlled using a laparoscopic tissue-holding forceps. By elevating the appendix, the mesoappendix is displayed A dissecting forceps is used to create a window in the mesoappendix to allow the appendicular vessels to be coagulated or ligated using a clip applicator. The appendix, free of its mesentery, can be ligated at its base with an absorbable loop ligature,divided, & removed through one of the operating ports. It is not usual to invert the stump of the appendix A single absorbable suture is used to close the linea alba at the umbilicus, and the small skin incisions may be closed with subcuticular sutures. Patients who undergo laparoscopic appendicectomy are likely to have less postoperative pain & to be discharged from hospital and return to activities of daily living sooner than those who have undergone open appendicectomy.
- 22. Source: Bailey & Loves Short Practice of Surgery 25th ed
- 23. Problems Encountered During Appendicectomy Source: Bailey & Loves Short Practice of Surgery 25th ed Problems Management A normal appendix is found Demands careful exclusion of other possible diagnosis Remove the appendix to avoid future diagnostic difficulties The appendix cannot be found Caecum should be mobilised, and the taeniae coli should be traced to their confluence on the caecum before the diagnosis of ‘absent appendix’ is made An appendicular tumour is found Small tumours (< 2.0 cm in diameter) can be removed by appendicectomy Larger tumours should be treated by a right hemicolectomy An appendix abscess is found and the appendix cannot be removed easily Should be treated by local peritoneal toilet, drainage of an abscess and intravenous antibiotics
- 24. Appendix mass Source: Bailey & Loves Short Practice of Surgery 25th ed • If an appendix mass is present & the condition of the patient is satisfactory, the standard treatment is the conservative • Careful recording of the patient’s condition and the extent of the mass should be made and the abdomen regularly re-examined. • mark the limits of the mass using a skin pencil. • Temperature and pulse rate should be recorded 4- hourly and a fluid balance record maintained • A contrast-enhanced CT examination of the abdomen should be performed and antibiotic therapy instigated. • An abscess, if present, should be drained radiologically. • Clinical deterioration or evidence of peritonitis is an indication for early laparotomy. • Clinical improvement is usually evident within 24–48 hours
- 25. Criteria for stopping conservative treatment of an appendix mass Source: Bailey & Loves Short Practice of Surgery 25th ed • A rising pulse rate • Increasing or spreading abdominal pain • Increasing size of the mass
- 27. Postoperative Complications Source: Bailey & Loves Short Practice of Surgery 25th ed • Wound infection • Intra-abdominal abscess • Adhesive intestinal obstruction • Rare • • • • • Ileus Respiratory – pneumonitis or collapse Venous thrombosis and embolism Portal pyaemia (pylephlebitis) Faecal fistula
- 28. Other causes of acute appendicitis • • Recurrent Acute Appendicitis Neoplasms of the Appendix
- 29. Recurrent Acute Appendicitis Source: Bailey & Loves Short Practice of Surgery 25th ed • Widely known but unfavourable • Not uncommon for patients to attribute such attacks to ‘biliousness’ or dyspepsia • Attacks vary in intensity and may occur every few months • Through history, patient might have had milder but similar attacks of pain showing fibrotic appendix indicative of previous inflammation • Chronic appendicitis, per se, does not exist; however, there is evidence of altered neuroimmune function in the myenteric nerves of patients with so called recurrent appendicitis (Büchler)
- 31. RESEARCH Active observation versus interval appendicectomy after successful non- operative treatment of an appendix mass in children (CHINA study): an open-label, randomised controlled trial
- 32. EVIDENCE BASED PRACTICE Computed Tomography Utilization for the Diagnosis of Acute Appendicitis in Children Decreases With a Diagnostic Algorithm