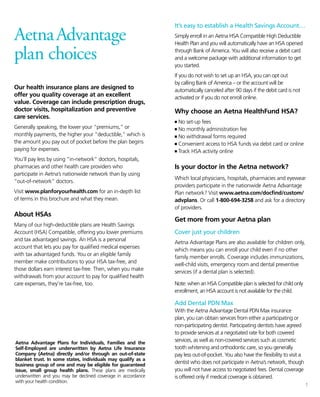
1) This plan has no deductible for in-network services and a $0 copay for primary care visits. Coinsurance is 30% in-network and 50% out-of-network, with a $7,500 individual/$15,000 family out-of-pocket maximum. Preventive care has a $30 copay in-network.
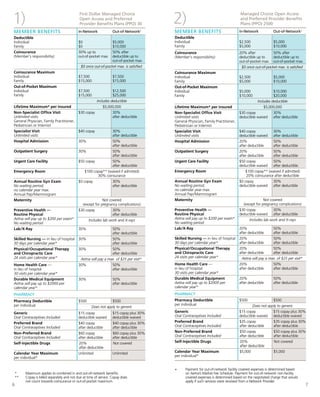
2) This plan has a $2,500/$5,000 deductible and 20% coinsurance in-network and 50% out-of-network. The out-of-pocket maximum is $5,000/$10,000 in-network and $10,000/$20,000 out-of-network. Primary care